Human Services Committee.Ecl
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2011 Political Contributions
2011 POLITICAL CONTRIBUTIONS 2011 Lilly Political Contributions 2 Government actions such as price controls, pharmaceutical manufacturer rebates, the Prescription Drug User Fee Act (PDUFA), and access to Lilly medicines affect our ability to invest in innovation. Lilly has a comprehensive government relations operation to have a voice in the public policymaking process at both the state and federal levels. Lilly is committed to participating in the political process as a responsible corporate citizen to help inform the U.S. debate over health care and pharmaceutical innovation. As a company that operates in a highly competitive and regulated industry, Lilly must participate in the political process to fulfill its fiduciary responsibility to its shareholders, and its overall responsibilities to its customers and its employees. Corporate Political Contribution Elected officials, no matter what level, have an impact on public policy issues affecting Lilly. We are committed to backing candidates who support public policies that contribute to pharmaceutical innovation and healthy patients. A number of factors are considered when reviewing candidates for support. The following evaluation criteria are used to allocate political contributions: • Has the candidate historically voted or announced positions on issues of importance to Lilly, such as pharmaceutical innovation and health care? • Has the candidate demonstrated leadership on key committees of importance to our business? • Does the candidate demonstrate potential for legislative leadership? -

Commonwealth of Pennsylvania Legislative
COMMONWEALTH OF PENNSYLVANIA LEGISLATIVE JOURNAL TUESDAY, NOVEMBER 15, 2016 SESSION OF 2016 200TH OF THE GENERAL ASSEMBLY No. 70 HOUSE OF REPRESENTATIVES JOURNALS APPROVED The House convened at 11 a.m., e.s.t. The SPEAKER. Without objection, all Journals not now in print will be approved. THE SPEAKER (MIKE TURZAI) PRESIDING REMARKS BY SPEAKER PRAYER The SPEAKER. Members, at this time I want to show great respect to one of our retiring members, Representative Ted HON. BRYAN BARBIN, member of the House of Harhai. Representatives, offered the following prayer: Representative Harhai, sir, what was the first year that you served? Special election 1998 and served up to and through here Will you join me in bowing your heads to the creator of the 2016. universe. Representative Harhai, as you know, is a good friend to Dear Lord, as we come to the end of this 200th session of many of us in this chamber, and it is my honor to wish him Your Holy Experiment, bless all of the assembled that are Godspeed. ending their service this day. Remember them for their part in Ted served the 58th District of Westmoreland County for stewarding freedom for the benefit of others. 18 years. He is the Democratic chair of the Game and Fisheries Help us, Lord, to remember Your servant, Moses, and Your Committee, and by profession this good man, smart man, was command in Deuteronomy 31:12, to read the law at the end of an investment banker who previously worked in the financial every 7 years. "Assemble the people…so they can listen and markets in New York City and in Chicago. -

Newportville, Pennsylvania. N**Notlce*** This Meeting Notification Is Available on the Boilermakers Local Lodge No
-fnle¿vtzl¿bnø1,Øt'ailzr/aa/y' BOILERMAKERS . IRON SHIP BUILDERS BLACKSMITHS . FORGERS & HELPERS SUBORDINATE LODGE NO. 13 23OO NEW FALLS BOAD WWW.BOILERMAKERSl 3.ORG NEWPORTVILLE, PA 19056 oFFlcE (215) 785-5536 @".@orr FAX (21 5) 785-5867 September 22,2010 Dear Brothers & Sisters: *****PLEASE READ***** *****I M PORTANT N OTI G ES***** Please be advised that as per membership action and consent, the October Regular Monthly Meeting Date of Local Lodge No. 13 has been changed to Wednesday October 6, 2010 at 8:00 pm at the Frank Donlon Hall, 2300 New Falls Road, Newportville, Pennsylvania. n**NoTlcE*** This meeting notification is available on the Boilermakers Local Lodge No. 1 3 website www.boilermakersl 3.orq We will also be glad to e-mail the meeting notice to you if you provide us with an e-mail address. *****P¡n Ceremony***** - Service pins for 15 or more years of continuous membership will be given at our semi-annual pin ceremony during this meeting on October 6,2010. lf you would like to be part of this ceremony, kindly contact the union hall. ****"Political Alert***** - The upcoming General Election is very important to our future as boilermakers. lt is our duty as members of a boilermaker union to vote in all elections and to support labor friendly candidates. Local Lodge No. 13 will be very active with this election and are in need of volunteers. Activities will include phone banking, labor walks, putting out political signs and Get Out The Vote Campaign. Enclosed you will find a list of the General Election "Labor Friendly" Recommended Gandidates. -

Perzel for Speaker of the House
COMMONWEALTH OF PENNSYLVANIA LEGISLATIVE JOURNAL TUESDAY , JANUARY 2 , 2007 SESSION OF 2007 191ST OF THE GENERAL ASSEMBLY No. 1 HOUSE OF REPRESENTATIVES thank You, Father, for this great privilege of being able to call The House convened at 12 m., e.s.t. to You. We now await Your leading. Respond to us, Lord, in ac cordance with our faith. All this we pray after Your will. Amen. THE CHIEF CLERK (ROGER NICK) PRESIDING PLEDGE OF ALLEGIANCE CALL TO ORDER (The Pledge of Allegiance was recited by members and visitors.) The CHIEF CLERK. This being the day and the hour appointed by Article II, section 4, of the Constitution of The CHIEF CLERK. The Sergeants at Arms will open the Pennsylvania for the meeting of the General Assembly, the doors of the House. Members and guests may be sea ted. House of Representatives will now come to order. The Sergeants at Arms will close the doors of this House. The prayer will be offered by Rev. Donald Wilson, ELECTION RETURNS PRESENTED First Baptist Church, Waynesburg, PA. Immediately after the prayer, we will recite the Pledge of Allegiance. The CHIEF CLERK. The Chair recognizes the Sergeant at Members and all guests will please rise to the extent they are Arms of the House. able. The SERGEANT AT ARMS. Mr. Chief Clerk, Deputy Secretary of the Commonwealth, Andrew Sislo. The CHIEF CLERK. The Chair recognizes Mr. Sislo. PRAYER Mr. SI SLO. Mr. Chief Clerk, as Deputy Secretary of the Commonwealth, it is my honor to present on behalf of the REV. DR. -

Verizon Political Contributions January – December 2008 Verizon Political Contributions January – December 2008 1
VERIZON POLITICAL CONTRIBUTIONS JANUARY – DECEMBER 2008 Verizon Political Contributions January – December 2008 1 A Message from Tom Tauke Verizon is affected by a wide variety of government policies — from telecommunications regulation to taxation to health care and more — that have an enormous impact on the business climate in which we operate. We owe it to our shareowners, employees and customers to advocate public policies that will enable us to compete fairly and freely in the marketplace. Political contributions are one way we support the democratic electoral process and participate in the policy dialogue. Our employees have established political action committees at the federal level and in 25 states. These political action committees (PACs) allow employees to pool their resources to support candidates for office who generally support the public policies our employees advocate. This report lists all PAC contributions and corporate political contributions made by Verizon in 2008. The contribution process is overseen by the Corporate Governance and Policy Committee of our Board of Directors, which receives a comprehensive report and briefing on these activities at least annually. We intend to update this voluntary disclosure twice a year and publish it on our corporate website. We believe this transparency with respect to our political spending is in keeping with our commitment to good corporate governance and a further sign of our responsiveness to the interests of our shareowners. Thomas J. Tauke Executive Vice President Public -

Constitutional Convention and As Was Determined in the Affirmative and the Resolution Was the First President of the United States
COMMONWEALTH OF PENNSYLVANIA LEGISLATIVE JOURNAL TUESDAY , JANUARY 30 , 2007 SESSION OF 2007 191ST OF THE GENERAL ASSEMBLY No. 8 HOUSE OF REPRESENTATIVES Mr. McCALL. Yes, Mr. Speaker . The House convened at 11 a.m., e.s.t. I would request a leave for the day for the gentleman from Northampton, Mr. SAMUELSON, and for the week, the gentleman from Westm oreland, Mr. TANGRETTI. THE SPEAKER (DENNIS M. O 'BRIEN) The SPEAKER. Without objection, the gentlemen will be PRESIDING placed on leave. The Chair recognizes the minority leader. Without objection, PRAYER the gentleman places on leave for the day the gentlemen, Representative ARGALL from Schuylkill Cou nty and HON. MATTHEW E. BAKER, member of the House of Representative MOUL from Adams County. Without objection, Representatives, offered the following prayer: the gentlemen will be placed on leave. Thank you, Mr. Speaker . MASTER ROLL CALL Let us pray: Lord God , thank You for being in this place, as we come The SPEAKER. The Chair is about to take the master roll. before You humbly and acknowledge You as our holy and Members will proceed to vote. sovereign God. Empower the members and all staff during this new session to use this season of opportunity for Your glory. The following roll call was recorded: With new members and experience d members working together in the General Assembly, may good and wise decisions be PRES ENT –198 revealed, as both the will of the people and in accord with Your provident plan. Adolph Gabig Mantz Roebuck Show them the priorities that best honor You and inspire Baker Galloway Markosek Rohrer them to act promptly. -

2010 GENERAL ELECTION CANDIDATE GUIDEBOOK Table of Contents
2010 GENERAL ELECTION CANDIDATE GUIDEBOOK Table of Contents Gubernatorial Race Page 2 Pennsylvania Governor Edward G. Rendell is term-limited. Republican Tom Corbett and Democrat Dan Onorato are facing off in the General Election for a four-year term. Their respective running mates are Jim Cawley and Scott Conklin. U.S. Senate Race Page 3 U.S. Senator Arlen Specter (D) was defeated in the Democrat Primary Election by Congressman Joe Sestak. The Republican nominee is former Congressman Pat Toomey. The two are vying for a six-year term. Congressional Races Pages 4-9 Pennsylvania’s 19 seats in the US House of Representatives are filled in every even-year election for two- year terms. All but one incumbent is seeking re-election. The 7th Congressional District is the only “open election” among Pennsylvania’s Congressional Delegation. State Senate Races Pages 10-12 One-half of Pennsylvania’s 50 state Senate Districts are filled in each even-year election. 22 of the 25 state Senators in those districts facing election are seeking re-election, leaving three “open seats” – all three open seats are being defended by the Democrats. Seven members of the state Senate (3 Republican/4 Democrat) are unopposed for re-election. State House Races Pages 13-33 All of Pennsylvania’s 203 state House Districts are filled in each even-year election. There are 17 open seats – 7 defended by the Republicans and 10 defended by the Democrats. 77 members of the House (41 Republican/36 Democrat) are unopposed for re-election. ABOUT PEG PAC The Pennsylvania Business Council’s political endorsements, political contributions and political action are made by the affiliated PEG PAC. -
Coalition of Legislations for Energy Action Now 1,198 State Legislator Signatories Urging Congressional Action As of 25 January 2010
COALITION OF LEGISLATIONS FOR ENERGY ACTION NOW 1,198 STATE LEGISLATOR SIGNATORIES URGING CONGRESSIONAL ACTION AS OF 25 JANUARY 2010 Rep. Eddie Ableser, AZ Rep. David Baram, CT Rep. Karla Bigham, MN Sen. Paula Aboud, AZ Rep. Jeb Bardon, IN Sen. Stan Bingham, NC Rep. Joseph Abruzzo, FL Rep. Elias Barela, NM Rep. Jackie Biskupski, UT Rep. Alma Adams, NC Sen. David Baria, MS Rep. Clement Bissonnette, VT ViceChair, Commerce, Small Rep. Jeff Barker, OR Rep. Spencer Black, WI Business, and Entrepreneurship Rep. John Barnes, IN Chair, Assembly Natural Resources Rep. Herb Adams, ME Assm. Peter Barnes III, NJ Committee Sen. Amanda Aguirre, AZ Rep. Phil Barnhart, OR Rep. Richard D. Blanchard, ME Rep. Edith Ajello, RI Rep. Dick Barrett, MT Rep. Lynne Blankenbeker, NH Deputy Majority Leader Rep. John Bartlett, IN Sen. Patricia Blevins, DE Sen. Charles Albertson, NC Sen. Philip Bartlett, ME Senate Majority Leader Rep. Eliseo Lee Alcon, NM Senate Majority Leader Rep. Anders Blewett, MT Del. Kenneth Alexander, VA Rep. Brent Barton, OR Sen. Lawrence Bliss, ME Rep. Martha Alexander, NC Business and Labor, ViceChair Assm. Marty Block, CA Rep. Kelly Alexander Jr, NC Del. Kumar Barve, MD Assistant Majority Whip ViceChair, Water Resources and Majority Leader Rep. Anna Blodgett, ME Infrastructure Sen. Ray Basham, MI Rep. David Bly, MN Sen. Justin Alfond, ME ViceChair, Natural Resources and Del. Elizabeth Bobo, MD Del. Saqib Ali, MD Environmental Affairs Committee Chair, Land Use and Ethics Rep. Alma Allen, TX Sen. Christopher Bateman, NJ Subcommittee Rep. Lucy Allen, NC Sen. Alan Bates, OR Assm. -
1434 Legislative Journal—House October 17
COMMONWEALTH OF PENNSYLVANIA LEGISLATIVE JOURNAL WEDNESDAY, OCTOBER 17, 2018 SESSION OF 2018 202D OF THE GENERAL ASSEMBLY No. 46 HOUSE OF REPRESENTATIVES SENATE MESSAGE The House convened at 9:30 a.m., e.d.t. AMENDED HOUSE BILLS RETURNED FOR CONCURRENCE AND THE SPEAKER (MIKE TURZAI) REFERRED TO COMMITTEE ON RULES PRESIDING The clerk of the Senate, being introduced, returned HB 26, PRAYER PN 4146; HB 99, PN 4254; HB 149, PN 4251; HB 353, PN 3779; HB 1013, PN 4069; HB 1511, PN 4253; HB 1885, HON. HARRY READSHAW, member of the House of PN 4255; and HB 2075, PN 4249, with information that the Representatives, offered the following prayer: Senate has passed the same with amendment in which the concurrence of the House of Representatives is requested. Thank you, Mr. Speaker. Colleagues, I solicit your personal prayers, and let us SENATE MESSAGE remember the families of Representative Mike O'Brien and Representative Sid Kavulich not only today but in the weeks to HOUSE BILLS come. CONCURRED IN BY SENATE Let us pray. Father, our God, we cry out in our times of need, for hope in The clerk of the Senate, being introduced, returned HB 927, times of despair, for faith in times of doubt, for comfort in times PN 1080; HB 1539, PN 3353; HB 2049, PN 3127; and HB 2453, of grief, for grace in times of sin, and for love in times of PN 3590, with information that the Senate has passed the same loneliness. Answer our cry. Be our refuge and our help. Restore without amendment. -

JASON ALTMIRE - Democrat U.S
PENNSYLVANIANS FOR EFFECTIVE GOVERNMENT Guidebook to New Elected Officials 2006 November 13, 2006 © Copyright 2006 Pennsylvanians for Effective Government Table of Contents U.S. Senate New Members 3 U.S. House New Members 5 Pennsylvania State Senate New Members 8 Pennsylvania State House New Members 12 2 U.S. SENATE New Member 3 Bob Casey Jr. - Democrat U.S. Senate Residence: Scranton, PA Marital Status: Married to Terese Previous Occupation: 5th Grade Teacher, Inner City Philadelphia, Jesuit Volunteer Corps; Lawyer Prev. Political Exp.: Elected Auditor General in 1996 and re-elected in 2000; Ran unsuccessfully for the Democratic nomination for governor in 2002; Elected State Treasurer in 2004 Education: BA from The College of the Holy Cross in 1982, J.D. from Catholic University in 1988 Birthdate: April 13, 1960 Birthplace: Scranton, PA Religion: Catholic Other: Casey is the recipient of numerous awards, including the Beacon Mailing: Award from the Pennsylvania Child Care Association and the Spirit of Dr. P.O. Box 22469 Martin Luther King, Jr. Legacy Award from the Interdenominational Philadelphia, PA 19110 Ministers Conference. He has also been one of the state’s most outspoken advocates for affordable health insurance and better working 215 567- 4190 conditions, training and pay for nurses and nurses’ aides. [email protected] Election Victory: 58.7% - 41.3% Opponent: Rick Santorum www.bobcasey.com Incumbent: Rick Santorum (R) 4 U.S. HOUSE New Members 5 JASON ALTMIRE - Democrat U.S. House - PA District 4 Residence: North Hills Marital Status: Married Prev. Occupation: Healthcare Executive, Former Congressional Staffer. Prev. Political Experience: Legislative Assistant in the Capitol Hill office of U.S. -
Write-In Names Report 2020 GENERAL PRIMARY and SPECIAL ELECTION June 2, 2020 Philadelphia, Pennsylvania
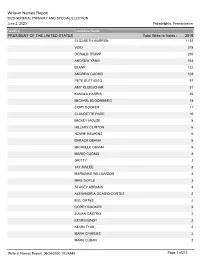
Write-in Names Report 2020 GENERAL PRIMARY AND SPECIAL ELECTION June 2, 2020 Philadelphia, Pennsylvania Heading Candidate Name PRESIDENT OF THE UNITED STATES Total Write-In Votes : 2515 ELIZABETH WARREN 1122 VOID 318 DONALD TRUMP 265 ANDREW YANG 163 BLANK 122 ANDREW CUOMO 103 PETE BUTTIGIEG 57 AMY KLOBUCHAR 31 KAMALA HARRIS 25 MICHAEL BLOOMBERG 18 CORY BOOKER 11 CLAUDETTE PAGE 10 MICKEY MOUSE 8 HILLARY CLINTON 6 HOWIE HAWKINS 6 BARACK OBAMA 5 MICHELLE OBAMA 5 MARIO CUOMO 4 GRITTY 3 JAY INSLEE 3 MARIANNE WILLIAMSON 3 MIKE DOYLE 3 STACEY ABRAMS 3 ALEXANDRIA OCASIO-CORTEZ 2 BILL GATES 2 COREY BOOKER 2 JULIAN CASTRO 2 KEVIN BUNDY 2 KEVIN TYAS 2 MARK CHARLES 2 MARK CUBAN 2 Write-in Names Report 06/24/2020 10:24AM Page 1 of212 Write-in Names Report 2020 GENERAL PRIMARY AND SPECIAL ELECTION June 2, 2020 Philadelphia, Pennsylvania Heading Candidate Name MUMIA ABU JAMAL 2 NATHAN SCHMIDT 2 OLGA MELENDEZ 2 PHIL MURPHY 2 RAHIEM S BURGESS 2 REBECCA L ZARNOWSKI 2 VAZQUEZ EMILIO 2 ADAM SCHIFF 1 AL GORE 1 ALBERT BRAUN 1 ALI MUHAMMAD 1 ANDREW FELTON 1 ANDREW GREGORY MAZUR 1 ANDREW THOMAS 1 ANNA GREENE 1 ANNALEE MAUSKGAT 1 ANNE SMALL 1 ANTHONY S RATKA 1 ANTONIO LIEGGI 1 AYISHA ABDULALI 1 BART WEAVER 1 BERNIE BROGDEN 1 BERNIE SAMPSON 1 BOB CASEY 1 BOB STRAUSS 1 BRAD PITT 1 BREE O NEIL 1 BRIAN WRIGHT 1 BRUCE BRADLEY II 1 BRUCE SPRINGSTEEN 1 BRUCE WAYNE 1 CARL BRUTANANADILEWSKI 1 Write-in Names Report 06/24/2020 10:24AM Page 2 of212 Write-in Names Report 2020 GENERAL PRIMARY AND SPECIAL ELECTION June 2, 2020 Philadelphia, Pennsylvania Heading Candidate Name -

Pennsylvania 2012 Prayer Calendar
Pennsylvania 2012 Prayer Calendar www.capitolcom.org Jeff Whitebread, State Director 1 2 3 4 5 6 7 Secretary of Economic State Leadership Department Heads Secretary of Education: Secretary of General Spiritual Executive Development: Governor: Tom Corbett Acting Secretary of Ronald Tomalis Services: C. Alan Walker Your Pastor(s) President: Lieutenant Governor: Aging: Sheri Philips Acting Secretary of Jim Cawley Brian Duke Secretary of Conservation Barack Obama Environmental Acting Secretary of Attorney General: And Natural Resources: Secretary of Agriculture: Protection: Health: Vice President: Linda Kelly Richard Allan George Greig Michael Krancer Dr. Eli Avila Auditor General: Joseph Biden Secretary of Corrections: Secretary of Banking: Insurance Commissioner: Jack Wagner John Wetzel Glenn Moyer Michael Consedine State Treasurer: Robin Wiessman 8 9 10 11 12 13 14 Secretary of Labor & Secretary of Public Secretary of State: Secretary of Legislative Secretary of Planning & Rep. Jason Altmire Industry: Welfare: Carol Aichele Affairs: Policy: Legislative Rep. Lou Barletta Julia Hearthway Gary Alexander Annemarie Kaiser Jennifer Branstetter Rep. Robert Brady Secretary of Congress Rep. Mark Critz Adjutant General of Acting Secretary of Transportation: Sec’y of Administration: Chief of State Police: Senator Pat Toomey Military Affairs; Revenue: Barry Schoch Kelly Logan Frank Noonan Senator Robert Casey Gen. Wesley Craig Dan Meuser 15 16 17 18 19 20 21 Rep. Charles Dent Rep. James Gerlach Rep. Patrick Meehan Rep. Allison Schwartz Justice Elena Kagan Justice Rep. Mike Dole Rep. Tim Holden Rep. Timothy Murphy Judicial Justice Anthony Kennedy Ruth Bader Ginsberg Rep. Bill Shuster Rep. Chaka Fattah Rep. Mike Kelly Rep. Joseph Pitts Rep. Glen Thompson US Supreme Court Justice Justice Stephen Breyer Rep.