Assessment of the Sustainability of the Enugu State CDTI Project
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Enugu State, Nigeria Out-Of-School Children Survey Report
ENUGU STATE, NIGERIA OUT-OF-SCHOOLCHILDREN SURVEY REPORT October, 2014 PREFACE The challenge of school-aged children who for one reason or another did not enrol in school at all or enrolled and later dropped out for whatever reason has been a perennial challenge to education the world over. Nigeria alone is said to house over 10 million out of school children. This is in spite of the universal basic education programme which has been running in the country since 1999. For Enugu State, it is not clear what the state contributes to that national pool of children who are reported to be out of school. Given the effort of the State Government in implementing the universal basic education programme, it is easy to assume that all children in Enugu State are enrolled and are attending school. This kind of assumption might not give us the benefit of knowing the true state of things as they relate to out-of-school children in our State. This is even more so given the State’s development and approval of the Inclusive Education Policy, which has increased the challenge of ensuring that every child of school age, no matter his or her circumstance of birth or residence, has access to quality education; hence, the need to be concerned even for only one child that is out of school. It is, therefore, in a bid to ascertain the prevalence of the incidence of children who are outside the school system, whether public or private, that the Ministry of Education and Enugu State Universal Basic Education Board collaborated with DFID-ESSPIN and other stakeholders to conduct the out of school children’s survey. -
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021
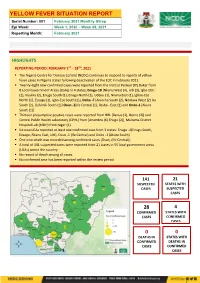
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021 HIGHLIGHTS REPORTING PERIOD: FEBRUARY 1ST – 28TH, 2021 ▪ The Nigeria Centre for Disease Control (NCDC) continues to respond to reports of yellow fever cases in Nigeria states following deactivation of the EOC in February 2021. ▪ Twenty -eight new confirmed cases were reported from the Institut Pasteur (IP) Dakar from 8 Local Government Areas (LGAs) in 4 states; Enugu-18 [Nkanu West (4), Udi (3), Igbo-Etiti (2), Nsukka (2), Enugu South (1), Enugu North (1), Udenu (1), Nkanu East (1), Igboe-Eze North (1), Ezeagu (1), Igbo-Eze South (1)], Delta -7 [Aniocha South (2), Ndokwa West (2) Ika South (2), Oshimili South (1)] Osun -2[Ife Central (1), Ilesha - East (1) and Ondo-1 [Akure South (1)] ▪ Thirteen presumptive positive cases were reported from NRL [Benue (2), Borno (2)] and Central Public Health Laboratory (CPHL) from [Anambra (6) Enugu (2)], Maitama District Hospital Lab (MDH) from Niger (1) ▪ Six new LGAs reported at least one confirmed case from 3 states: Enugu -4(Enugu South, Ezeagu, Nkanu East, Udi), Osun -1 (Ife Central) and Ondo -1 (Akure South) ▪ One new death was recorded among confirmed cases [Osun, (Ife Central)] ▪ A total of 141 suspected cases were reported from 21 states in 55 local government areas (LGAs) across the country ▪ No record of death among all cases. ▪ No confirmed case has been reported within the review period 141 21 SUSPECTED STATES WITH CASES SUSPECTED CASES 28 4 -

PROVISIONAL LIST.Pdf
S/N NAME YEAR OF CALL BRANCH PHONE NO EMAIL 1 JONATHAN FELIX ABA 2 SYLVESTER C. IFEAKOR ABA 3 NSIKAK UTANG IJIOMA ABA 4 ORAKWE OBIANUJU IFEYINWA ABA 5 OGUNJI CHIDOZIE KINGSLEY ABA 6 UCHENNA V. OBODOCHUKWU ABA 7 KEVIN CHUKWUDI NWUFO, SAN ABA 8 NWOGU IFIONU TAGBO ABA 9 ANIAWONWA NJIDEKA LINDA ABA 10 UKOH NDUDIM ISAAC ABA 11 EKENE RICHIE IREMEKA ABA 12 HIPPOLITUS U. UDENSI ABA 13 ABIGAIL C. AGBAI ABA 14 UKPAI OKORIE UKAIRO ABA 15 ONYINYECHI GIFT OGBODO ABA 16 EZINMA UKPAI UKAIRO ABA 17 GRACE UZOME UKEJE ABA 18 AJUGA JOHN ONWUKWE ABA 19 ONUCHUKWU CHARLES NSOBUNDU ABA 20 IREM ENYINNAYA OKERE ABA 21 ONYEKACHI OKWUOSA MUKOSOLU ABA 22 CHINYERE C. UMEOJIAKA ABA 23 OBIORA AKINWUMI OBIANWU, SAN ABA 24 NWAUGO VICTOR CHIMA ABA 25 NWABUIKWU K. MGBEMENA ABA 26 KANU FRANCIS ONYEBUCHI ABA 27 MARK ISRAEL CHIJIOKE ABA 28 EMEKA E. AGWULONU ABA 29 TREASURE E. N. UDO ABA 30 JULIET N. UDECHUKWU ABA 31 AWA CHUKWU IKECHUKWU ABA 32 CHIMUANYA V. OKWANDU ABA 33 CHIBUEZE OWUALAH ABA 34 AMANZE LINUS ALOMA ABA 35 CHINONSO ONONUJU ABA 36 MABEL OGONNAYA EZE ABA 37 BOB CHIEDOZIE OGU ABA 38 DANDY CHIMAOBI NWOKONNA ABA 39 JOHN IFEANYICHUKWU KALU ABA 40 UGOCHUKWU UKIWE ABA 41 FELIX EGBULE AGBARIRI, SAN ABA 42 OMENIHU CHINWEUBA ABA 43 IGNATIUS O. NWOKO ABA 44 ICHIE MATTHEW EKEOMA ABA 45 ICHIE CORDELIA CHINWENDU ABA 46 NNAMDI G. NWABEKE ABA 47 NNAOCHIE ADAOBI ANANSO ABA 48 OGOJIAKU RUFUS UMUNNA ABA 49 EPHRAIM CHINEDU DURU ABA 50 UGONWANYI S. AHAIWE ABA 51 EMMANUEL E. -

Niger Delta Budget Monitoring Group Mapping
CAPACITY BUILDING TRAINING ON COMMUNITY NEEDS ASSESSMENT & SHADOW BUDGETING NIGER DELTA BUDGET MONITORING GROUP MAPPING OF 2016 CAPITAL PROJECTS IN THE 2016 FGN BUDGET FOR ENUGU STATE (Kebetkache Training Group Work on Needs Assessment Working Document) DOCUMENT PREPARED BY NDEBUMOG HEADQUARTERS www.nigerdeltabudget.org ENUGU STATE FEDERAL MINISTRY OF EDUCATION UNIVERSAL BASIC EDUCATION (UBE) COMMISSION S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Teaching and Learning 40,000,000 Enugu West South East New Materials in Selected Schools in Enugu West Senatorial District 2 Construction of a Block of 3 15,000,000 Udi Ezeagu/ Udi Enugu West South East New Classroom with VIP Office, Toilets and Furnishing at Community High School, Obioma, Udi LGA, Enugu State Total 55,000,000 FGGC ENUGU S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Construction of Road Network 34,264,125 Enugu- North Enugu North/ Enugu East South East New Enugu South 2 Construction of Storey 145,795,243 Enugu-North Enugu North/ Enugu East South East New Building of 18 Classroom, Enugu South Examination Hall, 2 No. Semi Detached Twin Buildings 3 Purchase of 1 Coastal Bus 13,000,000 Enugu-North Enugu North/ Enugu East South East Enugu South 4 Completion of an 8-Room 66,428,132 Enugu-North Enugu North/ Enugu East South East New Storey Building Girls Hostel Enugu South and Construction of a Storey Building of Prep Room and Furnishing 5 Construction of Perimeter 15,002,484 Enugu-North Enugu North/ Enugu East South East New Fencing Enugu South 6 Purchase of one Mercedes 18,656,000 Enugu-North Enugu North/ Enugu East South East New Water Tanker of 11,000 Litres Enugu South Capacity Total 293,145,984 FGGC LEJJA S/N PROJECT AMOUNT LGA FED. -

Enugu State Nigeria Erosion and Watershed
RESETTLEMENT ACTION PLAN (RAP) Public Disclosure Authorized ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) Public Disclosure Authorized FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE Public Disclosure Authorized FINAL REPORT Public Disclosure Authorized RESETTLEMENT ACTION PLAN (RAP) ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE FINAL REPORT Submitted to: State Project Management Unit Nigeria Erosion and Watershed Management Project (NEWMAP) Enugu State NIGERIA NOVEMBER 2014 Page | ii Resettlement Action Plan for 9th Mile Gully Erosion Site Enugu State- Final Report TABLE OF CONTENTS TABLE OF CONTENTS.................................................................................................................................................................... ii LIST OF FIGURES .................................................................................................................................................................... v LIST OF TABLES...................................................................................................................................................................... v LIST OF PLATES ...................................................................................................................................................................... v DEFINITIONS ....................................................................................................................................................................... -

Geoelectrical Sounding for the Determination of Groundwater Prospects in Awgu and Its Environs, Enugu State, Southeastern Nigeria
IOSR Journal of Applied Geology and Geophysics (IOSR-JAGG) e-ISSN: 2321–0990, p-ISSN: 2321–0982.Volume 5, Issue 1 Ver. I (Jan. - Feb. 2017), PP 14-22 www.iosrjournals.org Geoelectrical Sounding for The Determination Of Groundwater Prospects In Awgu And Its Environs, Enugu State, Southeastern Nigeria OKEKE J. P.1; EZEH C. C2. ; OKONKWO A. C3. 1,2,3(Department of Geology and Mining, Enugu state University of science and Technology, Enugu State, Nigeria. West Africa). [email protected] Abstract: Geoelectrical sounding to determine the groundwater prospect in Awgu and its environs has been carried out. The study area lies within longitudes 007025’E and 0070 35’E and latitudes 06002’N and 06017’N with an area extent of 513sqkm. The area is underlain by two lithostratigraphic units, Awgu Shale and Owelli Sandstone. A total of ninety five (95) Vertical Electrical Soundings (VES) was acquired employing the Schlumberger electrode array configuration, with a maximum electrode separation ranging from 700m to 800m. Data analysis was done using a computer program RESOUND to generate the layer apparent resistivity, thickness and depth. A maximum of eight (8) layer resistivity were generated in each sounding point with a depth range of 50m to 356m. From the interpreted VES data layer 6, 7, and 8 are possible target for prospective aquifer horizons. Interpreted geoelectric layers show a sequence of shale/sand – shale sand – sand. Various contour maps were constructed using surfer 10 contouring program- Iso resistivity, Isochore (depth), Isopach (thickness), Longitudinal conductance and transverse resistance to show variation of parameters in the study area. -

Public Disclosure Authorized
INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT INTERNATIONAL DEVELOPMENT ASSOCIATION THE INSPECTION PANEL 1818 H Street, N.W. Telephone: (202) 458-5200 Washington, D.C. 20433 Fax: (202) 522-0916 Email: [email protected] Eimi Watanabe Chairperson Public Disclosure Authorized JPN REQUEST RQ13/09 July 16, 2014 MEMORANDUM TO THE EXECUTIVE DIRECTORS OF THE INTERNATIONAL DEVELOPMENT ASSOCIATION Request for Inspection Public Disclosure Authorized NIGERIA: Lagos Metropolitan Development and Governance Project (P071340) Notice of Non Registration and Panel's Observations of the First Pilot to Support Early Solutions Please find attached a copy of the Memorandum from the Chairperson of the Inspection Panel entitled "Request for Inspection - Nigeria: Lagos Metropolitan Development and Governance Project (P071340) - Notice of Non Registration and Panel's Observations of the First Pilot to Support Early Solutions", dated July 16, 2014 and its attachments. This Memorandum was also distributed to the President of the International Development Association. Public Disclosure Authorized Attachment cc.: The President Public Disclosure Authorized International Development Association INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT INTERNATIONAL DEVELOPMENT ASSOCIATION THE INSPECTION PANEL 1818 H Street, N.W. Telephone: (202) 458-5200 Washington, D.C. 20433 Fax : (202) 522-0916 Email: [email protected] Eimi Watanabe Chairperson IPN REQUEST RQ13/09 July 16, 2014 MEMORANDUM TO THE PRESIDENT OF THE INTERNATIONAL DEVELOPMENT ASSOCIATION Request for Inspection NIGERIA: Lagos Metropolitan Development and Governance Project (P071340) Notice of Non Registration and Panel's Observations of the First Pilot to Support Early Solutions Please find attached a copy of the Memorandum from the Chairperson of the Inspection Panel entitled "Request for Inspection - Nigeria: Lagos Metropolitan Development and Governance Project (P07 J340) - Notice of Non Registration and Panel's Observations of the First Pilot to Support Early Solutions" dated July 16, 2014 and its attachments. -

Lessons from Nigeria's 2011 Elections
Policy Briefing Africa Briefing N°81 Abuja/Dakar/Brussels, 15 September 2011 Lessons from Nigeria’s 2011 Elections democracy and overall political health. The eve of the elec- I. OVERVIEW tions was marked by a blend of cautious optimism and foreboding. Attahiru Jega, INEC chair, and his team won With the April 2011 general elections, Nigeria may have plaudits for instituting important reforms, including to the taken steps towards reversing the degeneration of its pre- voting procedure; the introduction of the idea of commu- vious elections, but the work is not finished. Despite some nity mandate protection to prevent malpractice; and the progress, early and intensive preparations for the 2015 prosecution and sentencing of officials, including the elections need to start now. Voter registration need not be electoral body’s own staff, for electoral offences. There as chaotic and expensive as it was this year if done on a were also grounds for pessimism: the upsurge of violence continual basis. Far-reaching technical and administrative in several states, encouraged by politicians and their sup- reforms of, and by, the Independent National Electoral porters who feared defeat; an ambiguous and confusing Commission (INEC), notably internal restructuring and legal framework for the elections; and a flawed voter reg- constituency delineation, should be undertaken and ac- istration exercise, with poorly functioning biometric scans, companied by broad political and economic reforms that that resulted in an inflated voters roll. make the state more relevant to citizens and help guaran- tee an electoral and democratic future. The deadly post- Few, however, predicted the violence that erupted in some presidential election violence in the North and bomb blasts Northern states following the announcement of the presi- by the Islamic fundamentalist Boko Haram sect since dential results. -
Shelf Prospectus Within the Meaning of Rule 40 (C) of the Sec Rules and Regulations
THIS DOCUMENT IS IMPORTANT AND SHOULD BE READ CAREFULLY. IF YOU ARE IN ANY DOUBT ABOUT ITS CONTENTS OR THE ACTION TO BE TAKEN, PLEASE CONSULT YOUR BANKER, STOCKBROKER, ACCOUNTANT, SOLICITOR OR ANY OTHER PROFESSIONAL ADVISER FOR GUIDANCE IMMEDIATELY. FOR INFORMATION CONCERNING CERTAIN RISK FACTORS WHICH SHOULD BE CONSIDERED BY PROSPECTIVE INVESTORS, SEE “RISK FACTORS” COMMENCING ON PAGE 45 HEREOF. THIS DEBT ISSUANCE PROGRAMME PROSPECTUS CONSTITUTES A SHELF PROSPECTUS WITHIN THE MEANING OF RULE 40 (C) OF THE SEC RULES AND REGULATIONS GOMBE STATE GOVERNMENT OF NIGERIA BOND ISSUANCE PROGRAMME OF N30,000,000,000 This Shelf Prospectus is to be read and construed in conjunction with any supplement hereto and all documents which are incorporated herein by reference and, in relation to any Series or Tranches (as defined herein) of Bonds, together with the applicable Pricing Supplement. This Shelf Prospectus shall be read and construed on the basis that such documents are incorporated and form part of this Shelf Prospectus. This Shelf Prospectus has been seen and approved by the representatives of the State Executive Council (the “Executive Council”). The Gombe State Executive Council (“EXCO”) on behalf of the Gombe State Government have taken reasonable care to ensure that the material facts contained herein are true and accurate in all material respects and confirm having made all reasonable enquiries, that to the best of their knowledge and belief, there are no material facts, the omission of which would make any statement herein misleading or untrue. The contents of this Shelf Prospectus are not to be construed as legal, financial or tax advice. -

Nigeria's Elections
Policy Briefing Africa Briefing N°79 Abuja/Dakar/Brussels, 24 February 2011 Nigeria’s Elections: Reversing the Degeneration? needed reforms against the imperative of actually holding I. OVERVIEW elections in 2011. He inherited an organisation complicit in the 2007 fraud, exposed to manipulation outside the The April 2011 general elections – if credible and peace- capital and over which the new Electoral Act denies him ful – would reverse the degeneration of the franchise full control. To his – and the nation’s – credit, a gamble to since Nigeria returned to civilian rule in 1999, yield more conduct a risky voter registration exercise seems to have representative and legitimate institutions and restore faith paid off, but its shaky start was a reminder of challenges, in a democratic trajectory. Anything similar to the 2007 even in simply delivering materials around the vast coun- sham, however, could deepen the vulnerability of West try in a timely manner. Africa’s largest country to conflict, further alienate citi- zens from the political elite and reinforce violent groups’ Underlying causes of electoral flaws, however, run deeper narratives of bad governance and exclusion. Flawed polls, than election administration. Stakes are high: the state is especially if politicians stoke ethnic or religious divides, the principle means of generating wealth; vast oil reve- may ignite already straining fault lines, as losers protest nues are accessed through public office. Extreme poverty results. Despite encouraging electoral preparations, serious makes voters vulnerable to bribes and intimidation. The obstacles remain. Many politicians still seem determined election takes place against an upsurge in violence, in- to use violence, bribery or rigging to win the spoils of of- cluding attacks in Borno, communal violence in Jos and fice. -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -

Hemispheres Studies on Cultures and Societies Vol. 30, No. 3
Institute of Mediterranean and Oriental Cultures Polish Academy of Sciences Hemispheres Studies on Cultures and Societies Vol. 30, No. 3 NIGERIA Wydawnictwo Naukowe ASKON Warszawa 2015 Editor-in-Chief Board of Advisory Editors JERZY ZDANOWSKI GRZEGORZ J. KACZYÑSKI OLA EL KHAWAGA Subject Editor MARIUSZ KRANIEWSKI ABIDA EIJAZ HARRY T. NORRIS English Text Consultant STANIS£AW PI£ASZEWICZ STEPHEN WALLIS EVARISTE N. PODA Secretary MARIA SK£ADANKOWA SABINA BRAKONIECKA MICHA£ TYMOWSKI This edition is prepared, set and published by Wydawnictwo Naukowe ASKON Sp. z o.o. ul. Stawki 3/1, 00193 Warszawa tel./fax: (48) 22 635 99 37 www.askon.waw.pl [email protected] © Copyright by Institute of Mediterranean and Oriental Cultures, Polish Academy of Sciences, Warsaw 2015 PL ISSN 02398818 ISBN 9788374520874 HEMISPHERES is published quarterly and is indexed in ERIH PLUS, The Central European Journal of Social Sciences and Humanities, ProQuest Database and Index Copernicus Contents Nkem O k o h, Translation as Validation of Culture: The Example of Chinua Achebe ....................................................................................... 5 Khalid I m a m, Justice, Fairness and the Quest for an Egalitarian Society in Africa: A Reading of Bukar Usmans Select Tales in Taskar Tatsuniyoyi: Littafi na Daya Zuwa na Goma Sha Hudu [A Compendium of Hausa Tales Book One to Fourteen] ....................................................21 Ibrahim Garba Satatima, Hausa Oral Songs as a Cultural Reflexive: A Study on Some Emotional Compositions ................................................33