RHA 2002 May 9 Part 2 Jul 7.Qxd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lands Envrironment Action Fund Toolkit
Lands Environmental Action Fund (LEAF) Manitoba First Nations ENVIRONMENT ECONOMY EMPLOYMENT 2014 CREATING OPPORTUNITIES Creating Environmental Economic Opportunities 2014 Produced by: David Lane, DMCL Environmental Anupam Sharma, Director of Operations, DOTC Robert Daniels, CEO, DOTC This project would not have been possible without generous support and guidance from the Dakota Ojibway Tribal Council, the members of the DOTC Council of Chiefs, and key individuals in their respective communities (Birdtail Sioux First Nation, Dakota Tipi First Nation, Long Plain First Nation, Roseau River Anishinabe First Nation, Sandy Bay Ojibway First Nation, Swan Lake First Nation, and Waywaysecappo First Nation). The information contained within this toolkit is collected from and considered to be part of the public domain. Dakota Ojibway Tribal Council offers this guide without any warranty of any kind, either express or implied. Nor does Dakota Ojibway Tribal Council assume any liability for any damages arising from the use of this product. Dakota Ojibway Tribal Council Head Office Long Plain Reserve #6, Band #287 Room 230, 2nd Floor 5010 Crescent Road West Portage la Prairie, MB Mailing Address: P.O. Box 338 Portage la Prairie, MB R1N 3B7 Website: www.dotc.mb.ca Aboriginal Affairs and Northern Development Canada, through the Lands Environmental Action Fund (LEAF), provided funding for this project. March 2014 Lands Environmental Action Fund (LEAF) 2 Creating Environmental Economic Opportunities 2014 CONTENTS: INTRODUCTION .......................................................................................................... -
Assembly of First Nations Mitigating Climate Change
Assembly of First Nations Mitigating Climate Change Community Success in Developing Energy Efficiency and Renewable Energy Projects Assembly of First Nations Table of Contents Acknowledgements........................................................................................................... 3 Introduction....................................................................................................................... 4 Hupacasath First Nation Micro-hydro Plant..................................................................... 6 Taku River Tlingit Power Station..................................................................................... 8 Nacho Nyak Dun Government House ............................................................................ 10 Xeni Gwet'in First Nation Solar Power Project.............................................................. 11 Rolling River Health Centre CBIP Project..................................................................... 14 Rolling River First Nation Wind-Monitoring Project..................................................... 15 Skownan Home Energy Efficiency Workshop Project................................................... 16 Swan Lake Community Energy Baseline Project........................................................... 17 Swan Lake First Nation Wind-Monitoring Project......................................................... 18 Chakastapaysin and Peter Chapman First Nations Independent Power Production....... 19 Black Lake Denesuline Nation Hydro Project............................................................... -

TRIBAL COUNCIL REPORT COVID-19 TESTING and DISEASE in FIRST NATIONS on RESERVE JULY 26, 2021 *The Reports Covers COVID-19 Testing Since the First Reported Case
TRIBAL COUNCIL REPORT COVID-19 TESTING AND DISEASE IN FIRST NATIONS ON RESERVE JULY 26, 2021 *The reports covers COVID-19 testing since the first reported case. The last TC report provided was on Monday July 19, 2021. DOTC Total Cases 252 Recovered Cases 240 New Cases 1 Active Cases 4 Total Deaths 8 FARHA Total Cases 1833 Recovered Cases 1814 New Cases 1 Active Cases 8 Total Deaths 11 Independent-North Total Cases 991 Recovered Cases 977 New Cases 0 Active Cases 4 Total Deaths 10 This summary report is intended to provide high-level analysis of COVID-19 testing and disease in First Nations on reserve by Tribal Council Region since first case until date noted above. JULY 26, 2021 Independent- South Total Cases 425 Recovered Cases 348 New Cases 36 Active Cases 74 Total Deaths 3 IRTC Total Cases 651 Recovered Cases 601 New Cases 11 Active Cases 38 Total Deaths 12 KTC Total Cases 1306 Recovered Cases 1281 New Cases 1 Active Cases 15 Total Deaths 10 This summary report is intended to provide high-level analysis of COVID-19 testing and disease in First Nations on reserve by Tribal Council Region since first case until date noted above. JULY 26, 2021 SERDC Total Cases 737 Recovered Cases 697 New Cases 14 Active Cases 31 Total Deaths 9 SCTC Total Cases 1989 Recovered Cases 1940 New Cases 11 Active Cases 31 Total Deaths 18 WRTC Total Cases 377 Recovered Cases 348 New Cases 2 Active Cases 25 Total Deaths 4 This summary report is intended to provide high-level analysis of COVID-19 testing and disease in First Nations on reserve by Tribal Council Region since first case until date noted above. -

Since 1985, Stars Has Flown More Than 45,000 Missions Across Western Canada
2019/20 Missions SINCE 1985, STARS HAS FLOWN MORE THAN 45,000 MISSIONS ACROSS WESTERN CANADA. Below are 760 STARS missions carried out during 2019/20 from our base in Winnipeg. MANITOBA 760 Alonsa 2 Altona 14 Amaranth 2 Anola 2 Arborg 4 Ashern 15 Austin 2 Bacon Ridge 2 Balsam Harbour 1 Beausejour 14 Benito 1 Beulah 1 Birds Hill 2 Black River First Nation 2 Bloodvein First Nation 6 Blumenort 1 Boissevain 3 Bowsman 1 Brandon 16 Brereton Lake 3 Brokenhead Ojibway Nation 1 Brunkild 2 Caddy Lake 1 Carberry 1 Carman 4 Cartwright 1 Clandeboye 1 Cracknell 1 Crane River 1 Crystal City 6 Dacotah 3 Dakota Plains First Nation 1 Dauphin 23 Dog Creek 4 Douglas 1 Dufresne 2 East Selkirk 1 Ebb and Flow First Nation 2 Edrans 1 Elphinstone 1 Eriksdale 9 Fairford 2 Falcon Lake 1 Fannystelle 1 Fisher Branch 1 Fisher River Cree Nation 4 Fort Alexander 3 Fortier 1 Foxwarren 1 Fraserwood 2 Garson 1 Gilbert Plains 1 Gimli 15 Giroux 1 Gladstone 1 Glenboro 2 Grand Marais 2 Grandview 1 Grosse Isle 1 Grunthal 5 Gypsumville 3 Hadashville 3 Hartney 1 Hazelridge 1 Headingley 5 Hilbre 1 Hodgson 21 Hollow Water First Nation 3 Ile des Chênes 3 Jackhead 1 Keeseekoowenin Ojibway First Nation 1 Kelwood 1 Kenton 1 Killarney 8 Kirkness 1 Kleefeld 1 La Rivière 1 La Salle 1 Lac du Bonnet 3 Landmark 3 Langruth 1 Lenore 1 Libau 1 Little Grand Rapids 3 Little Saskatchewan First Nation 7 Lockport 2 Long Plain First Nation 5 Lorette 3 Lowe Farm 1 Lundar 3 MacGregor 1 Manigotagan 2 Manitou 3 Marchand 2 Mariapolis 1 McCreary 1 Middlebro 5 Milner Ridge 2 Minnedosa 4 Minto 1 Mitchell -

Manitoba Regional Health Authority (RHA) DISTRICTS MCHP Area Definitions for the Period 2002 to 2012
Manitoba Regional Health Authority (RHA) DISTRICTS MCHP Area Definitions for the period 2002 to 2012 The following list identifies the RHAs and RHA Districts in Manitoba between the period 2002 and 2012. The 11 RHAs are listed using major headings with numbers and include the MCHP - Manitoba Health codes that identify them. RHA Districts are listed under the RHA heading and include the Municipal codes that identify them. Changes / modifications to these definitions and the use of postal codes in definitions are noted where relevant. 1. CENTRAL (A - 40) Note: In the fall of 2002, Central changed their districts, going from 8 to 9 districts. The changes are noted below, beside the appropriate district area. Seven Regions (A1S) (* 2002 changed code from A8 to A1S *) '063' - Lakeview RM '166' - Westbourne RM '167' - Gladstone Town '206' - Alonsa RM 'A18' - Sandy Bay FN Cartier/SFX (A1C) (* 2002 changed name from MacDonald/Cartier, and code from A4 to A1C *) '021' - Cartier RM '321' - Headingley RM '127' - St. Francois Xavier RM Portage (A1P) (* 2002 changed code from A7 to A1P *) '090' - Macgregor Village '089' - North Norfolk RM (* 2002 added area from Seven Regions district *) '098' - Portage La Prairie RM '099' - Portage La Prairie City 'A33' - Dakota Tipi FN 'A05' - Dakota Plains FN 'A04' - Long Plain FN Carman (A2C) (* 2002 changed code from A2 to A2C *) '034' - Carman Town '033' - Dufferin RM '053' - Grey RM '112' - Roland RM '195' - St. Claude Village '158' - Thompson RM 1 Manitoba Regional Health Authority (RHA) DISTRICTS MCHP Area -
The Arctic Gateway Group Is Owned by First Nations and Bayline Communities, Fairfax and Agt Foods, Building a Natural Resources
THE ARCTIC GATEWAY GROUP IS OWNED BY FIRST NATIONS AND BAYLINE COMMUNITIES, FAIRFAX AND AGT FOODS, BUILDING A NATURAL RESOURCES GATEWAY THROUGH THE ARCTIC TO THE WORLD. Arctic Gateway Group LP Arctic_Gateway ArcticGateway 728 Bignell Ave. ArcticGateway The Pas, MB R9A 1L8 1-888-445-1112 [email protected] www.arcticgateway.com ABOUT THE GATEWAY The Arctic Gateway Group LP owns and operates the Port of Churchill, Canada’s only Arctic seaport serviced by rail, on the Hudson Bay Railway, running from The Pas to Churchill, Manitoba. Strategically located on the west coast of Hudson Bay, the Arctic Gateway is the front door to Western Canada, linking Canadian trade in resources to the global marketplace. The Arctic Gateway’s logistical advantage, rail assets and unique location provide direct and efficient routes to markets for Canada’s abundant natural resources and manufactured products, while connecting Canadian consumers and importers to the world marketplace via the North. Hudson Bay Railway (CN, KRC) port of The Hudson Bay Railway is made up of 627 miles port location interchange churchill hudson bay railroad (hbr) agg HBR operating of former Canadian National (CN) trackage, with a agg railroad agreement network that connects with CN in The Pas, running north through Manitoba to the Hudson Bay at the lynn lake kelsey gillam Port of Churchill. The Hudson Bay Railway is a vital transportation pukatawagan thompson link in northern Manitoba, hauling perishables, automobiles, frac ilford sherridon thicket Flin Flon sand, construction material, heavy and dimensional equipment, sherritt jct wabowden scrap, hazardous materials, kraft paper, concentrates, containers, Cranberry portage the pas the pas jct fertilizer, wheat and other grain products. -
CTI / RHA Community/Region Index Jan-19
CTI / RHA Community/Region Index Jan-19 Location CTI Region Health Authority A Aghaming North Eastman Interlake-Eastern Health Akudik Churchill WRHA Albert North Eastman Interlake-Eastern Health Albert Beach North Eastman Interlake-Eastern Health Alexander Brandon Prairie Mountain Health Alfretta (see Hamiota) Assiniboine North Prairie Mountain Health Algar Assiniboine South Prairie Mountain Health Alpha Central Southern Health Allegra North Eastman Interlake-Eastern Health Almdal's Cove Interlake Interlake-Eastern Health Alonsa Central Southern Health Alpine Parkland Prairie Mountain Health Altamont Central Southern Health Albergthal Central Southern Health Altona Central Southern Health Amanda North Eastman Interlake-Eastern Health Amaranth Central Southern Health Ambroise Station Central Southern Health Ameer Assiniboine North Prairie Mountain Health Amery Burntwood Northern Health Anama Bay Interlake Interlake-Eastern Health Angusville Assiniboine North Prairie Mountain Health Anola North Eastman Interlake-Eastern Health Arbakka South Eastman Southern Health Arbor Island (see Morton) Assiniboine South Prairie Mountain Health Arborg Interlake Interlake-Eastern Health Arden Assiniboine North Prairie Mountain Health Argue Assiniboine South Prairie Mountain Health Argyle Interlake Interlake-Eastern Health Arizona Central Southern Health Amaud South Eastman Southern Health Ames Interlake Interlake-Eastern Health Amot Burntwood Northern Health Anola North Eastman Interlake-Eastern Health Arona Central Southern Health Arrow River Assiniboine -
Keeyask Generation Project April 2014
REPORT ON PUBLIC HEARING Keeyask Generation Project April 2014 REPORT ON PUBLIC HEARING Keeyask Generation Project April 2014 ii iii iv Table of Contents Foreword . xi Executive Summary . xv Chapter One: Introduction. .1 1.1 Th e Manitoba Clean Environment Commission. .1 1.2 Th e Project . .1 1.3 Th e Proponent. .2 1.4 Terms of Reference . .3 1.5 Th e Hearings . .4 1.6 Th e Report. .4 Chapter Two: The Licensing Process . .7 2.1 Needed Licences and Approvals . .7 2.2 Review Process for an Environment Act Licence . .7 2.3 Federal Regulatory Review and Decision Making . .8 2.4 Section 35 of Canada’s Constitution. .8 2.5 Need For and Alternatives To. .9 2.6 Role of the Clean Environment Commission . .9 2.7 Th e Licensing Decision. .9 Chapter Three: The Public Hearing Process. 11 3.1 Clean Environment Commission . 11 3.2 Public Participation . 11 3.2.1 Participants . 11 3.2.2 Participant Assistance Program . 11 3.2.3 Presenters. 12 3.3 Th e Pre-Hearing . 12 3.4 Th e Hearings . 12 v Chapter Four: Manitoba’s Electrical Generation and Transmission System . 13 4.1 System Overview. 13 4.2 Generating Stations . 15 4.3 Lake Winnipeg Regulation and the Churchill River Diversion. 17 Chapter Five: The Keeyask Generation Project. 21 5.1 Overview. 21 5.2 Major Project Components and Infrastructure. 23 5.2.1 Powerhouse . 23 5.2.2 Spillway . 24 5.2.3 Dams . 24 5.2.4 Dykes . 24 5.2.5 Ice Boom . -
Market Housing Program
Achieving the Right Balance CANDO’s 24th Annual Conference – October 23, 2017 Fredericton, New Brunswick 1 The Fund’s Vision Every First Nation family has the opportunity to have a home on their own land in a strong community. 2 ©2008 FNMHF 3 ©2008 FNMHF # of First Nation Applications Received by the Fund / Total # of FNs in each Prov./ Territories (as of September 30, 2017) 9/14 2/33 84/202 18/47 16/63 13/75 13/40 65/134 12/35 ©2008 FNMHF First Nations announced for Credit Enhancement as of October 5, 2017 • Miawpukek, NF •Siksika, AB •Neskonlith, BC •Penelakut, BC • Membertou, NS • T’it’q’et, BC • Nipissing, ON • Nooaitch, BC • Lac La Ronge, SK • Eastmain, QC • Mississauga, ON • Skeetchestn, BC • Batchewana, ON • Tsawout, BC • Wemindji, QC • Kwanlin Dün, YT • Onion Lake, SK • Sagamok, ON • Henvey Inlet, ON • Sechelt, BC • Atikameksheng, ON • Seabird Island, BC • Beausoleil, ON •Teslin Tlingit Council, YT Anishnawbek, ON • Tk’emlups, BC • Wahnapitae, ON • Tsartlip First Nation, BC • Whitefish River, ON • Moose Cree, ON • Temagami, ON • Tr'ondëk Hwëch'in, YT • Champagne & • Serpent River, ON • Carcross/Tagish, YT Aishihik, YT • Curve Lake, ON • Penticton, BC • Skidegate, BC • Pic River, ON • Mohawks of the Bay • Aundeck Omni • Quatsino, BC • Lac Seul, ON of Quinte, ON Kaning, ON • Little Shuswap ,BC • Waswanipi, QC • Adams Lake, BC • Long Plain, MB • Mistissini, QC • Flying Dust, SK • Garden River, ON • Skwah, BC •Saugeen, ON • Okanagan, BC • Lower Nicola, BC • Fisher River, MB •Wahta, ON • Chisasibi, QC • Upper Nicola, BC •Alderville, ON •Mattagami, ON • Chippewas of • Hiawatha, ON • Lake Cowichan, BC •Chapleau Cree, ON Nawash, ON • M’Chigeeng, ON •Leq’á:mél, BC •Nuxalk, BC • Simpcw, BC • ʔaq'am (St. -

Page 1 of 3 MANITOBA FIRST NATIONS POLICE SERVICE
MANITOBA FIRST NATIONS POLICE SERVICE (DAKOTA OJIBWAY POLICE SERVICE) History The original establishment of the Dakota Ojibway Tribal Council Police Department, now known as the Dakota Ojibway Police Service, dated December 1974, was prepared and agreed to by all Chiefs of the D.O.T.C. After three years of negotiations, funding was approved by the different levels of government. In November of 1977, the police department commenced operations with one Chief of Police and nine members. The program was funded by Indian & Northern Affairs Canada from 1977 to 1993. The development of the Police Service was to establish local control and accountability to the First Nation communities. In November of 1993, the Police Service ceased operations due to a lack of funding commitment from the Province of Manitoba. Tripartite negotiations reconvened in 1994 and technical meetings took place as follows: March 10, May 12, May 26 and June 23, 1994. On May 19, 1994, the D.O.T.C. Council of Chiefs and representatives from both levels of Government, Manitoba Justice and Public Safety Canada were able to secure an Interim Policing Service Agreement which saw the restoration of joining policing services (D.O.P.S./R.C.M.P.) to (7) seven of the (8) eight D.O.T.C. Member First Nation communities, with the effective start date of June 1, 1994. On December 31, 1994, a long-term Tripartite Agreement was finalized and on February 1, 1995, the Dakota Ojibway Police Service resumed full-time policing services to (6) six D.O.T.C. First Nation communities: Birdtail Sioux First Nation, Dakota Plains Wahpeton Nation, Long Plain First Nation, Canupawakpa Dakota Nation, Roseau River Anishinabe First Nation and Sioux Valley Dakota Nation. -
Copy of Green and Teal Simple Grid Elementary School Book Report
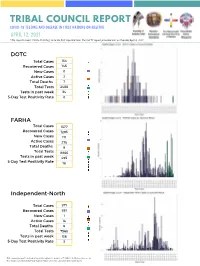
TRIBAL COUNCIL REPORT COVID-19 TESTING AND DISEASE IN FIRST NATIONS ON RESERVE APRIL 12, 2021 *The reports covers COVID-19 testing since the first reported case. The last TC report provided was on Tuesday April 6, 2021. DOTC Total Cases 154 Recovered Cases 145 New Cases 0 Active Cases 2 Total Deaths 7 Total Tests 2488 Tests in past week 34 5-Day Test Positivity Rate 0 FARHA Total Cases 1577 Recovered Cases 1293 New Cases 111 Active Cases 275 Total Deaths 9 Total Tests 8866 Tests in past week 495 5-Day Test Positivity Rate 18 Independent-North Total Cases 871 Recovered Cases 851 New Cases 1 Active Cases 14 Total Deaths 6 Total Tests 7568 Tests in past week 136 5-Day Test Positivity Rate 3 This summary report is intended to provide high-level analysis of COVID-19 testing and disease in First Nations on reserve by Tribal Council Region since first case until date noted above. APRIL 12, 2021 Independent- South Total Cases 218 Recovered Cases 214 New Cases 1 Active Cases 2 Total Deaths 2 Total Tests 1932 Tests in past week 30 5-Day Test Positivity Rate 6 IRTC Total Cases 380 Recovered Cases 370 New Cases 0 Active Cases 1 Total Deaths 9 Total Tests 3781 Tests in past week 55 5-Day Test Positivity Rate 0 KTC Total Cases 1011 Recovered Cases 948 New Cases 39 Active Cases 55 Total Deaths 8 Total Tests 7926 Tests in past week 391 5-Day Test Positivity Rate 10 This summary report is intended to provide high-level analysis of COVID-19 testing and disease in First Nations on reserve by Tribal Council Region since first case until date noted above. -

Meet Snow Lake's 2008 Grads
Sweet Nothings Please see us for giftware, souvenirs, jewelry, com- puter parts and service, Epicure, baby and bath items, flowers, pictures, and the work of a variety Providing business and residential High Speed Wireless Internet service to of local artists, artisans, musicians, and writers. Snow Lake and the surrounding area. Packages start as low as $27.95. Give us a call today and find out how we Open Tuesday to Friday from 12:00 to 5:00 p.m., Saturday from can hook you up with lightning fast High Speed Internet! 10:00 a.m. to 4:00 p.m. Call toll free at 1-866-206-3707, E-mail: [email protected], or Check us out online: www.yourgiftideastore.com see our web page: http://www.gillamnet.com $1.00 NDERGROUND THE U PRESS Volume 12, Issue 12 Snow Lake Manitoba June 12, 2008 Meet Snow Lake's 2008 grads... AROUND TOWN • On June 5th, Judy Bishop ad- vised that her son had 103 days until he arrived home from his tour of duty in Afghanistan. She says that she misses him terribly, but he manages to call and email a lot when he is any- where with access. She also said he was saddened to hear of the recent loss of a member of his battalion, The Princess Patricia's Canadian Light Infantry, based at CFB Shilo. Noting that although he didn’t know Capt. Richard (Steve) Class of 2008: (L) Jenna Wiwcharuk-Roy, Dana Kowalchuk, Jace Ryan, Sheila Holmgren, Christina Walker, Brittany Ventura, and Danny Otto (Reclining).