Short Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
EN SOWP05 for PDF.QXD
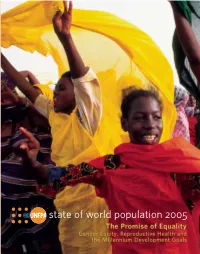
state of world population 2005state of world Goals Health and the Millennium Development Reproductive Gender Equity, of Equality: Promise The UNFPA, the United Nations Population Fund, is an international development agency that promotes the right of every woman, man and child to enjoy a life of health and equal opportunity. UNFPA supports countries in using population data for policies and programmes to reduce poverty and to ensure that every pregnancy is wanted, every birth is safe, every young person is free of HIV/AIDS, and every girl and woman is treated with dignity and respect. UNFPA — because everyone counts. state of world population 2005 United Nations Population Fund 220 East 42nd Street, 23rd Fl. New York, NY 10017 U.S.A. www.unfpa.org ISBN 0-89714-750-2 E/31,000/2005 sales no. E.05.III.H.1 Printed on recycled paper. state of world population 2005 The Promise of Equality Gender Equity, Reproductive Health and the Millennium Development Goals Copyright © UNFPA 2005 United Nations Population Fund Thoraya Ahmed Obaid, Executive Director Contents Chapters 1 Overview ı 6 Partnering with Boys and Men 57 Men’s Roles in Achieving the 2 Strategic Investments: Millennium Development Goals 57 The Equality Dividend 9 The Impact of Gender Roles on Men 58 A Poverty of Opportunity and Choices 9 Reaching Out to Boys and Men 60 Critical Investments, Large Payoffs Reinterpreting Masculinity 60 (Education, Reproductive Health, Economic Rights) ı0 The Formative Years 6ı Reconciling Productive and Reproductive Roles ı5 Accelerating Progress 62 -

A Look from Latin America and the Caribbean on the Millennium Development Goals and the Post-2015 Work
A LOOK FROM LATIN AMERICA AND THE CARIBBEAN ON THE MILLENNIUM DEVELOPMENT GOALS AND THE POST-2015 WORK This document of the Committee of NGOs of CSW for Latin America and the Caribbean was prepared by an independent group designated by the Committee of NGOs of CSW and with contributions from NGOs, networks and experts from the region (see list in Appendix). The purpose of this document is to contribute the voice of civil society to the elaboration of the nal document of CSW. The result of a robust regional consultation, it proposes the continuation of the dialogue before and during CSW. With the support of the Regional Oce of UN Women for the Americas and the Caribbean INTRODUCTION In Latin America and the Caribbean, the impossibility trafficking for the purpose of sexual exploitation, of fulfilling all the MDGs and their targets is evident. among others. The region continues to be the most unequal in the Although two goals, MDG 3 and 5, refer to gender world,1 and although there have been advances in the issues, gender equality was not explicitly included in elimination of poverty, the proposed targets were not the goals. Restricting women’s, adolescents’ and girls’ and will not be achieved. Women’s organizations, rights to only two goals with very high targets, which groups and networks from Latin America and the are far from being achieved by 2015, does not Caribbean are concerned that while many countries acknowledge the interdependency of the goals and report significant advances in the achievement of the the key role of gender equality in development. -

Programming Module on Working with the Health Sector to Address
Programming Module on Working with the Health Sector to Address Violence against Women and Girls Developed by: Jeanne Ward based on the work of Jill Gay and Dina Deligiorgis with contributions from Bonnie Shepard on behalf of UNFPA, Natalia Macdonald and Julie Lafreniere Technical review and feedback provided by: Deborah Billings, PhD, University of South Carolina, Health Promotion, Education and Behavior, Arnold School of Public Health; Women's and Gender Studies Manuela Colombini, London School of Hygiene and Tropical Medicine Suzanne Maman, University of North Carolina at Chapel Hill Brigid McKaw, Medical Director, Family Violence Prevention Center, Kaiser Permanente Partner Agency: Health Module February 2011 INTRODUCTION AND KEY CONCEPTS Why is the Health Sector Critical in Addressing Violence against Women and Girls? o The health sector is a key entry point for survivors. o The health sector has a responsibility to quality of care. o The health sector has a critical role in preventing violence. o Health sector prevention and response programming can reduce the economic and development costs to societies of violence against women. o Health services for survivors are a basic human right. What are Key Elements of a Comprehensive Health Sector Approach to Violence against Women and Girls? o An evidence-base of good practices in health sector approaches to violence against women. o Key theoretical models for building a comprehensive approach. o The “systems” approach to health service delivery. o The “integrated” approach to health service delivery. o Adapting health sector approaches to different contexts and resource levels: from core services to comprehensive care. GUIDING PRINCIPLES Overview of basic principles o Human rights-based approach o Survivor-centred approach o Quality of care approach o Medical ethics of care approach Standards for health service delivery INITIATING OR IMPROVING A NATIONAL HEALTH SECTOR STRATEGY Conduct a situational analysis of the health sector. -

Women out Loud: How Women Living with HIV Will Help the World End AIDS
WOMEN OUT LOUD HOW women LIVING WITH HIV WILL HELP THE WORLD END AIDS REACHING THE TEN TA UNITED POLITICALN ATIONS RGETS OF THE 2011 DECLA GENE RA RAL TION ON A SSEMBL HI Y V AND AIDS WOMEN OUT LOUD HOW women LIVING WITH HIV WILL HELP THE WORLD END AIDS REACHING THE TEN TA UNITED POLITICALN ATIONS RGETS O DECLA GENE RA RAL F THE 2011 TION ON A SSEMBL HI Y V AND AIDS Copyright © 2012 Joint United Nations Programme on HIV/AIDS (UNAIDS) All rights reserved The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of UNAIDS concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. UNAIDS does not warrant that the information published in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use. WHO Library Cataloguing-in-Publication Data Women out loud: How women living with HIV will help the world end AIDS. “UNAIDS / JC2416E” 1.HIV infections – prevention and control. 2.HIV infections – transmission. 3.Acquired immunodeficiency syndrome – prevention and control. 4.Women. I.UNAIDS. ISBN 978-92-9173-995-0 (NLM classification: WC 503.6) CONTENTS REDUCE SEXUAL TRANSMISSION 8 PREVENT HIV AMONG PEOPLE WHO INJECT DRUGS 18 ELIMINATE NEW HIV INFECTIONS AMONG CHILDREN 26 AND KEEP THEIR MOTHERS ALIVE 15 MILLION ACCESSING TREATMENT 34 AVOID TB DEATHS 42 CLOSE THE RESOURCE GAP 50 ELIMINATE GENDER INEQUALITIES 60 ELIMINATE STIGMA AND DISCRIMINATION 68 ELIMINATE HIV-RELATED RESTRICTIONS ON ENTRY, 78 STAY AND RESIDENCE STRENGTHEN HIV INTEGRATION 86 FOREWORD Women may make up half the world’s population, but they do not share it equally. -

A CASE for LEGAL ABORTION WATCH the Human Cost of Barriers to Sexual and Reproductive Rights in Argentina
HUMAN RIGHTS A CASE FOR LEGAL ABORTION WATCH The Human Cost of Barriers to Sexual and Reproductive Rights in Argentina A Case for Legal Abortion The Human Cost of Barriers to Sexual and Reproductive Rights in Argentina Copyright © 2020 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-62313-8462 Cover design by Rafael Jimenez Human Rights Watch defends the rights of people worldwide. We scrupulously investigate abuses, expose the facts widely, and pressure those with power to respect rights and secure justice. Human Rights Watch is an independent, international organization that works as part of a vibrant movement to uphold human dignity and advance the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Sydney, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org AUGUST 2020 ISBN: 978-1-62313-8462 A Case for Legal Abortion The Human Cost of Barriers to Sexual and Reproductive Rights in Argentina Summary ......................................................................................................................... 1 Recommendations ........................................................................................................... 8 To the President of Argentina: ................................................................................................. -

Human Rights of Women Living with HIV in the Americas
Human Rights of Women Living with HIV in the Americas The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners to maximize results for the AIDS response. The Inter-American Commission of Women (CIM) is the main hemispheric policy forum for the promotion of women’s rights and gender equality. Created in 1928 - in recognition of the importance of women’s social inclusion to democratic strengthening and human development in the Americas – CIM was the first inter-governmental organization established to promote women’s human rights and gender equality. The Organization of American States (OAS) brings together the nations of the Western hemisphere to promote democracy, strengthen human rights, foster peace, security and cooperation and advance common interests. The origins of the Organization date back to 1890 when nations of the region formed the Pan American Union to forge closer hemispheric relations. This union later evolved into the OAS and in 1948, 21 nations signed its governing charter. Since then, the OAS has expanded to include the nations of the English- speaking Caribbean and Canada, and today all of the independent nations of North, Central and South America and the Caribbean make up its 35 member states. Human Rights of Women Living with HIV in the Americas Author: Dinys Luciano Co-author: Martín Negrete Editor: Marijo Vázquez Copyright ©2015 UNAIDS and CIM/OAS All rights reserved UNAIDS Regional Support Office for Latin America and Comisión Interamericana de Mujeres (CIM) the Caribbean 1889 F Street NW Gonzalo Crance Street, # 166, Washington, DC, 20006 Ciudad Del Saber, Clayton. -
Fulfilling the UN75 Declaration Expert Series Experts Roundtable 3
Fulfilling the UN75 Declaration Expert Series Experts Roundtable 3 UN75 Declaration commitments #5 We will place women and girls at the center and #11 We will listen to and work with youth Hosted on 1 April 2021 Synthesis of Major Insights & Recommendations On April 1, 2021, a consortium of independent civil society organizations took part in the third roundtable of the “Fulfilling the UN75 Declaration Expert Series,” where thought leaders from global civil society engaged UN Missions and Secretariat officials in a candid dialogue on progress, challenges, and further measures needed to meet two of the twelve commitments presented in the UN75 Declaration. This discussion, sponsored by the Coalition for the UN We Need, Baha’i International Community, the Center for Women’s Global Leadership, Search for Common Ground, Soroptimist International, and the Stimson Center, addressed the UN75 Declaration commitments #5 on “We will place women and girls at the center” and #11 on “We will listen to and work with youth.” The series is intended to take stock of progress toward achieving the twelve UN75 Declaration commitments, introduce alternative institutional, policy, and normative measures for improving implementation, and consider steps for achieving such reforms, including a possible follow-on intergovernmental process as recommended in the Eminent Persons Open Letter signed by 49 former world leaders and UN officials. The expert series aims to contribute insights and concrete proposals for consideration in the Secretary-General's forthcoming (Our Common Agenda) report— expected to be released by September 2021, prior to the UN General Assembly (UNGA) High-Level Week.1 The roundtable’s lead-off speakers included: Azzam Tomeh, Search for Common Ground; Krishanti Dharmaraj, Center for Women’s Global Leadership; Vivek Rai, UN Women; and (moderator) Saphira Rameshfar, Representative to the United Nations, Baha’i International Community. -

UNGASS in SHARP Focus, Issue 4 (175.31 Kb Pdf File)
UNGASS in SHARP Focus Sexual Health and Rights and the 2006 UNGASS Review Editor: Susana T. Fried ([email protected]) Editor’s note: UNGASS in SHARP Focus is an initiative of the OSI/SHARP (sexual health and rights project). Its purpose is to provide information about key sexual health and rights issues and activities arising in the process of the UNGASS review. It is directed both toward those attending the special session and those who are not. There will be 6 issues released. The first two will be issued prior to the review, in order to provide background information about the status of negotiations and planned activities during the UNGASS. Three issues will be released during the UNGASS(May 31 – June 2), at the end of each day. Finally a wrap-up report will be issued following the end of the session. For more information or to share events, strategies and activities, please contact Susana T. Fried at [email protected] or Rachel Thomas, OSI/SHARP at [email protected]. PLEASE FEEL FREE TO SEND INFORMATION ABOUT EVENTS, STRATEGIES AND PROPOSED ACTIONS. WE WILL DO OUR BEST TO DISSEMINATE THE INFORMATION Issue 4: 1 June 2006 Table of contents 1. Update on today’s negotiations – p. 1 2. Press releases and civil society statements in brief - p. 1-3 3. Full text of press releases and civil society statements a. Statement by women’s organizations – pp. 3-5 b. African civil society coalition on AIDS – pp. 5-7 c. Civil Society press release – pp. 7-10 d. Coalition on Sexual and Bodily Rights in Muslim Societies – pp. -

Decisions Denied Women’S Access to Contraceptives and Abortion in Argentina
Human Right Watch June 2005 Vol. 17, No. 1 (B) Decisions Denied Women’s Access to Contraceptives and Abortion in Argentina I. Summary ..................................................................................................................................... 1 II. Recommendations ................................................................................................................... 5 To the Government of Argentina.......................................................................................... 5 To Donors ................................................................................................................................. 8 To the Federation of Argentine Societies of Gynecology and Obstetrics....................... 8 III. Background ............................................................................................................................. 9 Women’s Political, Economic, and Social Status................................................................. 9 Nationalism and Women’s Role as Childbearers...............................................................11 Catholic Church Opposition to Reproductive Rights.......................................................17 IV. Pervasive Barriers in Access to Contraceptives...............................................................21 Domestic and Sexual Violence .............................................................................................21 Misleading, Inaccurate, or Incomplete Information..........................................................26 -

GENDER EQUITY POLICIES in LATIN AMERICA This Spotlight Presents Some of the Key Latin American Organisations Working to Promote Gender Equality in the Region
Spotlight on Organisations ELLA Area: Governance ELLA Theme: Gender Equity Policies SPOTLIGHT ON ORGANISATIONS: GENDER EQUITY POLICIES IN LATIN AMERICA This Spotlight presents some of the key Latin American organisations working to promote gender equality in the region. These national-level organisations - based in Argentina, Brazil, Chile, Colombia, Guatemala, Peru and Mexico - are playing a key role in ensuring the advancement of women in their own countries and in the wider region by promoting the effective realisation of women’s rights, strengthening citizen capacities and developing a gender-based research agenda. Together they cover a variety of issues, from gender-based violence, to health, media and political participation. Feminist Research and Advisory Centre (Centro Feminista de Estudos e Assessoria) Link: http://www.cfemea.org.br/ Areas of Expertise: Feminism, sexual and reproductive rights, labour and social rights, violence against women, political participation Key Activities: Government lobbying, research, strategic partnerships, political education This organisation promotes feminism, human rights, democracy and racial equality in Brazil. Working with a gender approach, this civil society organisation undertakes research aimed at improving political participation of women, promoting sexual and reproductive rights and ending gender-based violence. The organisation also lobbies the Brazilian Congress, and disseminates articles and publications on its areas of expertise. The Centre for the Peruvian Woman Flora Tristán (Centro de la Mujer Peruana Flora Tristán) Link: http://www.flora.org.pe/web2/ Areas of Expertise: Women’s political participation, women’s human rights, women’s empowerment, gender justice and equity, health Key Activities: Legal and health services, community-based programmes, publications, national and regional research, advocacy, campaigning and educational activities The Centre for the Peruvian Woman Flora Tristán is one of the most important organisations working on women’s rights in Peru. -

Violence Against Women and Girls and Its Consequences on Sexual
women’s, gender and rights perspectives in health policies and programmes for change issn 1394-4444 Supplement 2015 to Volume 17 No. 2 2011 Violence against published by the asian-pacific resources & research centre Women and Girls and Its for women and Fundación para Estudio e Investigación de Consequences on Sexual la Mujer and Reproductive Health in Latin America and the published with funding support Caribbean by Notes and References Gender equality and the ability to fully exercise their race, age, ethnic background, sexual the human rights of women and girls, including orientation and gender identity, HIV status, and the power to make decisions regarding their socio economic status, among others. own bodies and live a life free of violence, is still a pending debt for most women and girls In the region, 32 of the 34 countries of the in the Latin American and the Caribbean region. Organization of American States (OAS) have ratified the Inter-American Convention on the 1 UNDP. “About Latin America and the Latin America and the Caribbean is the Prevention, Punishment and Eradication of Caribbean”. Accessed September 22, 2015. most unequal region in the world; ten of the Violence against Women or “Convention of http://www.latinamerica.undp.org/content/ rblac/en/home/regioninfo.html 15 most unequal countries are part of this Belém do Pará” (1994). However, only very region1 and it concentrates seven of 14 most few countries have included in their national 2 ECLAC. Press Release. “Poverty and Indigence Reduction Stalls in Most of Latin violent countries.2 The economic, political legislations the sanction of all forms of gender- American Countries”.January 26, 2015. -

Civil Society Advisory Group to the Core Group
Civil Society Advisory Group to the Core Group BERTHA CECILIA GARCIA CIENFUEGOS Asociación Regional Mujeres Ingenieras Engineer, Master of Science, mention Natural Resources, National University of Cajamarca, has followed studies in scientific research at CAEU-OEI, University of Oviedo-Spain, with AECID scholarship, and Disaster Risk Reduction-DRR at Universidad San Carlos, Guatemala and Florida University-USA, with USAID / OFDA scholarship. CONCYTEC associate researcher, with extensive experience in plant taxonomy, biodiversity, environment, water, sanitation, DRR, climate change and resilient ecosystems; She has 16 years of university teaching experience and has represented in 9 countries as Lecturer in Science Congress. Recognition by Women`s Environment & Development Organizations as women force in defense of environment; currently, Vice President of the Peruvian chapter of the Organization for Women in Science for the Development World-OWSD, from where she continues to contribute to the science and technology of the country and Latin America; In addition to this deployment of intellectual abilities, Master Garcia has formed a family with her husband and children. CHIDI KING International Trade Union Confederation Chidi is the Director of the Equality Department at the International Trade Union Confederation (ITUC), the umbrella organisation for trade union national centres worldwide. She leads the implementation of policies adopted by the ITUC Congress and governing bodies as regards equality. She developed and led the ITUC campaign to secure a Convention to address gender-based violence and harassment in the world of work. She also led on behalf of the ITUC on the negotiations of the Violence and Harassment Convention and Recommendation 2019 (C190 and R206) at the International Labour Conference of the ILO, providing the secretariat to the Workers’ Group.