Minimally Invasive Surgery in Total Hip Arthroplasty
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gluteal Region-II
Gluteal Region-II Dr Garima Sehgal Associate Professor King George’s Medical University UP, Lucknow Structures in the Gluteal region • Bones & joints • Ligaments Thickest muscle • Muscles • Vessels • Nerves Thickest nerve • Bursae Learning Objectives By the end of this teaching session Gluteal region –II all the MBBS 1st year students must be able to: • Enumerate the nerves of gluteal region • Write a short note on nerves of gluteal region • Describe the location & relations of sciatic nerve in gluteal region • Enumerate the arteries of gluteal region • Write a short note on arteries of gluteal region • Enumerate the arteries taking part in trochanteric and cruciate anastomosis • Write a short note on trochanteric and cruciate anastomosis • Enumerate the structures passing through greater sciatic foramen • Enumerate the structures passing through lesser sciatic foramen • Enumerate the bursae in relation to gluteus maximus • Enumerate the structures deep to gluteus maximus • Discuss applied anatomy Nerves of Gluteal region (all nerves in gluteal region are branches of sacral plexus) Superior gluteal nerve (L4,L5, S1) Inferior gluteal nerve (L5, S1, S2) FROM DORSAL DIVISIONS Perforating cutaneous nerve (S2,S3) Nerve to quadratus femoris (L4,L5, S1) Nerve to obturator internus (L5, S1, S2) FROM VENTRAL DIVISIONS Pudendal nerve (S2,S3,S4) Sciatic nerve (L4,L5,S1,S2,S3) Posterior cutaneous nerve of thigh FROM BOTH DORSAL &VENTRAL (S1,S2) & (S2,S3) DIVISIONS 1. Superior Gluteal nerve (L4,L5,S1- dorsal division) 1 • Enters through the greater 3 sciatic foramen • Above piriformis 2 • Runs forwards between gluteus medius & gluteus minimus • SUPPLIES: 1. Gluteus medius 2. Gluteus minimus 3. Tensor fasciae latae 2. -

Diagnosis and Management of Snapping Hip Syndrome
Cur gy: ren lo t o R t e a s e m a u r c e h h Via et al., Rheumatology (Sunnyvale) 2017, 7:4 R Rheumatology: Current Research DOI: 10.4172/2161-1149.1000228 ISSN: 2161-1149 Review article Open Access Diagnosis and Management of Snapping Hip Syndrome: A Comprehensive Review of Literature Alessio Giai Via1*, Alberto Fioruzzi2, Filippo Randelli1 1Department of Orthopaedics and Traumatology, Hip Surgery Center, IRCCS Policlinico San Donato, Milano, Italy 2Department of Orthopaedics and Traumatology, IRCCS Policlinico San Matteo, Pavia, Italy *Corresponding author: Alessio Giai Via, Department of Orthopaedics and Traumatology, Hip Surgery Center, IRCCS Policlinico San Donato, Milano, Italy, Tel: +393396298768; E-mail: [email protected] Received date: September 11, 2017; Accepted date: November 21, 2017; Published date: November 30, 2017 Copyright: ©2017 Via AG, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Background: Snapping hip is a common clinical condition, characterized by an audible or palpable snap of the hip joint. The snap can be perceived at the lateral side of the hip (external snapping hip), or at the medial (internal snapping hip). It is usually asymptomatic, but in few cases, in particular in athletes, the snap become painful (snapping hip syndrome-SHS). Materials and methods: This is a narrative review of current literature, which describes the pathogenesis, diagnosis and treatment of SHS. Conclusion: The pathogenesis of SHS is multifactorial. -
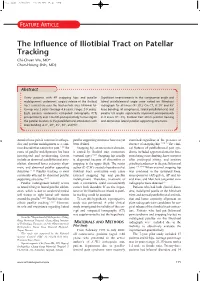
The Influence of Iliotibial Tract on Patellar Tracking Chi-Chuan Wu, MD* Chun-Hsiung Shih, MD†
2wu.qxd 2/10/04 11:19 AM Page 199 FEATURE ARTICLE The Influence of Iliotibial Tract on Patellar Tracking Chi-Chuan Wu, MD* Chun-Hsiung Shih, MD† Abstract Thirty patients with 49 snapping hips and patellar Significant improvements in the congruence angle and malalignment underwent surgical release of the iliotibial lateral patellofemoral angle were noted on Merchant tract contracture over the trochanteric area. Minimal fol- radiograph for all knees (PϽ.01). On CT, at 20° and 45° low-up was 2 years (average 4.6 years, range: 2-9 years). knee bending, all congruence, lateral patellofemoral, and Eight patients underwent computed tomography (CT) patellar tilt angles significantly improved postoperatively preoperatively and 1 month postoperatively to investigate in 8 knees (PϽ.01). Iliotibial tract affects patellar tracking the patellar location in the patellofemoral articulation with and dominates lateral patellar supporting structures. knee bending at 0°, 20°, 45°, 60°, and 90°. Anterior knee pain is common in orthope- patellar supporting structures have not yet examined regardless of the presence or dics and patellar malalignment is a com- been defined. absence of snapping hip.22,24,25 The clini- mon disorder that causes this pain.1-10 The Snapping hip, an uncommon disorder, cal features of patellofemoral pain syn- cause of patellar malalignment has been is caused by iliotibial tract contracture drome included aggravated anterior knee investigated and predisposing factors (external type).20-23 Snapping hip usually pain during stair climbing, knee soreness include an abnormal patellofemoral artic- is diagnosed because of discomfort or after prolonged sitting, and positive ulation, abnormal lower extremity align- snapping in the upper thigh. -

Sacroiliac Joint Dysfunction and Piriformis Syndrome
Classic vs. Functional Movement Approach in Physical Therapy Setting Crista Jacobe-Mann, PT Nevada Physical Therapy UNR Sports Medicine Center Reno, NV 775-784-1999 [email protected] Lumbar Spine Intervertebral joints Facet joints Sacroiliac joint Anterior ligaments Posterior ligaments Pelvis Pubic symphysis Obturator foramen Greater sciatic foramen Sacrospinous ligament Lesser sciatic foramen Sacrotuberous ligament Hip Capsule Labrum Lumbar spine: flexion and extension ~30 total degrees of rotation L1-L5 Facet joints aligned in vertical/saggital plane SI joints 2-5 mm in all directions, passive movement, not caused by muscle activation Shock absorption/accepting load with initial contact during walking Hip Joints Extension 0-15 degrees 15% SI joint pain noted in chronic LBP patients Innervation: L2-S3 Classic signs and symptoms Lower back pain generally not above L5 transverse process Pain can radiate down posterior thigh to posterior knee joint, glutes, sacrum, iliac crest sciatic distribution Pain with static standing, bending forward, donning shoes/socks, crossing leg, rising from chair, rolling in bed Relief with continuous change in position Trochanteric Bursitis Piriformis Syndrome Myofascial Pain Lumbosacral Disc Herniation and Bulge Lumbosacral Facet Syndrome J. Travell suspects Si joint pain may causes piriformis guarding and lead to Piriformis syndrome… Tenderness to palpation of PSIS, lower erector spinae, quadratus lumborum and gluteal muscles Sometimes positive SLR Limited hip mobility -

Anatomy of the Lateral Retinaculum
Anatomy of the lateral retinaculum Introduction The lateral retinaculum of the knee is not a distinct anatomic structure but is composed of various fascial structures on the lateral side of the patella. Anatomical descriptions of the lateral retinaculum have been published, but the attachments, name or even existence of its tissue bands and layers are controversial. The medial patellofemoral ligament on the other hand has been more recently re-examined and its detailed anatomy characterised (Amis et al., 2003, Nomura et al., 2005, Panagiotopoulos et al., 2006, Smirk and Morris, 2003, Tuxoe et al., 2002) The first fascial layer is the fascia lata (deep fascia) that continues to envelop the knee from the thigh (Kaplan, 1957). The fascia lata covers the patellar region but does not adhere to the quadriceps apparatus. The iliotibial tract is integral to the deep fascia and is a lateral thickening of the fascia lata. The anterior expansion of the iliotibial band curves forward. It forms a group of arciform fibres and blends with the fascia lata covering the patella. Fulkerson (Fulkerson and Gossling, 1980) described the anatomy of the knee lateral retinaculum in two distinctly separate layers (Figure 1). The superficial oblique layer originates from the iliotibial band and interdigitates with the longitudinal fibres of the vastus lateralis. The deep layer consist of the deep transverse retinaculum with the epicondylopatellar ligament proximally and the patellotibial ligament distally. The patellotibial ligament proceeds obliquely to attach to the lateral meniscus and tibia. The epicondylopatellar ligament was said to be probably the same 1 ligament described by Kaplan. -

The Muscles That Act on the Lower Limb Fall Into Three Groups: Those That Move the Thigh, Those That Move the Lower Leg, and Those That Move the Ankle, Foot, and Toes
MUSCLES OF THE APPENDICULAR SKELETON LOWER LIMB The muscles that act on the lower limb fall into three groups: those that move the thigh, those that move the lower leg, and those that move the ankle, foot, and toes. Muscles Moving the Thigh (Marieb / Hoehn – Chapter 10; Pgs. 363 – 369; Figures 1 & 2) MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: ANTERIOR: Iliacus* iliac fossa / crest lesser trochanter femoral nerve flexes thigh (part of Iliopsoas) of os coxa; ala of sacrum of femur Psoas major* lesser trochanter --------------- T – L vertebrae flexes thigh (part of Iliopsoas) 12 5 of femur (spinal nerves) iliac crest / anterior iliotibial tract Tensor fasciae latae* superior iliac spine gluteal nerves flexes / abducts thigh (connective tissue) of ox coxa anterior superior iliac spine medial surface flexes / adducts / Sartorius* femoral nerve of ox coxa of proximal tibia laterally rotates thigh lesser trochanter adducts / flexes / medially Pectineus* pubis obturator nerve of femur rotates thigh Adductor brevis* linea aspera adducts / flexes / medially pubis obturator nerve (part of Adductors) of femur rotates thigh Adductor longus* linea aspera adducts / flexes / medially pubis obturator nerve (part of Adductors) of femur rotates thigh MUSCLE: ORIGIN: INSERTION: INNERVATION: ACTION: linea aspera obturator nerve / adducts / flexes / medially Adductor magnus* pubis / ischium (part of Adductors) of femur sciatic nerve rotates thigh medial surface adducts / flexes / medially Gracilis* pubis / ischium obturator nerve of proximal tibia rotates -

Readingsample
Body Contouring Art, Science, and Clinical Practice Bearbeitet von Melvin A. Shiffman, Alberto Di Giuseppe 1st Edition. 2010. Buch. xxviii, 869 S. Hardcover ISBN 978 3 642 02638 6 Format (B x L): 19,3 x 26 cm Gewicht: 2072 g Weitere Fachgebiete > Medizin > Chirurgie > Plastische, Rekonstruktive & Kosmetische Chirurgie Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. Gluteal Contouring Surgery: Aesthetics and Anatomy 2 Robert F. Centeno 2.1 Introduction the gluteus maximus muscle and fat deposits in the superficial fascia. In addition, our erect posture con- tributed to the lumbosacral curve, which is also unique Most plastic surgeons are probably more familiar with to primates. Evolutionary biology suggests that an the anatomy of the face, abdomen, or breasts than with hourglass figure, with a small waist and full buttocks, the anatomy of the gluteal region. Because only a small has historically been associated with female reproduc- percentage of plastic surgery procedures involve the tive potential and physical health across cultures, gen- buttocks, retaining knowledge of its clinical anatomy erations, and ethnicities [1]. A waist-to-hip ratio of 0.7 is not a high priority for most surgeons. This picture, in women remains the ideal of beauty even as different however, is changing as increasing number of patients ethnic groups prefer different gluteal shapes and cur- request body contouring and are increasingly aware of vatures. -

Anatomy and Biomechanics of the Lateral Side of the Knee
To learn more about this study, please click here: http://drlaprade.com REVIEW ARTICLE Anatomy and Biomechanics of the Lateral Side of the Knee Anthony R. Sanchez, II, MD,* Matthew T. Sugalski, MD,* and Robert F. LaPrade, MD, PhD*w external lip of the iliac crest. It inserts onto the Abstract: The posterolateral corner (PLC) of the knee is a anterolateral aspect of the lateral tibial plateau. Its critical element for a functional lower extremity. It consists of an insertion on the tibia was originally described by Gerdy array of complex ligamentous and musculotendinous structures. and later popularized by Segond as the ‘‘tubercle of The primary function of the PLC is to resist varus and external Gerdy.’’ Today it is referred to as ‘‘Gerdy tubercle.’’1 rotation and posterior translation of the tibia. Injuries to these The iliotibial band is divided into superficial, deep, structures can cause significant disability and compromise and capsulo-osseous layers. The superficial layer is first activities of daily living and work, recreational, and sporting encountered after dissecting through the subcutaneous activities. A thorough understanding of the complex anatomy tissues on the lateral aspect of the leg. After splitting the and biomechanics of the PLC will aid the clinician in this first fascial layer (superficial layer) of the iliotibial band, challenging diagnostic and therapeutic problem. The first deeper fibers intimately adhere to the lateral supracondy- section of this paper describes the anatomy of the PLC of the lar tubercle of the femur and blend into the lateral knee focusing on the intricate insertion sites of the individual intramuscular septum. -

The Human Iliotibial Band Is Specialized for Elastic Energy Storage Compared with the Chimp Fascia Lata Carolyn M
© 2015. Published by The Company of Biologists Ltd | The Journal of Experimental Biology (2015) 218, 2382-2393 doi:10.1242/jeb.117952 RESEARCH ARTICLE The human iliotibial band is specialized for elastic energy storage compared with the chimp fascia lata Carolyn M. Eng1,2,*, Allison S. Arnold1, Andrew A. Biewener1 and Daniel E. Lieberman2 ABSTRACT The iliotibial band (ITB) is a unique structure in the human lower This study examines whether the human iliotibial band (ITB) is limb, derived from the fascia lata (FL) of the thigh, which may specialized for elastic energy storage relative to the chimpanzee fascia contribute to locomotor economy (Fig. 1). The ITB is not present in lata (FL). To quantify the energy storage potential of these structures, other apes and thus almost certainly evolved independently in we created computer models of human and chimpanzee lower limbs hominins, but its role in human locomotion is not well understood. based on detailed anatomical dissections. We characterized the Although the most common view of the ITB’s function is to geometryand force–length properties of the FL, tensor fascia lata (TFL) stabilize the pelvis in the frontal plane (Inman, 1947; Kaplan, 1958; and gluteus maximus (GMax) in four chimpanzee cadavers based on Stern, 1972; Gottschalk et al., 1989), we recently created a measurements of muscle architecture and moment arms about the hip musculoskeletal model of the ITB to investigate whether forces and knee. We used the chimp model to estimate the forces and generated by the tensor fascia lata (TFL) or gluteus maximus corresponding strains in the chimp FL during bipedal walking, and (GMax) substantially stretch the ITB during running, storing elastic compared these data with analogous estimates from a model of the energy that is recovered later in the stride (Eng et al., 2015). -
Gluteal Region and Back of Thigh Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Gluteal Region and Back of Thigh Doctors Notes Notes/Extra explanation Editing File Objectives Know contents of gluteal region: Groups of Glutei muscles and small muscles (Lateral Rotators). Nerves & vessels. Foramina and structures passing through them as: 1-Greater Sciatic Foramen. 2-Lesser Sciatic Foramen. Back of thigh : Hamstring muscles. Movements of the lower limb Hip = Thigh Knee=Leg Foot=Ankle Flexion/Extension Flexion/Extension Flexion/Extension Rotation Adduction/Abduction Inversion/Eversion Contents Of Gluteal Region: Muscles / Nerves / Vessels 1- Muscles: • Glutei: 1. Gluteus maximus. 2. Gluteus medius. 3. Gluteus minimus. Abductors: • Group of small muscles (Lateral Rotators): 1. Gluteus medius. 2. Gluteus minimus. 1.Piriformis. Rotators: 2.Obturator internus 1. Obturator internus. 3.Superior gemellus 2. Quadratus femoris. 4.Inferior gemellus Extensor: 5.Quadratus femoris Gluteus maximus. Contents Of Gluteal Region: Muscles / Nerves / Vessels 2- Nerves (All from Sacral Plexus): 1. Sciatic nerve. 2. Superior gluteal nerve. 3. Inferior gluteal nerve. 4. Post. cutaneous nerve of thigh. 5. Nerve to obturator internus. 6. Nerve to quadratus femoris. 7. Pudendal nerve. Contents Of Gluteal Region: Muscles / Nerves / Vessels 3- VESSELS: (all from internal iliac vessels): 1. Superior gluteal 2. Inferior gluteal 3. Internal pudendal vessels. Greater sciatic foreamen: Greater sciatic notch of hip bone is transformed into foramen by: sacrotuberous (between the sacrum to ischial tuberosity) & sacrospinous (between the sacrum to ischial spine ) Structures passing through Greater sciatic foramen : Nerves: Vessels: Greater sciatic foramen Above 1. Superior gluteal nerves, 2. Superior gluteal piriformis vessels. Lesser sciatic foramen muscle. 3. Piriformis muscle. Belew 4. Inferior gluteal nerves 10. -

Iliotibial Band Syndrome
Volume #2, 2020 OrthopedicNotes ILIOTIBIAL BAND SYNDROME Iliotibial band syndrome (ITBS) is the most common cause of lateral knee pain in runners and walkers, with an incidence as high as 12% of all running related overuse injuries.1 ITBS results from recurrent friction of the iliotibial band (ITB) sliding over the lateral femoral epicondyle. ANATOMY AND FUNCTION The iliotibial band is the continuation of the tendinous portion of the tensor fascia latae muscle. It also attaches indirectly to parts of the gluteus medius, gluteus maximus, and the vastus lateralis muscles. An intermuscular septum connects the ITB to the linea aspera femoris until just proximal to the lateral epicondyle of the femur. Distally, the ITB spreads out and inserts on the lateral border of the patella, the lateral patellar retinaculum, and Gerdy’s tubercle of the tibia. The ITB is only free from bony attachment between the superior aspect of the lateral femoral epicondyle and Gerdy’s tubercle.2 A study of runners with ITB symptoms found that the posterior edge of the band was impinging against the lateral epicondyle just after foot strike in the gait cycle.3 The friction first occurred at less than 30° of knee flexion.4 Recurrent rubbing can produce irritation and chronic low-grade inflammation, especially beneath the posterior fibers of the ITB. TREATMENT OF ITB SYNDROME 1. A reduction in stressful activities is necessary to allow the body to catch up with healing. Reduce the repetitive mechanical stress at the lateral femoral condyle. 2. Contract-relax exercises to lengthen shortened iliopsoas, rectus femoris, and gastrocnemius- soleus muscles are performed three times daily in three bouts of a 7-second submaximal contraction followed by a 15-second stretch (contract-relax procedure). -

Intercostal, Ilioinguinal, and Iliohypogastric Nerve Transfers for Lower Limb Reinnervation After Spinal Cord Injury: an Anatomical Feasibility and Experimental Study
LABORATORY INVESTIGATION J Neurosurg Spine 30:268–278, 2019 Intercostal, ilioinguinal, and iliohypogastric nerve transfers for lower limb reinnervation after spinal cord injury: an anatomical feasibility and experimental study *Ahmed A. Toreih, MD,1 Asser A. Sallam, MD, PhD,1 Cherif M. Ibrahim, MD,2 Ahmed I. Maaty, MD,3 and Mohsen M. Hassan4 Departments of 1Orthopedic Surgery and Trauma and 3Physical Medicine, Rheumatology, and Rehabilitation, Suez Canal University Hospitals; 2Department of Anatomy, Suez Canal University; and 4Department of Surgery, Anesthesiology, and Radiology, Faculty of Veterinary Medicine, Suez Canal University, Ismailia, Egypt OBJECTIVE Spinal cord injury (SCI) has been investigated in various animal studies. One promising therapeutic ap- proach involves the transfer of peripheral nerves originating above the level of injury into those originating below the level of injury. The purpose of the present study was to evaluate the feasibility of nerve transfers for reinnervation of lower limbs in patients suffering SCI to restore some hip and knee functions, enabling them to independently stand or even step forward with assistive devices and thus improve their quality of life. METHODS The feasibility of transferring intercostal to gluteal nerves and the ilioinguinal and iliohypogastric nerves to femoral nerves was assessed in 5 cadavers. Then, lumbar cord hemitransection was performed below L1 in 20 dogs, followed by transfer of the 10th, 11th, and 12th intercostal and subcostal nerves to gluteal nerves and the ilioinguinal and iliohypogastric nerves to the femoral nerve in only 10 dogs (NT group). At 6 months, clinical and electrophysiological evaluations of the recipient nerves and their motor targets were performed.