Full Report (January 7, 2008)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Municipal Register of Cultural Heritage Resources Designated Under the Ontario Heritage Act
Municipal Register of Cultural Heritage Resources Designated Under the Ontario Heritage Act Designated Properties Last Updated: 2021 1 Background In Ontario, the conservation of cultural heritage resources is considered a matter of public interest. Significant heritage resources must be conserved. The Ontario Heritage Act gives municipalities and the provincial government powers to preserve the heritage of Ontario. The primary focus of the Act is the protection of heritage buildings, cultural landscapes and archaeological sites. The Ontario Heritage Act enables municipalities to designate such properties if they hold “cultural heritage value or interest”. Municipal heritage designations are enacted by City Council through the passing of a by-law. Once a property is designated, it gains public recognition as well as a measure of protection from demolition or unsympathetic alteration. Designation helps guide future change to the property so that the cultural heritage value of the property can be maintained. There are two types of designation under the Ontario Heritage Act: designation of individual properties (known as Part IV designation), and designation of unique and important streetscapes, areas or "heritage conservation districts" (known as Part V designation). Any real property that has cultural heritage value or interest can be designated, including houses, barns, factories, cemeteries, parks, bridges, trees, gardens, hedgerows, fences, monuments, churches, woodlots, historic sites and the list goes on. Heritage designation is based on provincially regulated criteria (Ontario Heritage Act, O. Reg. 9/06), which includes design or physical value, historical or associative value, and/or contextual value. Heritage designation can be based on meeting one or more of these three broad criteria. -

Forward Looking Statements
TORSTAR CORPORATION 2020 ANNUAL INFORMATION FORM March 20, 2020 TABLE OF CONTENTS FORWARD LOOKING STATEMENTS ....................................................................................................................................... 1 I. CORPORATE STRUCTURE .......................................................................................................................................... 4 A. Name, Address and Incorporation .......................................................................................................................... 4 B. Subsidiaries ............................................................................................................................................................ 4 II. GENERAL DEVELOPMENT OF THE BUSINESS ....................................................................................................... 4 A. Three-Year History ................................................................................................................................................ 5 B. Recent Developments ............................................................................................................................................. 6 III. DESCRIPTION OF THE BUSINESS .............................................................................................................................. 6 A. General Summary................................................................................................................................................... 6 B. -

BBAC Minutes
BBAC minutes December 15, 2014 - 6:30pm – 8:30pm 16 George Street North (Brampton Safe City Association offices) Attendees: Members: David Laing, Dayle Laing, Stephen Laidlaw, Kevin Montgomery, Lisa Stokes, George Shepperdley, Pauline (Polly) Thornham, John Van West, Erica Duque (Peel Active Transportation) Regrets: Gerald Pyjor, Peter Bolton, Ernst Braendli, Tricia Prato, Jerry Prato, Paola Rico, Chris Spinney, Jason Hammond (Community CarShare) Meeting Started: 6:42 pm Review and approve Motion to approve minutes: George, seconded Kevin – Carried minutes from last meeting Actions arising from previous minutes Brampton City Update David reported that he requested from the Clerk’s Office, a new Councillor representative for BBAC. He heard back that this decision is pending the outcome of the new committees of Council. (New Business) Regional Update Erica reported that Beth Savan’s project will be linked with Peel Region’s Community Based Social Marketing project for efficiencies and cost savings. David suggested that Ranjana Mitra, Executive Director of the Community Environment Alliance, and Uzma Ifan, Community Development Coordinator of the Punjabi Community Health Services might be appropriate partners. Action: David to send Ranjana’s and Uzma’s contact information to Erica. Erica reported she is organizing a “staff only” meeting on February 26th regarding Municipal Liability. The leading liability partner at Gowlings Lafleur Henderson LLP, lawyer Belinda Bain will be presenting on liability and insurance issues for active transportation. (Ms. Bain presented on this topic at the Ontario Bike Summit in Toronto last April.) Dave McLaughlin from MMM Group will be presenting about 1 | P a g e BBAC minutes Ontario Book 18. -

REPORT City Council the Corporation of the City of Brampton
REPORT City Council The Corporation of the City of Brampton Summary On August 13, 2020, in my capacity as Integrity Commissioner, I received a complaint (the “Complaint”) regarding Mayor Patrick Brown (“Mayor Brown”). The Complaint was based on an incident that took place on August 4, 2020, when Mayor Brown attended at the Earnscliffe Recreation Centre ice hockey arena (the “Arena”). The Complaint alleged that Mayor Brown was there to play hockey and that he was not wearing a mask. The Complaint alleged that Mayor Brown had violated Rule 4 (Use of City Property, Services, and Other Resources), Rule 7 (Improper use of Influence), Rule 15 (Discreditable Conduct), and Rule 18 (Failure to Adhere to Council Policies and Procedures) of the City of Brampton’s Code of Conduct for Members of Council (the “Code”). The Complaint also alleged that Mayor Brown had violated the City of Brampton’s Mandatory Face Coverings By-law 135-2020 (the “Mask By-law”), and implied that he had violated the provincial re-opening guidelines passed under the Emergency Management and Civil Protection Act (the “Emergency Orders”) and was involved in changing the City of Brampton’s “Facility Rental” website to cover his actions. Background and Summary I received the Complaint from Aaron Rosenberg, a lawyer representing the Rebel News Network Ltd. (“Rebel News”) and one of its reporters, David Menzies (“Mr. Menzies”). I will refer to them collectively as the “Complainants”. The Complaint included a link to a brief clip of footage taken by Rebel News on August 4, 2020. The Complaint also contained a link to an article published by the Brampton Guardian on August 9, 2020, titled: “Patrick Brown responds to Rebel News video alleging he broke Brampton’s COVID-19 bylaws” (the “Guardian Article”) (Tab 1). -

General Remarks William Osler Health System AGM and Peel Memorial Celebration
General Remarks William Osler Health System AGM and Peel Memorial Celebration Maria Britto, Board Chair, Central West LHIN Wednesday, June 25, 2014 Osler AGM and Peel Memorial Celebration Thank you John and good afternoon everyone. MPP Dhillon, Mayor Fennell, Kay, Matt, special guests, members of the local community… on behalf of the Central West Local Health Integration Network I am so very pleased to be here this afternoon, and to help celebrate such an important milestone in the transformation of Peel Memorial Hospital. The Central West LHIN operates from a simple but profound premise… that the health care needs of local communities are best understood by those who live and work in them. With that said, it was a number of years ago that the Central West LHIN conducted specific work related to both the current and future health care needs of this community. In so doing, the LHIN reached out to engage the local community as an active participant in planning its local health care system. Let me just say… this community responded! There were hundreds of people engaged in sharing their ideas, needs and hopes for the future. And, as a result, the LHIN was able to use this invaluable information to help guide its thinking around what the future of local health care could look like… the possibility of a new health care model that was sustainable, cost-effective and truly integrated for the benefit of residents in local and surrounding communities. Given where we are today, I would suggest this community has had an undeniable impact. -

2003 ANNUAL REPORT 54310 Torstar Cover 3/22/04 9:22 PM Page 1 Page PM 9:22 3/22/04 Cover Torstar 54310 54310 Torstar Cover 3/22/04 9:22 PM Page 3
TORSTAR CORPORATION 2003 ANNUAL REPORT 54310 TorStar Cover 3/22/04 9:22 PM Page 1 54310 TorStar Cover 3/22/04 9:22 PM Page 3 CORPORATE INFORMATION OPERATING COMPANIES – PRODUCTS AND SERVICES TORSTAR DAILY NEWSPAPERS COMMUNITY NEWSPAPERS Metroland Printing, Publishing & Distributing is Ontario’s leading publisher of community newspapers, publishing 63 community newspapers in 106 editions. Some of the larger publications include: Ajax/Pickering News Advertiser Aurora/Newmarket Era-Banner Barrie Advance Brampton Guardian Burlington Post Etobicoke Guardian Markham Economist & Sun TORSTAR IS A BROADLY BASED CANADIAN MEDIA COMPANY. Torstar was built on the foundation of its Mississauga News Oakville Beaver flagship newspaper, the Toronto Star, which remains firmly committed to being a great metropolitan Oshawa/Whitby This Week Richmond Hill Liberal newspaper dedicated to advancing the principles of its long-time publisher, Joseph Atkinson. Scarborough Mirror INTERACTIVE MEDIA DAILY PARTNERSHIPS From this foundation, Torstar’s media presence has expanded through Metroland Printing, Publishing & Distributing, and CityMedia Group, which together include almost 100 newspapers and related services, www.thestar.com Sing Tao principally in Southern Ontario. Torstar has also built a major presence in book publishing through Harlequin, which is a leading global publisher of romance and women’s fiction, selling books in nearly 100 countries and SPECIALTY PRODUCTS eye Weekly in 27 languages. Forever Young Real Estate News Toronto.com Torstar strives to be one of Canada’s premier media companies. Torstar and all of its businesses are Car Guide committed to outstanding corporate performance in the areas of maximizing shareholder returns, advancing Boat Guide City Parent editorial excellence, creating a great place to work and having a positive impact in the communities we serve. -

Recruitment and Classified Advertising in Both Community and Daily Newspapers
Recruitment and &ODVVL¿HG$GYHUWLVLQJ Rate Card January 2015 10 Tempo Avenue, Toronto, Ontario M2H 2N8 tel.: 416.493.1300 fax: 416.493.0623 e:DÀLQGHUV#PHWURODQGFRP www.millionsofreaders.com www.metroland.com METROLAND MEDIA GROUP LTD. AJAX/PICKERING - HAMILTON COMMUNITY METROLAND NEWSPAPERS EDITIONS FORMAT PRESS RUNS 1 DAY 2 DAYS 3 DAYS DEADLINES, CONDITIONS AND NOTES Ajax/ Pickering News Advertiser Wed Tab 54,400 3.86 1.96 Deadline: 2 Business Days prior to publication Thurs Tab 54,400 Alliston Herald (Modular ad sizes only) Thurs Tab 22,500 1.45 1.20 Deadline: 2 Business Days prior to publication Almaguin News Thurs B/S 4,600 0.75 Deadline: 3 Business Days prior to publication Ancaster News/Dundas Star Thurs Tab 30,879 1.25 Deadline: 3 Business Days prior to publication Arthur Enterprise News Wed Tab 900 0.61 Deadline: 3 Business Days prior to publication Barrie Advance/Innisfil/Journal Thurs Tab 63,800 2.95 2.33 Deadline: 2 Business Days prior to publication (Modular ad sizes only) Belleville News Thurs Tab 23,715 Deadline: 2 Business Days prior to publication Bloor West Villager Thurs Tab 34,300 Deadline: 2 Business Days prior to publication Bracebridge Examiner Thurs Tab 8,849 1.40 Deadline: 3 Business Days prior to publication Bradford West Gwillimbury Topic Deadline: 2 Business Days prior to publication - Material & Thurs Tab 10,700 1.00 (Modular ad sizes only) Booking **Process Color add 25%, Spot add 15%, up to $350 Brampton Guardian/ Wed Tab 240,500 Deadline: 2 Business Days prior to publication. -
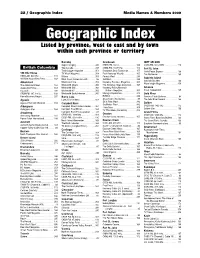
Geographic Index Media Names & Numbers 2009 Geographic Index Listed by Province, West to East and by Town Within Each Province Or Territory
22 / Geographic Index Media Names & Numbers 2009 Geographic Index Listed by province, west to east and by town within each province or territory Burnaby Cranbrook fORT nELSON Super Camping . 345 CHDR-FM, 102.9 . 109 CKRX-FM, 102.3 MHz. 113 British Columbia Tow Canada. 349 CHBZ-FM, 104.7mHz. 112 Fort St. John Truck Logger magazine . 351 Cranbrook Daily Townsman. 155 North Peace Express . 168 100 Mile House TV Week Magazine . 354 East Kootenay Weekly . 165 The Northerner . 169 CKBX-AM, 840 kHz . 111 Waters . 358 Forests West. 289 Gabriola Island 100 Mile House Free Press . 169 West Coast Cablevision Ltd.. 86 GolfWest . 293 Gabriola Sounder . 166 WestCoast Line . 359 Kootenay Business Magazine . 305 Abbotsford WaveLength Magazine . 359 The Abbotsford News. 164 Westworld Alberta . 360 The Kootenay News Advertiser. 167 Abbotsford Times . 164 Westworld (BC) . 360 Kootenay Rocky Mountain Gibsons Cascade . 235 Westworld BC . 360 Visitor’s Magazine . 305 Coast Independent . 165 CFSR-FM, 107.1 mHz . 108 Westworld Saskatchewan. 360 Mining & Exploration . 313 Gold River Home Business Report . 297 Burns Lake RVWest . 338 Conuma Cable Systems . 84 Agassiz Lakes District News. 167 Shaw Cable (Cranbrook) . 85 The Gold River Record . 166 Agassiz/Harrison Observer . 164 Ski & Ride West . 342 Golden Campbell River SnoRiders West . 342 Aldergrove Campbell River Courier-Islander . 164 CKGR-AM, 1400 kHz . 112 Transitions . 350 Golden Star . 166 Aldergrove Star. 164 Campbell River Mirror . 164 TV This Week (Cranbrook) . 352 Armstrong Campbell River TV Association . 83 Grand Forks CFWB-AM, 1490 kHz . 109 Creston CKGF-AM, 1340 kHz. 112 Armstrong Advertiser . 164 Creston Valley Advance. -

Vice President, Philanthropy Executive Brief
Brampton Civic Peel Memorial Etobicoke General Vice President, Philanthropy Executive Brief Table of Contents The Opportunity .............................................................................................................. 2 About the William Osler Health System Foundation ........................................................ 2 About Our Foundation ..................................................................................................... 3 Additional Information ...................................................................................................... 4 The Ideal Candidate ........................................................................................................ 4 Key Responsibilities ........................................................................................................ 5 Biography: Ken Mayhew, President & CEO .................................................................... 6 Board of Directors ........................................................................................................... 7 Organizational Chart ....................................................................................................... 8 Application Process KCI (Ketchum Canada Inc.) has been retained to conduct this search on behalf of William Osler Health System Foundation. For more information about this exciting leadership opportunity, please contact Tara George, Senior Vice President, or Sylvia Kadlick, Senior Consultant, by email at [email protected]. William -

Diagnostics List of Accredited Echocardiography Facilities (609)
Diagnostics Accredited Echocardiography Facilities List of Accredited Echocardiography Facilities (626) # Facility - Site Address City Postal Modalities 1 360 Cardiology and Diagnostic Centre Inc - Syed Najib 106 Humber College Blvd Etobicoke M9V4E4 TTE Stress MPC 2 A Naas MPC - Hagesville 75 Parkview Rd Hagesville N0A1H0 TTE 3 A Naas MPC - Simcoe 365 West St Simcoe N3Y1T7 TTE 4 Abonowara MPC 282 Linwell Rd St Catharines L2N6N5 TTE Stress 5 Accurate Heart Diagnostic Inc - Etobicoke 56 Westmore Dr Etobicoke M9V3Z7 TTE Stress 6 Accurate Heart Diagnostic Inc - Mississauga 3420 Hurontario St Mississauga L5B4A9 TTE Stress 7 Accurate Heart Diagnostic Inc - Pertosa 100 Pertosa Dr Brampton L6X0H9 TTE Stress 8 Accurate Heart Diagnostic Inc - Sandalwood 2945 Sandalwood Parkway Brampton L6R3J6 TTE Stress East 9 Advance Cardiac Services Ltd - Lindsay 65 Angeline St North LINDSAY K9V5N7 TTE 10 Advanced Cardio Diagnostics - Mississauga 77 Queensway West Mississauga L5B1B7 TTE Stress 11 Advanced Cardio Diagnostics - Richmond Hill 10520 Yonge St Richmond Hill L4C3C7 TTE Stress 12 Advanced Cardio Diagnostics - West 3101 Bloor St West Toronto M8X2W2 TTE Stress 13 Advanced Cardiology Inc - Newmarket 16700 Bayview Ave Newmarket L3X1W1 TTE Stress 14 Advanced Cardiology Inc - Owen Sound 1580 20th St East Owen Sound N4K 5P5 TTE Stress 15 Albany Medical Clinic Echocardiography Lab 807 Broadview Ave Toronto M4K2P8 TTE 16 Alexandra Hospital Ingersoll 29 Noxon St Ingersoll N5C1B8 TTE 17 All Health Cardiology Inc 180 Steeles Ave West Vaughan L4J2L1 TTE Stress 18 -
William Osler Health System Turns to Interbit Data's Netdelivery For
case study William Osler Health System turns to Interbit Data’s NetDelivery for COVID-19 emergency mass notification William Osler Health System is a full-service hospital system that serves 1.3 million residents within the Central West Local Health Integration Network in metropolitan Toronto, Canada. It operates three hospitals: Brampton Civic Hospital, Etobicoke General Hospital and the Peel Memorial Centre for Integrated Health and Wellness. The sites provide a comprehensive range of acute care, outpatient services including an expansive Mental Health and Addictions program, and community-based services. In March, due to the growing number of COVID-19 cases in Ontario, the government asked that all Ontario hospitals scale down on non-urgent surgeries and clinical activity to help healthcare staff and physicians preserve capacity for possible elevation in COVID cases that would require hospital care. This left Osler with a daunting challenge: Staff had less than a week to notify every provider that had referred patients for appointments that there were going to be cancellations and no scheduling of new appointments. Faced with this unprecedented demand, Osler staff quickly realized they had no way to easily notify all the providers from outside clinics, some of them many hundreds of miles away, about the cancellations. The health system had a paging system to send out mass communications to internal staff members, but no way of communicating externally to the more than 5,800 providers who refer patients to its hospitals. The only option was to manually contact each individual clinic by phone — a process that likely would entail assigning four or five employees to look up contact information and place calls full-time for at least a week, and then hope that staff at the mostly shuttered clinics were monitoring their voicemails. -

City Council Item I6-1 for September 12, 2012
BRAMPTON ""'-' „J22 bmmpton.ca FlOWef City The Corporation of the City of Brampton Date: August 27,2012 BRAMPTON CITY COUNCIL File: M25-PMH DATEiSephuMr i2( fog Subject: Agreement for the Use of a Municipal Grant for the New Peel Memorial Centre for Integrated Health and Wellness at 20 Lynch Street, Brampton, Ontario (Formerly Peel Memorial Hospital) Contact: Mo Lewis, Commissioner of Financial and Information Services (Tel: 905 874-2250) Dennis Cutajar, Commissioner of Economic Development and Communications (Tel: 905-874-2698) OVERVIEW • At their meeting of August 8, 2012 City Council directed staff to undertake a number of activities in relation to the new Peel Memorial Centre for Integrated Health and Wellness ("Centre") proposed by the William Osier Health System ("Osier"). These activities have been completed and the results are contained in this report. • On Tuesday August 14, 2012, City staff met with management staff from OSLER to discuss the principles of a grant Agreement between the City and OSLER and to discuss process, timelines/milestones. • Following this meeting, City and Osier staff worked together to prepare a draft Agreement directing the use of a S60 million municipal grant towards the local share commitment associated with the proposed Centre. • This report recommends that the Mayor and City Clerk be authorized to execute the Agreement in a form that is satisfactory to the City Solicitor and content of the Agreement satisfactory to the respective Commissioners. A copy of the draft Agreement can be found in Appendix 1 for Council consideration. RECOMMENDATIONS 1. That the report from the Commissioner of Financial and Information Services and the Commissioner of Economic Development and Communications dated August 27, 2012, to the Council meeting of September 12, 2012, re: Agreement For the Use of a Municipal Grant for the New Peel Memorial Centre for Integrated £6-1-2 Health and Wellness at 20 Lynch Street, Brampton, Ontario (Formerly Peel Memorial Hospital) - Ward 3 (File M25-PMH), be received; and 2.