Pediatric Shoulder AP View (Humeral Head)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -

Scapular Motion Tracking Using Acromion Skin Marker Cluster: in Vitro Accuracy Assessment
Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti, Claudio Rosso, Ara Nazarian, Joseph P. DeAngelis, Arun J. Ramappa & Ugo Della Croce Journal of Medical and Biological Engineering ISSN 1609-0985 J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 1 23 Your article is protected by copyright and all rights are held exclusively by Taiwanese Society of Biomedical Engineering. This e- offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 ORIGINAL ARTICLE Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti • Claudio Rosso • Ara Nazarian • Joseph P. DeAngelis • Arun J. Ramappa • Ugo Della Croce Received: 11 October 2013 / Accepted: 20 March 2014 Ó Taiwanese Society of Biomedical Engineering 2015 Abstract Several studies have recently investigated how estimated using an AMC combined with a single anatom- the implementations of acromion marker clusters (AMCs) ical calibration, the accuracy was highly dependent on the method and stereo-photogrammetry affect the estimates of specimen and the type of motion (maximum errors between scapula kinematics. -

Spontaneous Fracture of the Scapula Spines in Association with Severe Rotator Cuff Disease and Osteoporosis
Central Annals of Musculoskeletal Disorders Case Report *Corresponding author Hans Van der Wall, CNI Molecular Imaging & University of Notre Dame, Sydney, Australia, Tel: +61 2 9736 1040; Spontaneous Fracture of the FAX: +61 2 9736 2095; Email: [email protected] Submitted: 25 March 2020 Scapula Spines in Association Accepted: 07 April 2020 Published: 10 April 2020 ISSN: 2578-3599 with Severe Rotator Cuff Copyright © 2020 Robert B, et al. Disease and Osteoporosis OPEN ACCESS 1 2 3 Breit Robert , Strokon Andrew , Burton Leticia , Van der Wall Keywords H3* and Bruce Warwick3 • Scapular fracture • Rotator cuff arthropathy 1CNI Molecular Imaging, Australia • Osteoporosis 2Sydney Private Hospital, Australia • Scintigraphy 3CNI Molecular Imaging & University of Notre Dame, Sydney, Australia • SPECT/ CT 4Concord Hospital, Australia Abstract We present the case of a 74 year-old woman with diabetes mellitus and established osteoporosis who initially presented with increasing pain and disability of the shoulders. Investigations showed severe rotator cuff disease. This was treated conservatively with physiotherapy and corticosteroid injection into both joints with good pain relief but no improvement in function. She subsequently presented with increasing posterior thoracic pain with plain films reporting no evidence of rib fracture. Bone scintigraphy showed severe rotator cuff disease and degenerative joint disease at multiple sites. The single photon emission computed tomography (SPECT)/ x-ray Computed Tomography (CT) showed bilateral scapula spine fractures of long standing with a probable non-union on the left side. These fractures are rare and difficult to treat when associated with rotator cuff disease. INTRODUCTION Fractures of the scapula spine are rare, with a reported level of dysfunction remained significant with marked restriction frequency of less than twenty cases in the literature [1-8]. -

Distal Clavicle Resection
www.ashevilleortho.com Distal Clavicle Resection Impingement syndrome and associated rotator cuff tears are commonly encountered shoulder problems. This condition is caused when the rotator cuff tendons rub the underside of the acromion bone. Chronic rubbing can lead to a weakening and even tearing of the rotator cuff. Symptoms include pain, weakness and loss of motion. Whether this procedure is done using a scope or through a small incision is dependent on the severity of the tear and the doctor’s preference. The method shown in these animations is with a scope. This content is for informational purposes only. It is not intended to represent actual surgical technique or results. The information is not intended to be a substitute for professional medical advice, diagnosis, treatment or care. Always seek the advice of a medical professional when you have a medical condition. Do not disregard professional medical advice or delay in seeking advice if you have read something in this printout. Copyright © 2013, Understand.com, LLC, All Rights Reserved. Asheville Orthopaedic Associates • (828) 252-7331 www.ashevilleortho.com Distal Clavicle Resection Introduction Impingement syndrome and associated rotator cuff tears are commonly encountered shoulder problems. This condition is caused when the rotator cuff tendons rub the underside of the acromion bone. Chronic rubbing can lead to a weakening and even tearing of the rotator cuff. Symptoms include pain, weakness and loss of motion. Whether this procedure is done using a scope or through a small incision is dependent on the severity of the tear and the doctor’s preference. The method shown in these animations is with a scope. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Radiohamate Impingement After Proximal Row Carpectomy ‘Radiohamate Impingement PRC’
Acta Orthop. Belg., 2020, 86 e-supplement 1, 19-21 CASE REPORT Radiohamate impingement after proximal row carpectomy ‘Radiohamate impingement PRC’ Pieter Caekebeke, Luc De Smet From the Department of Orthopaedics UZ Leuven, Pellenberg, Belgium Radiocarpal impingement after PRC is a well-known from 0% to 18% (5). Radiocarpal and pisiform complication due to impingement of the radial styloid impingement have been described after PRC. The against the radial carpal bones. A less common first is probably due to the proximalization of the impingement syndrome is that of the pisiforme. distal row with impingement of the trapezium/ We describe a radiohamate impingement and its trapezoid against the radial styloid process. The diagnosis and treatment. Based on a case we saw treatment is a radial styloid process resection for at our practice. Diagnosis is bases on standard radiographs and SPECT-CT. The treatment is the first and a pisiformectomy for the latter (3,5). No initially conservative. Surgery is necessary when other impingement syndromes have been described. conservative treatment fails and consists of resectie We present a case of radiohamate impingement of the proximal pole of the hamate. syndrome after proximal row carpectomy. Keywords: Radiohamate ; impingement ; proximal row CASE REPORT carpectomy. A 53-year-old mechanic contacted us 1 year after a work-accident with localized radiocarpal INTRODUCTION pain and swelling. Radiographs showed a stage Proximal row carpectomy (PRC) is a well- two SLAC wrist. (Fig. 1) A PRC with synovectomy established motion-preserving salvage procedure was performed. The following 3 years were for degenerative disorders of the proximal carpal uneventful with no to minimal pain complaints. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
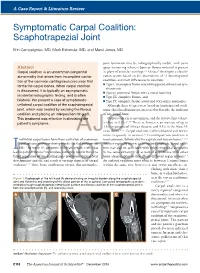
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Lag Screw Fixation for Treatment of an Ulnar Styloid Process Fracture with Antebrachiocarpal Joint Luxation in a Cat
Published online: 2019-06-04 THIEME e32 Case Report Lag Screw Fixation for Treatment of an Ulnar Styloid Process Fracture with Antebrachiocarpal Joint Luxation in a Cat Lindsay A. Parker1 Amy S. Kapatkin2 Mark C. Fuller3 1 Department of Companion Animals, Atlantic Veterinary College, Address for correspondence Lindsay A. Parker, DVM, Atlantic University of Prince Edward Island, Charlottetown, Canada Veterinary College, University of Prince Edward Island, 550 University 2 Department of Surgical and Radiological Sciences, University of Avenue, Charlottetown, PEI, C1A 4P3, Canada California, Davis, CA, United States (e-mail: [email protected]). 3 Fuller Animal Specialty Surgery, Airdrie, AB, Canada VCOT Open 2019;2:e32–e35. Abstract Fracture of the ulnar styloid process can result in clinically debilitating antebrachio- carpal instability. Previously described repair methods include Kirschner wire and figure Keywords of eight tension band wire and/or intramedullary pinning. This case report describes ► feline ulnar styloid surgical repair of a short oblique ulnar styloid process fracture in a cat using two fracture cortical screws placed in lag fashion. Recheck evaluation confirmed lameness-free full ► osteosynthesis return to function with anatomical fracture healing. Introduction acic limb and, on examination under sedation, was found to Lateral styloid process fractures generally require surgical have a marked soft tissue swelling associated with the distal stabilization to avoid carpal instability and to act as a right antebrachium and increased lateral carpal laxity. physical buttress to provide normal joint function.1 Due to Radiographs revealed an antebrachiocarpal joint luxa- the small diameter of the feline distal ulna, these types of tion with an oblique ulnar styloid process fracture (►Fig. -

Conservative Vs. Surgical Management of Ulnar Styloid Fractures Associated with Distal Radius Fractures
CLINICAL RESEARCH Conservative vs. surgical management of ulnar styloid fractures associated with distal radius fractures Cristian Robles, Santiago Iglesias, Christian Allende Nores, Pablo Rotella, Martín Caloia, Miguel Capomassi Orthopedics and Traumatology Department, Sanatorio Allende (Córdoba, Argentina) ABSTRACT Objectives: To evaluate potential differences in clinical and radiological outcomes after surgical versus conservative management of ulnar styloid fractures associated with unstable distal radius fractures treated by locked volar plating. Materials and Methods: This was a multicenter, retrospective and descriptive study including surgical patients treated at four different institutions between 2009 and 2012 for ulnar styloid fractures associated with unstable distal radius fractures. Ulnar styloid fractures were treated con- servatively in group I and surgically in group II. Results: The average follow-up was 56 months. The study included 57 patients divided into two groups (group I [29 cases] and group II [28 cases]). Patients in group II had 2.76 times (95% CI: 1.086; 8.80) more chances of achieving bone union than those in group I. DASH and pain scores, both at rest and during activity, did not show significant differences between the two groups (p = 0.276 and p = 0.877). Group I presented milder ulnar deviation and better strength (p = 0.0194 and p = 0.024). Conclusions: Although patients who underwent surgery for ulnar styloid fractures had 2.76 more chances of achieving bone union than those who received conservative management, there were no significant differences between both groups in subjective evaluations (DASH and pain scores) or when considering the degree of ulnar styloid involve- ment. However, the parameters of strength and ulnar deviation were better in the conservative management group. -

Biceps Anatomical Aberration in a Cadaveric Study
CaseReport32 Indian Journalof Anatomy Volume 7Number 3, May -June 2018 DOI: http://dx.doi.org/10.21088/ija.2320.0022.7318.24 BicepsAnatomicalAberrationinaCadavericStudy ViayAnanth K. Abstract InaroutinecadavericdissectionsinacadavertheshortheadofBicepsBrachiitendon(SBT)showedbifurcated inattachmentwiththebellyofthePronatorTeresmuscleseenalongwithitsusualcourseofattachmentwiththe radialtuberosity. Thiswas seenbilaterally on boththe upperlimbs inthesame bodyduringthe anatomical dissection.erethebicepsbrachiiwasoriginatingfromthelongheadfromthesupraglenoidtuberclefromthe capusularjointandtheshortheadfromthecoracoidprocessofscapula. KeywordsBicepsBrachiiandPronatorTeresMuscleExtrarticularInsertionCadaver. Introduction Intheupperextremitytheanteriorcompartment formstheflexorgroupmusclesofwhichalongwith thecoracobrachialistheBicepsBrachiiplaysamajor roleinflexingthearmsandtheelbowjoint.It compensatestheactionwiththeTricepsBrachiithe posteriorcompartmentmuscleofthebrachiumwhich formstheextensors. Itisalargefusiformmuscleofthatcompartment 3,8andaprimarysupinatoroftheforearm.Biceptal aponeurosis,atriangularbandformedfromthedeep fasciaoriginatesfromthebicepstendon.This aponeurosisgivesprotectiontothecubitalfossa.A thirdhead is also reportedseen posterior to the brachialartery8. Itoriginatesfromlongandshortheadsfrom supraglenoidtubercleandcoracoidsprocessof scapularespectively. Andboththeheadsconvergewiththetwobelles andgetsinsertedintotheposteriorpartofthe tuberosityofradiusbone9. Fi.Rt.SideArm Authors AffiliationLecturer,DepartmentofAnatomy, igure1showsBicepsBrachiiinthefrontof