Barium Enema Water Soluble Contrast Enema
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Intravenous Therapy Procedure Manual
INTRAVENOUS THERAPY PROCEDURE MANUAL - 1 - LETTER OF ACCEPTANCE __________________________________________ hereby approves (Facility) the attached Reference Manual as of _____________________. (Date) The Intravenous Therapy Procedure Manual will be reviewed at least annually or more often when deemed appropriate. Revisions will be reviewed as they occur. Current copies of the Intravenous Therapy Procedure Manual shall be maintained at each appropriate nursing station. I have reviewed this manual and agree to its approval. __________________________ (Administrator) __________________________ (Director of Nursing) __________________________ (Medical Director) - 2 - TABLE OF CONTENTS TABLE OF CONTENTS INTRODUCTION A. Purpose 1 B. Local Standard of Practice 1 RESPONSIBILITIES A. Responsibilities: M Chest Pharmacy 1 B. Responsibilities: Administrator 1 C. Responsibilities: Director of Nursing Services (DON/DNS) 1 D. Skills Validation 2 AMENDMENTS GUIDELINES A. Resident Candidacy for IV Therapy 1 B. Excluded IV Medications and Therapies 1 C. Processing the IV Order 1 D. IV Solutions/Medications: Storage 2 E. IV Solutions/Medications: Handling 3 F. IV Solutions and Supplies: Destroying and Returning 4 G. IV Tubing 5 H. Peripheral IV Catheters and Needles 6 I. Central Venous Devices 7 J. Documentation and Monitoring 8 K. IV Medication Administration Times 9 L. Emergency IV Supplies 10 I TABLE OF CONTENTS PROTOCOLS A. IV Antibiotic 1 1. Purpose 2. Guidelines 3. Nursing Responsibilities B. IV Push 2 1. Purpose 2. Guidelines C. Anaphylaxis Allergic Reaction 4 1. Purpose 2. Guidelines 3. Nursing Responsibilities and Interventions 4. Signs and Symptoms of Anaphylaxis 5. Drugs Used to Treat Anaphylaxis 6. Physician Protocol PRACTICE GUIDELINES A. Purpose 1 B. Personnel 1 C. Competencies 1 D. -

Rectal Suppository & Enema Administration to Administration Unlicensed Assistive Personnel (UAP) Module/Skill Checklist
Delegation of Medication Rectal Suppository & Enema Administration to Administration Unlicensed Assistive Personnel (UAP) Module/Skill Checklist Objective At the completion of this module, the UAP should be able to administer rectal suppository & enema medications. NOTE: 1) The RN or LPN is permitted to delegate ONLY after application of all components of the NCBON Decision Tree for Delegation to UAP and after careful consideration that delegation is appropriate: a) for this client, b) with this acuity level, c) with this individual UAP’s knowledge and experience, and d) now (or in the time period being planned). 2) Successful completion of the “Infection Control” module by the UAP should be documented prior to instruction in medication administration by this or ANY route. Procedure for: SUPPOSITORY 1. Perform skills in General Medication Administration Checklist. 2. Provide privacy. Have client void before procedure. 3. Put on clean gloves. 4. Position the client on their left (preferred) side with the top leg bent slightly. 5. Remove the foil or wrapper from the suppository, if present. 6. Apply a small amount of lubricant to the suppository and your gloved index finger on your dominant hand – the hand holding the suppository. 7. Separate the buttocks with your gloved, non dominant hand. 8. Ask the client to breathe slowly and deeply through the mouth. 9. Place tip of suppository against anus and gently insert the suppository about 4- inches along the rectal wall. Avoid putting the suppository in stool. 10. After removing your finger, squeeze buttocks together for a few minutes to help client hold in the suppository for as long as possible. -

Injection Technique 1: Administering Drugs Via the Intramuscular Route
Copyright EMAP Publishing 2018 This article is not for distribution except for journal club use Clinical Practice Keywords Intramuscular injection/ Medicine administration/Absorption Practical procedures This article has been Injection technique double-blind peer reviewed Injection technique 1: administering drugs via the intramuscular route rugs administered by the intra- concerns that nurses are still performing Author Eileen Shepherd is clinical editor muscular (IM) route are depos- outdated and ritualistic practice relating to at Nursing Times. ited into vascular muscle site selection, aspirating back on the syringe Dtissue, which allows for rapid (Greenway, 2014) and skin cleansing. Abstract The intramuscular route allows absorption into the circulation (Dough- for rapid absorption of drugs into the erty and Lister, 2015; Ogston-Tuck, 2014). Site selection circulation. Using the correct injection Complications of poorly performed IM Four muscle sites are recommended for IM technique and selecting the correct site injection include: administration: will minimise the risk of complications. l Pain – strategies to reduce this are l Vastus lateris; outlined in Box 1; l Rectus femoris Citation Shepherd E (2018) Injection l Bleeding; l Deltoid; technique 1: administering drugs via l Abscess formation; l Ventrogluteal (Fig 1, Table 1). the intramuscular route. Nursing Times l Cellulitis; Traditionally the dorsogluteal (DG) [online]; 114: 8, 23-25. l Muscle fibrosis; muscle was used for IM injections but this l Injuries to nerves and blood vessels muscle is in close proximity to a major (Small, 2004); blood vessel and nerves, with sciatic nerve l Inadvertent intravenous (IV) access. injury a recognised complication (Small, These complications can be avoided if 2004). -

22428 Moxifloxacin Statisical PREA
U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research Office of Translational Science Office of Biostatistics S TATISTICAL R EVIEW AND E VALUATION CLINICAL STUDIES NDA/Serial Number: 22,428 Drug Name: Moxifloxacin AF (moxifloxacin hydrochloride ophthalmic solution) 0.5% Indication(s): Treatment of bacterial conjunctivitis Applicant: Alcon Pharmaceuticals, Ltd. Date(s): Letter date:21 May 2010; Filing date: 18 June, 2010; PDUFA goal date: 19 November 2010 Review Priority: Priority Biometrics Division: Anti-infective and Ophthalmology Products Statistical Reviewer: Mark. A. Gamalo, Ph.D. Concurring Reviewers: Yan Wang, Ph.D. Medical Division: Anti-infective and Ophthalmology Products Clinical Reviewer: Lucious Lim, M.D. Project Manager: Lori Gorski Keywords: superiority, Moxifloxacin hydrochloride ophthalmic solution, bacterial conjunctivitis, bulbar conjunctival injection, conjunctival discharge/exudate TABLE OF CONTENTS TABLE OF CONTENTS................................................................................................................ 2 LIST OF TABLES.......................................................................................................................... 3 1. EXECUTIVE SUMMARY ...................................................................................................... 4 1. 1 Conclusions and Recommendations..................................................................................... 4 1. 2 Brief Overview of Clinical Studies ..................................................................................... -

Bowel Preparation Instructions Fleet Enema
66 BOWEL PREPARATION INSTRUCTIONS FLEET ENEMA Please read these instructions before you have your enema and follow carefully. If you need more advice before using the enema, please telephone the Endoscopy Unit on Tel: 01246 512197 You have been given a phosphate enema, which should be kept and used at room temperature. This is to be used on the day you are coming to hospital for your flexible sigmoidoscopy procedure. Instructions: • The enema must be given at least one hour before you leave home to attend hospital. e.g. if your appointment is at 2.00pm and you will be leaving at 1.30pm you must give the enema at 12.30pm. • To give the enema, you need to lie down on your side with both knees bent and pulled up towards your chest. • Remove the enema cap and throw it away. • Relax and gently insert the full length of the nozzle into your rectum (back passage). • Do this without using undue force. The tip of the nozzle is already lubricated to make insertion easier • Squeeze the bottle until it is completely empty. The bottle may be rolled up (like a tube of toothpaste) ensure it empties. Then gently withdraw the bottle while still squeezing to keep it rolled up. • Hold the liquid in your back passage for as long as you can (by clenching your buttocks) 66 MAKE SURE YOU ARE CLOSE TO A TOILET AS THE ENEMA WILL RESULT IN A RAPID EMPTYING OF YOUR BOWELS • Return the used enema to its carton and throw away safely in your domestic waste. -

About Your Surgery Pre-Operative Instructions Prior to Surgery Post-Operative Instructions How to Reach Us
www.fpminstitute.com About Your Surgery Pre-operative Instructions Prior to Surgery Post-operative Instructions How to Reach Us www.fpminstitute.com Pre-operative Instructions Please Note Patient Name: Procedure: Vaginal Colpopexy Enterocele / Rectocele Repair A physician at The Institute for Female Pelvic Medicine & Sacral Colpopexy Colpocleisis / Colpectomy Reconstructive Surgery is available for emergencies 24 hours per day. Hysterectomy Removal / Revision Uterosacral Vault Suspension InterStim® Office hours are Monday through Friday, 8 a.m. to 4 p.m. Colporrhaphy Pubovaginal Sling After hours and on weekends, you can leave non-urgent messages Other: that will be returned the next business day. For urgent situations, Surgery Date: the answering service can page the physician on call. Medical Clearance Blood work at Lab Blood work on Admit. You are required to be medically cleared for surgery by your primary care physician and/or cardiologist within 30 days of your scheduled surgery. You have been given a medical clearance form that your physician will need to complete, as well as a script for an EKG and bloodwork. Please contact your physician and schedule your medical clearance appointment for the week of (not before this www.fpminstitute.com date). If your physician sends you to a lab for bloodwork, we suggest you do this at least two to three days before your appointment, but not before the date indicated above. We will need copies of your test results and completed medical clearance form faxed to us at the number on the form at least three (3) business days prior to your surgery. If you have any questions, please contact our nursing department. -

A Study of Effects of Mouthwash on the Human Oral Mucosae: with Special References to Sites, Sex Differences and Smoking
J. Nihon Univ. Sch. Dent., Vol. 39, No. 4, 202-210, 1997 A study of effects of mouthwash on the human oral mucosae: With special references to sites, sex differences and smoking Kayo Kuyama1 and Hirotsugu Yamamoto2 Departments of Public Health1 and Pathology2, Nihon University School of Dentistry at Matsudo (Received8 Septemberand accepted20 September1997) Abstract : In recent years, the use of mouthwash an ingredientof almost all mouthwashesat zero to 23.0 % has become widespread as a part of routine oral (9, 10), was discussed in particular (4, 6-8). In this hygiene. However, there have been no fundamental connection,Gagari et al. (1) pointed out that the exposure studies on the influence of mouthwashes on the human time of ethanol to the oral mucosae by mouthwashing oral mucosae. One hundred and twenty-five subjects was probably longer than that provided by drinking an (50 males and 75 females) were selected for this study. alcoholic beverage. The inflammation and/or The effects of mouthwash was assessed with the use of hyperkeratosis of the hamster cheek pouch caused by exfoliative cytological and cytomorphometric analyses exposure to a commerciallyavailable mouthwash with a of smears obtained from clinically normal upper high ethanol content were examined (11, 12). In a study labium and cheek mucosae before mouthwashing, 30 of human oral mucosae, epithelial peeling, ulceration, s, 10 min and 1 h after mouthwashing. The inflammationand other miscellaneouschanges occurred independent variables examined were oral site, sex in the mucosae as a result of mouthwashing with high- and smoking (smokers versus never-smokers). In all alcoholproducts (13). -
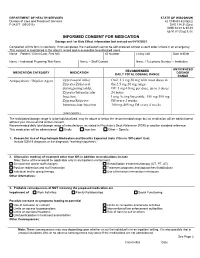
Informed Consent for Medication, Zyprexa
DEPARTMENT OF HEALTH SERVICES STATE OF WISCONSIN Division of Care and Treatment Services 42 CFR483.420(a)(2) F-24277 (09/2016) DHS 134.31(3)(o) DHS 94.03 & 94.09 §§ 51.61(1)(g) & (h) INFORMED CONSENT FOR MEDICATION Dosage and / or Side Effect information last revised on 04/16/2021 Completion of this form is voluntary. If not completed, the medication cannot be administered without a court order unless in an emergency. This consent is maintained in the client’s record and is accessible to authorized users. Name – Patient / Client (Last, First MI) ID Number Living Unit Date of Birth , Name – Individual Preparing This Form Name – Staff Contact Name / Telephone Number – Institution ANTICIPATED RECOMMENDED MEDICATION CATEGORY MEDICATION DOSAGE DAILY TOTAL DOSAGE RANGE RANGE Antipsychotic / Bipolar Agent Zyprexa oral tablet; Oral: 2.5 mg-50 mg with most doses in Zyprexa Zydis oral the 2.5 mg-20 mg range disintegrating tablet; IM: 5 mg-10 mg per dose, up to 3 doses Zyprexa Intramuscular 24 hours Injection; Long Acting Injectable: 150 mg-300 mg Zyprexa Relprevv IM every 2 weeks, Intramuscluar Injection 300 mg-405 mg IM every 4 weeks (olanzapine) The anticipated dosage range is to be individualized, may be above or below the recommended range but no medication will be administered without your informed and written consent. Recommended daily total dosage range of manufacturer, as stated in Physician’s Desk Reference (PDR) or another standard reference. This medication will be administered Orally Injection Other – Specify: 1. Reason for Use of Psychotropic Medication and Benefits Expected (note if this is ‘Off-Label’ Use) Include DSM-5 diagnosis or the diagnostic “working hypothesis.” 2. -

Product Monograph
PRODUCT MONOGRAPH Pr SANDOZ ONDANSETRON ODT Ondansetron Orally Disintegrating Tablets 4 mg and 8 mg ondansetron Manufacturer Standard Pr SANDOZ ONDANSETRON Ondansetron Tablets 4 mg and 8 mg ondansetron (as ondansetron hydrochloride dihydrate) Manufacturer Standard PrONDANSETRON INJECTION USP (ondansetron hydrochloride dihydrate) 2 mg/mL PrONDANSETRON HYDROCHLORIDE DIHYDRATE INJECTION Ondansetron Injection Manufacturer Standard 2 mg/mL Ondansetron (as ondansetron hydrochloride dihydrate) for injection Antiemetic (5-HT3-receptor antagonist) Sandoz Canada Inc. Date of Preparation: 145 Jules-Léger September 26, 2016 Boucherville, Québec, Canada J4B 7K8 Control No.: 198381 Ondansetron by Sandoz Page 1 of 43 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION .......................................................... 3 SUMMARY PRODUCT INFORMATION ................................................................................. 3 INDICATIONS AND CLINICAL USE ....................................................................................... 4 CONTRAINDICATIONS ............................................................................................................ 4 WARNINGS AND PRECAUTIONS .......................................................................................... 5 ADVERSE REACTIONS ............................................................................................................ 7 DRUG INTERACTIONS ............................................................................................................ -

Tax, Price and Cigarette Smoking
i62 Tob Control: first published as 10.1136/tc.11.suppl_1.i62 on 1 March 2002. Downloaded from Tax, price and cigarette smoking: evidence from the tobacco documents and implications for tobacco company marketing strategies F J Chaloupka, K M Cummings, CP Morley, JK Horan ............................................................................................................................. Tobacco Control 2002;11(Suppl I):i62–i72 Objective: To examine tobacco company documents to determine what the companies knew about the impact of cigarette prices on smoking among youth, young adults, and adults, and to evaluate how this understanding affected their pricing and price related marketing strategies. Methods: Data for this study come from tobacco industry documents contained in the Youth and Marketing database created by the Roswell Park Cancer Institute and available through http:// roswell.tobaccodocuments.org, supplemented with documents obtained from http://www. See end of article for tobaccodocuments.org. authors’ affiliations Results: Tobacco company documents provide clear evidence on the impact of cigarette prices on ....................... cigarette smoking, describing how tax related and other price increases lead to significant reductions in smoking, particularly among young persons. This information was very important in developing the Correspondence to: F J Chaloupka, Department industry’s pricing strategies, including the development of lower price branded generics and the pass of Economics (m/c 144), through of cigarette excise tax increases, and in developing a variety of price related marketing efforts, University of Illinois at including multi-pack discounts, couponing, and others. Chicago, 601 South Conclusions: Pricing and price related promotions are among the most important marketing tools Morgan Street, Chicago, IL 60607-7121, USA; employed by tobacco companies. -

How Smoking Affects the Way You Look
How smoking affects the way you look September 2018 (Review date: September 2021) SMOKING AND THE SKIN SMOKING AND WOUND One of the most obvious effects of smoking HEALING is on the appearance of the skin. Skin that Smoking impairs wound healing, delaying recovery is damaged by tobacco smoke typically has and increasing the risk of complications.8 9 The 1 a greyish, wasted appearance , and can be problems that smoking can cause are so serious that affected in several ways. The more a person some plastic surgeons have even declined to perform smokes, the greater the risk of premature cosmetic surgeries on patients who refused to quit wrinkling. One explanation for this is that smoking.10 The Royal College of Anaesthetists advises smoking increases the production of an that quitting smoking any time prior to surgery is enzyme that breaks down collagen in the beneficial.11 skin, causing it to sag.2 Collagen is the main structural protein of the skin and is essential for the skin’s elasticity. SMOKING AND PSORIASIS Psoriasis is a chronic inflammatory skin condition Smokers in their 40s often have as many which, while not life-threatening, can be extremely facial wrinkles as non-smokers in their 60s.3 uncomfortable and disfiguring. Smokers have a two-to- Skin damage caused by smoking may not be threefold higher risk of developing psoriasis than non- immediately visible to the naked eye, but is smokers, with women being at the greatest risk.12 13 still happening, and can start to be detected in one’s 20s or 30s. -
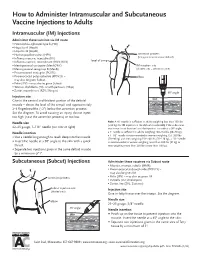
How to Administer Intramuscular and Subcutaneous Vaccines to Adults
How to Administer Intramuscular and Subcutaneous Vaccine Injections to Adults Intramuscular (IM) Injections Administer these vaccines via IM route • Haemophilus influenzae type b (Hib) • Hepatitis A (HepA) • Hepatitis B (HepB) • Human papillomavirus (HPV) acromion process (bony prominence above deltoid) • Influenza vaccine, injectable (IIV) • level of armpit • Influenza vaccine, recombinant (RIV3; RIV4) • Meningococcal conjugate (MenACWY) IM injection site • Meningococcal serogroup B (MenB) (shaded area = deltoid muscle) • Pneumococcal conjugate (PCV13) • Pneumococcal polysaccharide (PPSV23) – elbow may also be given Subcut • Polio (IPV) – may also be given Subcut • Tetanus, diphtheria (Td), or with pertussis (Tdap) • Zoster, recombinant (RZV; Shingrix) 90° angle Injection site skin Give in the central and thickest portion of the deltoid muscle – above the level of the armpit and approximately subcutaneous tissue 2–3 fingerbreadths (~2") below the acromion process. See the diagram. To avoid causing an injury, do not inject muscle too high (near the acromion process) or too low. Needle size Note: A ⅝" needle is sufficient in adults weighing less than 130 lbs (<60 kg) for IM injection in the deltoid muscle only if the subcutane- 22–25 gauge, 1–1½" needle (see note at right) ous tissue is not bunched and the injection is made at a 90° angle; Needle insertion a 1" needle is sufficient in adults weighing 130–152 lbs (60–70 kg); a 1–1½" needle is recommended in women weighing 153–200 lbs • Use a needle long enough to reach deep into the muscle. (70–90 kg) and men weighing 153–260 lbs (70–118 kg); a 1½" needle • Insert the needle at a 90° angle to the skin with a quick is recommended in women weighing more than 200 lbs (91 kg) or thrust.