Health Cluster Situation Report #4 Uh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
LPM of Naudero for Web.Pdf
·.. •• NEPL NRUiJERO ENERG'-r' (PVT) LIMITED. Date: May 23, 2014' The Registrar National Electric Power Regulatory Authority Islamabad Subject: Naudero Energy (Pvt.) limited· Modlflca'tlon In Generation LIcense " Dear Sir: In compliance to the NEPRALicensingRegulations 1999 - Modification procedure, we submit the following: 1. Text of proposed modification; Power Purchaser definition may be changed as following: "Power Purchaser" means an entity purchasing electricity from the licensee, pursuant to a Power PurchaseAgreement 2. A statement of the reason In support of the modification; Naudero Energy has earlier entered into a PPA with HESCO (subsequently novated to SEPCO)whileinstalling PhaseI of 16.5 MW, therefore Power Purchaser definition was written as the distribution licensee. The PPAhas expired and now Naudero Energy has received a consent from GoS (Government of Sindh) to purchase electricity for its various department consumers through a wheeling agreement with SEPCOfrom Naudero Energy (draft Wheeling Agreement already submitte1).Slnce GoS is not distributing the electricity and therefore having no distribution license, definition has to be amended as proposed above. 3, A statement of the impact on tariff, quality of service and the performance by the licensee of its obligations under the license There is no impact on tariff, quality of service and the performance due to this modification We shall appreciate that since Wheeling is a new concept in the country, we therefore request NEPRAto guide Naudero Energy for any other modification required to achieve the Wheeling transaction with GoS andSEPC~ . H"dOfflc. ,. Floor. BIodI-3. Hockay Club of PlklslanStadium. Naud.ro. 4leCfUM-h~SO--iP.kll.t ..~,,~)--- Page 10 2 -OIslrlctl:llrkllna------- Tel" +92-21-11166&447 F.x" +e2,213-5880533 Sindh E.mall:lando.nayerluganniiscomnigrou/.Pk I J ' Find enclosed; i) Demand Draft No. -

Asia Briefing, Nr. 74: After Bhutto's Murder
Policy Briefing Asia Briefing N°74 Islamabad/Brussels, 2 January 2008 After Bhutto’s Murder: A Way Forward for Pakistan I. OVERVIEW Musharraf gave up his position of Army Chief on 28 November under U.S. pressure, but the legitimacy of his presidential election remains contested. He Gravely damaged by eight years of military rule, withdrew martial law formally on 15 December, Pakistan’s fragile political system received a major ending the emergency and reviving the constitution. blow on 27 December 2007, when former Prime At the same time, however, he not only did not restore Minister Benazir Bhutto was assassinated. Her the dismissed judges or void the repressive decrees he murder, days before the parliamentary elections had issued but also unilaterally and without any legal scheduled for 8 January 2008 and now postponed to basis proclaimed amendments to the constitution 18 February, put an end to a U.S. effort to broker a purporting to deny the courts and the parliament their power-sharing deal with President Pervez Musharraf constitutional prerogatives to challenge his changes. which the centre-left Pakistan Peoples Party (PPP) leader had already recognised was unrealistic. Her Bhutto’s PPP and the centre-right Muslim League popularity and the belief Musharraf and his allies (Pakistan Muslim League-Nawaz, PML-N) of former were responsible, directly or indirectly, have led to Prime Minister Nawaz Sharif had reluctantly agreed violent countrywide protests. to participate in the 8 January elections, motivated primarily by the desire to expose Musharraf’s Stability in Pakistan and its contribution to wider anti- intention to rig the vote. -

BORN to BE HANGED Praise Fo R the Book
BORN TO BE HANGED Praise fo r the Book While tracing the making of Zulfikar Ali Bhutto-the most popular leader of his people, Dr Syeda Hameed easily identifies him as a self-destroying character in a Greek tragedy. But the chief merit of this book lies in explaining the factors contributing to his meteoric rise and the unravelling of his mind through a reading of his prison letters with Dr Mubashir Hasan's help, and how Bhutto, with a Janus like posture, tried to build a socialist castle on the fo undation of Islamic ideology. The guardians of vested interest were not duped; they hanged him fo r shaking their throne. An eye-opener fo r students of Pakistan's muddled politics. -I.A. Rehman, Human Rights Activist and Political Analyst, Pakistan Syeda Hameed's labour of love, spanning two decades, has flowered into a vivid portrayal of one of the most intriguing public figures of South Asia -Asif Noorani, Senior Journalist and Author, Pakistan BORN TO BE HANGE POLITICAL BIOGRAPHY OF ZULFIKAR ALI BHUTTO SYEDA HAMEED RUPA Published by Rupa Publications India Pvt. Ltd 2017 7/ 16, Ansari Road, Daryaganj New Delhi 110002 Sales Centres: Allahabad Bcngaluru Chennai Hyderabad Jaipur Kathmandu Kolkata Mumbai Copyright «;l Syeda Hameed 2017 Photo courtesy: Author's collection and Sheba George The views and opinions expressed in this book are the author's own and the facts are as reported by her which have been verified to the extent possible, and the publishers arc not in any way liable for the same. All rights reserved. -

Who Assassinated Benazir Bhutto by Shakeel Anjum
WHO ASSASSINATED BENAZIR BHUTTO Shakeel Anjum Reproduced By: Sani Hussain Panhwar Member Sindh Council, PPP Who Assassinated Benazir Bhutto; Copyright © www.bhutto.org 2 Dedicated to the millions, the souls of whom withered and faith in politics diminished with the demise of Benazir Bhutto Who Assassinated Benazir Bhutto; Copyright © www.bhutto.org 3 CONTENTS Preface .. .. .. .. .. .. .. .. .. 8 Chapter-1 Benazir Bhutto — A Profile .. .. .. .. .. 12 Chapter-2 The Return of Benazir Bhutto .. .. .. .. .. 17 Euphoria and Hope .. .. .. .. .. .. 17 Suicide Attack & Aftermath .. .. .. .. .. 19 Condemnation & Blame .. .. .. .. .. .. 20 BB Speaks her Mind Out .. .. .. .. .. .. 21 SIG’s Technical Report .. .. .. .. .. .. 21 Chapter-3 Destiny Plays It’s Role .. .. .. .. .. .. 24 Threats and Fears .. .. .. .. .. .. .. 24 Defiant to the Last .. .. .. .. .. .. .. 24 The Assassins Strike .. .. .. .. .. .. 25 Pistol ‘Norinco’ Used to Shoot Benazir Bhutto .. .. .. 26 History .. .. .. .. .. .. .. .. 27 Autopsy Not Allowed .. .. .. .. .. .. 27 The Medical Report .. .. .. .. .. .. 28 Medical Report Rejected .. .. .. .. .. .. 32 Violence Erupts .. .. .. .. .. .. .. 32 International Media Smells Rat .. .. .. .. .. 33 Fear Becomes True .. .. .. .. .. .. .. 36 The Zia Remnants .. .. .. .. .. .. .. 38 Chapter-4 Investigations .. .. .. .. .. .. .. .. 39 JIT Constituted .. .. .. .. .. .. .. .. 39 Mysterious Factors .. .. .. .. .. .. .. .. 40 The Malicious FIR .. .. .. .. .. .. .. .. 44 Demand of FIR Against Rehman Malik Ignored .. .. .. 45 Chapter-5 Twist in The -

Was Bhutto Killed Before Hanging by Sadiq Jafri
Was Bhutto killed before hanging? Sadiq Jafri Reproduced By: Sani Hussain Panhwar Member Sindh Council, PPP Was Bhutto Killed before hanging Copyright © www.bhutto.org 1 Dedicated To My son, bahawal, who may see the dawn of freedom of expression, when he grows up. Was Bhutto Killed before hanging Copyright © www.bhutto.org 2 Author’s Note Completing this work was a herculean task given the fierce antagonism of our ubiquitous Intelligence agencies. In fact many developments occurred as this piece was going to the press. For one, shortly before the printing began, an interview, with Murtaza Bhutto was splashed across the pages of the News, covering three pages. After the forceful projection of that interview, it would be an uphill task for me to convince readers about the antecedents --- or the lack of them of the AZO, to the public. It is amid these constraints that I have after all got the work ready for the reader’s consumption. I hope now the credibility of the product of the sweat of my brow shall find favour with all those who seek the truth. Was Bhutto Killed before hanging Copyright © www.bhutto.org 3 Contents Introduction by “Zeno” .. .. .. .. .. .. .. 6 The controversy .. .. .. .. .. .. .. .. 7 Geri Arbab .. .. .. .. .. .. .. .. 13 Imprisonment .. .. .. .. .. .. .. .. 16 Old jail .. .. .. .. .. .. .. .. .. 19 Hypothesis .. .. .. .. .. .. .. .. 21 Gen Chishti .. .. .. .. .. .. .. .. 25 The lieutenant .. .. .. .. .. .. .. .. 27 Error .. .. .. .. .. .. .. .. .. 33 The jailors .. .. .. .. .. .. .. .. .. 37 Roger, Roger, Black Horse Over! .. .. .. .. .. .. 43 Executioners execute execution .. .. .. .. .. .. 52 Finish it !!! .. .. .. .. .. .. .. .. .. 54 Top secret .. .. .. .. .. .. .. .. .. 56 The burial .. .. .. .. .. .. .. .. .. 64 Shaheed Baba .. .. .. .. .. .. .. .. 68 Janaza .. .. .. .. .. .. .. .. .. 74 Eyewitnesses .. .. .. .. .. .. .. .. 75 The mark .. .. .. .. .. .. .. .. 76 Justice .. .. .. .. .. .. .. .. .. 82 Was Bhutto Killed before hanging Copyright © www.bhutto.org 4 Forensic . -
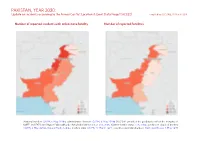
PAKISTAN, YEAR 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 25 March 2021
PAKISTAN, YEAR 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 25 March 2021 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, 6 May 2018a; administrative divisions: GADM, 6 May 2018b (ACCORD amended the geodata to reflect the merging of NWFP and FATA into Khyber Pakhtunkhwa); China/India border status: CIA, 2006; Kashmir border status: CIA, 2004; geodata of disputed borders: GADM, 6 May 2018a; Natural Earth, nodate; incident data: ACLED, 12 March 2021; coastlines and inland waters: Smith and Wessel, 1 May 2015 PAKISTAN, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Protests 8109 1 11 Conflict incidents by category 2 Battles 270 173 519 Development of conflict incidents from 2012 to 2020 2 Riots 191 20 39 Violence against civilians 113 75 95 Methodology 3 Explosions / Remote 100 50 150 Conflict incidents per province 4 violence Strategic developments 29 0 0 Localization of conflict incidents 4 Total 8812 319 814 Disclaimer 6 This table is based on data from ACLED (datasets used: ACLED, 12 March 2021). Development of conflict incidents from 2012 to 2020 This graph is based on data from ACLED (datasets used: ACLED, 12 March 2021). 2 PAKISTAN, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Methodology Geographic map data is primarily based on GADM, complemented with other sources if necessary. -

Zulfikar Ali Bhutto
Zulfikar Ali Bhutto Recollections and Remembrances Foreword Mohtrama Benazir Bhutto Reproduced By: Sani Hussain Panhwar Member Sindh Council, PPP Zulfikar Ali Bhutto, Recollections and Remembrances; Copyright © www.bhutto.org 1 Dedicated to The people of Pakistan Shaheed Bhutto’s source of strength Zulfikar Ali Bhutto, Recollections and Remembrances; Copyright © www.bhutto.org 2 TABLE OF CONTENTS FOREWORD .. .. .. .. .. .. .. .. 6 ACKNOWLEDGEMENT .. .. .. .. .. .. .. 9 HE WAS A LOVING HUSBAND Begum Nusrat Bhutto .. .. .. .. .. 10 A HAPPY MAN ALWAYS Ameer Begum .. .. .. .. .. .. 22 A SISTER SPEAKS Mrs. Munawar -ul-Islam .. .. .. .. .. 28 MONJO PAYARO CHACHO Miss Shabnam Bhutto .. .. .. .. .. 34 AN IDEAL OF MILLIONS Mr. Tariq Islam .. .. .. .. .. .. 39 EARLY YEARS. Mr. Omar Kureshi .. .. .. .. .. .. 50 AN UNCOMPROMISING LAWYER Mr. G. H. Abbasi .. .. .. .. .. .. 53 COMMUNICATION WITH THE MASSES WAS HIS KEY Haji Nazar Muhammad Leghari .. .. .. .. 58 MERA SAHIB Mr. Abdul Qayum Khan .. .. .. .. .. 63 THE MEMOIRS Mr. Dost Mohammad .. .. .. .. .. 67 IN THE LINE OF DUTY Mr. Mohammed Urs .. .. .. .. .. 72 HOME SWEET HOME Mr. Usman Flashman .. .. .. .. .. 76 Zulfikar Ali Bhutto, Recollections and Remembrances; Copyright © www.bhutto.org 3 MY LEADER. Mr. Muhammad Hanif Khan .. .. .. .. 81 MR BHUTTO AS PRIME MINISTER Major Gen. (Rd) Nasirullah Khan Babar .. .. .. 89 BHUTTO AS A REFORMER Sheikh Muhammad Rasheed .. .. .. .. 99 MY FIRST MEETING WITH SHAHEED Sheikh Rafiq Ahmed .. .. .. .. .. 123 A HOUSEHOLD NAME IN EVERY POOR HOME Mr. Ghias-ud-din Janbaz .. .. .. .. .. 125 THE MAN WHO MEANT BUSINESS Mr. F. K. Bandial .. .. .. .. .. .. 132 IK NARA BANA HEY USKA LAHOO Mr. Habib Jalib .. .. .. .. .. .. 137 HISTORY LIVES IN HIM Mr. Mahmood Sham .. .. .. .. .. 141 WHEN HE “DID NOT” SPEAK ON POLITICS Dr. Kamil Rajpar .. .. .. .. .. .. 145 THEY ARE MY PAKISTAN Mr. Sayeed Humayun Adv . -
Benazir Bhutto
Benazir Bhutto Reconciliation Islam, Democracy, and the West Contents Note to the Reader 1 The Path Back 2 The Battle Within Islam: Democracy Versus Dictatorship, Moderation Versus Extremism 3 Islam and Democracy: History and Practice 4 The Case of Pakistan 5 Is the Clash of Civilizations Inevitable? 6 Reconciliation Afterword Acknowledgments Notes About the Author Credits Copyright About the Publisher Note to the Reader This book was written under extraordinary circumstances. It was my privilege to work with Benazir Bhutto on this project over the last very difficult months. This period of her life included her historic return to Karachi on October 18, 2007, which attracted three million supporters to greet her, and the unsuccessful assassination attempt on her in the early minutes of October 19 that killed 179 people. In the midst of all of this tumult Benazir and I collaborated on the book, at times while Benazir was under house arrest by the Musharraf regime and under the constraints of emergency rule, tantamount to martial law. Despite the events swirling about her and her responsibility of leading Pakistan’s largest political party—the Pakistan Peoples Party—in the parliamentary election campaign, Benazir Bhutto remained focused on Reconciliation: Islam, Democracy, and the West. This book was very important to her, and she threw herself into it with the complete attention and intensity with which she did so many things in her life. Benazir was convinced that the battles between democracy and dictatorship, and between extremism and moderation, were the two central forces of the new millennium. She believed that the message of her cherished religion, Islam, was being politicized and exploited by extremists and fanatics. -

After Bhutto's Murder
Policy Briefing Asia Briefing N°74 Islamabad/Brussels, 2 January 2008 After Bhutto’s Murder: A Way Forward for Pakistan I. OVERVIEW Musharraf gave up his position of Army Chief on 28 November under U.S. pressure, but the legitimacy of his presidential election remains contested. He Gravely damaged by eight years of military rule, withdrew martial law formally on 15 December, Pakistan’s fragile political system received a major ending the emergency and reviving the constitution. blow on 27 December 2007, when former Prime At the same time, however, he not only did not restore Minister Benazir Bhutto was assassinated. Her the dismissed judges or void the repressive decrees he murder, days before the parliamentary elections had issued but also unilaterally and without any legal scheduled for 8 January 2008 and now postponed to basis proclaimed amendments to the constitution 18 February, put an end to a U.S. effort to broker a purporting to deny the courts and the parliament their power-sharing deal with President Pervez Musharraf constitutional prerogatives to challenge his changes. which the centre-left Pakistan Peoples Party (PPP) leader had already recognised was unrealistic. Her Bhutto’s PPP and the centre-right Muslim League popularity and the belief Musharraf and his allies (Pakistan Muslim League-Nawaz, PML-N) of former were responsible, directly or indirectly, have led to Prime Minister Nawaz Sharif had reluctantly agreed violent countrywide protests. to participate in the 8 January elections, motivated primarily by the desire to expose Musharraf’s Stability in Pakistan and its contribution to wider anti- intention to rig the vote. -

Zulfikar Ali Bhutto
ZULFIKAR ALI BHUTTO A MEMOIR By Chakar Ali Junejo Reproduced By: Sani H. Panhwar Member Sindh Council, PPP Zulfikar Ali Bhutto; A Memoir, Copyright © www.bhutto.org 1 Contents Chapter One My People .. .. .. .. .. .. .. .. 7 Chapter Two The Bhuttos .. .. .. .. .. .. .. .. 11 Chapter Three Jan Mohammed Junejo & Sir Shahnawaz Bhutto .. .. 14 Chapter Four My Early Days .. .. .. .. .. .. .. 19 Chapter Five First Meeting With Z. A. Bhutto .. .. .. .. .. 22 Chapter Six Days In London .. .. .. .. .. .. .. 28 Chapter Seven Back Home 1952-57 .. .. .. .. .. .. .. 33 Chapter Eight Pakistan’s Spokesman In The UN .. .. .. .. 38 Chapter Nine Ayub Khan’s Minister .. .. .. .. .. .. 41 Chapter Ten The Kashmir Delegations .. .. .. .. .. .. 47 Chapter Eleven The 1965 War And After .. .. .. .. .. .. 51 Chapter Twelve Revolt Against Ayub .. .. .. .. .. .. 54 Chapter Thirteen The PPP Is Born .. .. .. .. .. .. .. 60 Chapter Fourteen Movement Against Ayub .. .. .. .. .. .. 66 Chapter Fifteen Breaking-Up of Pakistan .. .. .. .. .. .. 73 Chapter Sixteen Bhutto’s Pakistan .. .. .. .. .. .. .. 79 Chapter Seventeen The Martyr .. .. .. .. .. .. .. .. 84 Chapter Eighteen Mr. Bhutto’s Political Legacy .. .. .. .. .. 87 Zulfikar Ali Bhutto; A Memoir, Copyright © www.bhutto.org 2 I dedicate this book to Benazir Bhutto Daughter of Shaheed Zulfikar Daughter of the East Chakar Ali Junejo Zulfikar Ali Bhutto; A Memoir, Copyright © www.bhutto.org 3 INTRODUCTION Mr. Chakar Ali Junejo was a trusted companion of Quaid-i-Awam Zulfikar Ali Bhutto for more than 35 years. He saw him from very close quarters and became a fervent admirer of the Shaheed. In his memoirs he has thrown light on many new and endearing aspects of his friend and leader’s character and personality which make this book a document of historical interest. This biographical volume has a value all its own and we are sure it will be appreciated for that quality by it’s readers. -

A Brief Profile of Larkana
A BRIEF PROFILE OF LARKANA Prepared By, Ikhtiar Ahmed Khoso Regional Business Coordinator Small & Medium Enterprise Development Authority Larkana LARKANA AT GALANCE TABLE OF CONTENTS Location Larkana before partition Role of the City Climate of Larkana Physical Features Educational Institutions Statistics of Larkana city Festivals Agriculture system Irrigation Horticulture Livestock Industries Trade and Trade Center Vocation of Larkana Banks /Financial Institutions Hotels Industrialization in Larkana District Location A glance of the map of Sindh reveals that Larkana, from location point of view enjoys a strategic position. After Karachi it is largest city on the west bank of river Indus in Sindh. It include on an area of 7423sq Km. with a population of 1927066. It lies on 27o 33' North latitude and 65o 16' East longitude. The city is located in upper Sindh at a distance of about 85 km south west of Sukkur. Important towns in the vicinity of Larkana include Dokri, Naudero, Ratodero, Qambar, Bakrani, Shahdadkot, Badah and Miro Khan. Larkana before Partition 'Hujaee nano ta ghum Larkano' if you have the money, then visit Larkana. That's one of the most popular idioms by which Larkana has been described right from its existence. Known to be a poetic city with a romantic aura in the air, Larkana projected a loving feeling despite the fact that it lacked the beauty or precision seen in Shikarpur or Karachi. Larkana has been famous for the Guawa fruit production. But above and all these descriptions, Larkana derives its historical importance from the fact that it is the actual cradle in Sindh to the mother of all civilizations, namely Moen-jo-Daro or the mound of the Dead, which is located in the vicinity of Larkana. -
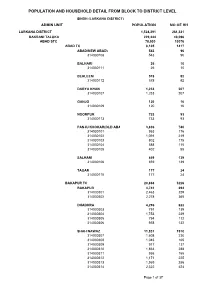
Larkana Blockwise
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (LARKANA DISTRICT) ADMIN UNIT POPULATION NO OF HH LARKANA DISTRICT 1,524,391 261,331 BAKRANI TALUKA 229,444 40,096 ABAD STC 78,530 13076 ABAD TC 8,105 1417 ABAD(NEW ABAD) 543 96 314030108 543 96 BALHARI 26 10 314030111 26 10 BEHLEEM 578 92 314030112 578 92 DARYA KHAN 1,233 207 314030107 1,233 207 GANJO 120 16 314030109 120 16 NOORPUR 733 93 314030113 733 93 PANJU KHOKAR(OLD ABAD) 3,836 740 314030101 953 176 314030102 1,091 219 314030103 802 175 314030104 588 115 314030105 402 55 SALHANI 859 139 314030106 859 139 TAGAR 177 24 314030110 177 24 BAKAPUR TC 20,868 3226 BAKAPUR 4,741 694 314030301 2,463 329 314030302 2,278 365 DHADHRA 4,296 622 314030303 791 139 314030304 1,753 239 314030305 794 112 314030306 958 132 SHAH NAWAZ 11,831 1910 314030307 1,608 230 314030308 1,045 165 314030309 917 137 314030310 1,863 288 314030311 936 155 314030312 1,171 225 314030313 1,969 286 314030314 2,322 424 Page 1 of 37 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (LARKANA DISTRICT) ADMIN UNIT POPULATION NO OF HH MAD BAHU TC 22,760 3808 FARIDABAD 11,967 1855 314030401 2,355 319 314030402 988 194 314030403 439 66 314030404 1,444 236 314030405 798 153 314030406 921 182 314030407 1,351 204 314030408 1,873 341 314030409 1,798 160 MAD BAHU 10,793 1953 314030410 1,280 222 314030411 593 106 314030412 514 63 314030413 954 167 314030414 631 116 314030415 249 43 314030416 879 179 314030417 588 114 314030418 524 85 314030419 481 74 314030420 628 107 314030421 722 123 314030422 636