Osteogenesis Imperfecta: Recent Findings Shed New Light on This Once Well-Understood Condition Donald Basel, Bsc, Mbbch1, and Robert D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Atypical Femur Fracture in an Adolescent Boy Treated with Bisphosphonates for X-Linked Osteoporosis Based on PLS3 Mutation Denise M
Atypical femur fracture in an adolescent boy treated with bisphosphonates for X-linked osteoporosis based on PLS3 mutation Denise M. van de Laarschot BSc1, M. Carola Zillikens MD PhD 1 1 Department of Internal Medicine, Erasmus MC, Rotterdam, The Netherlands Corresponding author at: Erasmus Medical Centre, PO Box 2040, 3000 CA Rotterdam, The Netherlands. Abstract Long-term use of bisphosphonates has raised concerns about the association with Atypical Femur Fractures (AFFs) that have been reported mainly in postmenopausal women. We report a case of an 18-year-old patient with juvenile osteoporosis based on X-linked osteoporosis due to a PLS3 mutation who developed a low trauma femoral fracture after seven years of intravenous and two years of oral bisphosphonate use, fulfilling the revised ASBMR diagnostic criteria of an AFF. The occurrence of AFFs has not been described previously in children or adolescents. The underlying monogenetic bone disease in our case strengthens the possibility of a genetic predisposition at least in some cases of AFF. We cannot exclude that a transverse fracture of the tibia that also occurred after a minor trauma at age 16 might be part of the same spectrum of atypical fractures related to the use of bisphosphonates. In retrospect our patient experienced prodromal pain prior to both the tibia and the femur fracture. Case reports of atypical fractures in children with a monogenetic bone disease such as Osteogenesis Imperfecta (OI) or juvenile osteoporosis are important to consider in the discussion about optimal -

Differential Diagnosis: Brittle Bone Conditions Other Than OI
Facts about Osteogenesis Imperfecta Differential Diagnosis: Brittle Bone Conditions Other than OI Fragile bones are the hallmark feature of osteogenesis imperfecta (OI). The mutations that cause OI lead to abnormalities within bone that result in increased bone turnover; reduced bone mineral content and decreased bone mineral density. The consequence of these changes is brittle bones that fracture easily. But not all cases of brittle bones are OI. Other causes of brittle bones include osteomalacia, disuse osteoporosis, disorders of increased bone density, defects of bone, and tumors. The following is a list of conditions that share fragile or brittle bones as a distinguishing feature. Brief descriptions and sources for further information are included. Bruck Syndrome This autosomal recessive disorder is also referred to as OI with contractures. Some people now consider this to be a type of OI. National Library of Medicine Genetics Home Reference: http://ghr.nlm.nih.gov Ehlers-Danlos Syndrome (EDS) Joint hyperextensibility with fractures; this is a variable disorder caused by several gene mutations. Ehlers-Danlos National Foundation http://www.ednf.org Fibrous Dysplasia Fibrous tissue develops in place of normal bone. This weakens the affected bone and causes it to deform or fracture. Fibrous Dysplasia Foundation: https://www.fibrousdysplasia.org Hypophosphatasia This autosomal recessive disorder affects the development of bones and teeth through defects in skeletal mineralization. Soft Bones: www.softbones.org; National Library of Medicine Genetics Home Reference: http://ghr.nlm.nih.gov/condition Idiopathic Juvenile Osteoporosis A non-hereditary transient form of childhood osteoporosis that is similar to mild OI (Type I) National Osteoporosis Foundation: www.nof.org McCune-Albright Syndrome This disorder affects the bones, skin, and several hormone-producing tissues. -

WO 2010/115932 Al
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 14 October 2010 (14.10.2010) WO 2010/115932 Al (51) International Patent Classification: AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, A61K 31/675 (2006.01) A61K 45/06 (2006.01) CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, A61K 38/00 (2006.01) A61P 19/08 (2006.01) DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, A61K 39/395 (2006.01) A61P 19/10 (2006.01) HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, (21) International Application Number: ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, PCT/EP20 10/054605 NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, (22) International Filing Date: SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, 7 April 2010 (07.04.2010) TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (26) Publication Language: English GM, KE, LR, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, (30) Priority Data: ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, 61/167,688 8 April 2009 (08.04.2009) US TM), European (AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, LV, (71) Applicant (for all designated States except US): NO- MC, MK, MT, NL, NO, PL, PT, RO, SE, SI, SK, SM, VARTIS AG [CH/CH]; Lichtstrasse 35, CH-4056 Basel TR), OAPI (BF, BJ, CF, CG, CI, CM, GA, GN, GQ, GW, (CH). -

Genetic Causes and Underlying Disease Mechanisms in Early-Onset Osteoporosis
From DEPARTMENT OF MOLECULAR MEDICINE AND SURGERY Karolinska Institutet, Stockholm, Sweden GENETIC CAUSES AND UNDERLYING DISEASE MECHANISMS IN EARLY-ONSET OSTEOPOROSIS ANDERS KÄMPE Stockholm 2020 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Eprint AB 2020 © Anders Kämpe, 2020 ISBN 978-91-7831-759-2 Genetic causes and underlying disease mechanisms in early-onset osteoporosis THESIS FOR DOCTORAL DEGREE (Ph.D.) By Anders Kämpe Principal Supervisor: Opponent: Professor Outi Mäkitie Professor André Uitterlinden Karolinska Institutet Erasmus Medical Centre, Rotterdam Department of Molecular Medicine and Surgery Department of Internal Medicine Laboratories Genetic Laboratory / Human Genomics Facility (HuGe-F) Co-supervisor(s): Examination Board: Associate Professor Anna Lindstrand Professor Marie-Louise Bondeson Karolinska Institutet Uppsala University Department of Molecular Medicine and Surgery Department of Immunology, Genetics and Pathology Associate Professor Giedre Grigelioniene Professor Göran Andersson Karolinska Institutet Karolinska Institutet Department of Molecular Medicine and Surgery Department of Laboratory Medicine Professor Ann Nordgren Minna Pöyhönen Karolinska Institutet University of Helsinki Department of Molecular Medicine and Surgery Department of Medical Genetics Associate Professor Hong Jiao Karolinska Institutet Department of Biosciences and Nutrition ABSTRACT Adult-onset osteoporosis is a disorder that affects a significant proportion of the elderly population worldwide and entails a substantial disease burden for the affected individuals. Childhood-onset osteoporosis is a rare condition often associating with a severe bone disease and recurrent fractures already in early childhood. Both childhood-onset and adult-onset osteoporosis have a large genetic component, but in children the disorder is usually genetically less complex and often caused by a single gene variant. -

Skeletal Dysplasias
Skeletal Dysplasias North Carolina Ultrasound Society Keisha L.B. Reddick, MD Wilmington Maternal Fetal Medicine Development of the Skeleton • 6 weeks – vertebrae • 7 weeks – skull • 8 wk – clavicle and mandible – Hyaline cartilage • Ossification – 7-12 wk – diaphysis appears – 12-16 wk metacarpals and metatarsals – 20+ wk pubis, calus, calcaneus • Visualization of epiphyseal ossification centers Epidemiology • Overall 9.1 per 1000 • Lethal 1.1 per 10,000 – Thanatophoric 1/40,000 – Osteogenesis Imperfecta 0.18 /10,000 – Campomelic 0.1 /0,000 – Achondrogenesis 0.1 /10,000 • Non-lethal – Achondroplasia 15 in 10,000 Most Common Skeletal Dysplasia • Thantophoric dysplasia 29% • Achondroplasia 15% • Osteogenesis imperfecta 14% • Achondrogenesis 9% • Campomelic dysplasia 2% Definition/Terms • Rhizomelia – proximal segment • Mezomelia –intermediate segment • Acromelia – distal segment • Micromelia – all segments • Campomelia – bowing of long bones • Preaxial – radial/thumb or tibial side • Postaxial – ulnar/little finger or fibular Long Bone Segments Counseling • Serial ultrasound • Genetic counseling • Genetic testing – Amniocentesis • Postnatal – Delivery center – Radiographs Assessment • Which segment is affected • Assessment of distal extremities • Any curvatures, fracture or clubbing noted • Are metaphyseal changes present • Hypoplastic or absent bones • Assessment of the spinal canal • Assessment of thorax. Skeletal Dysplasia Lethal Non-lethal • Thanatophoric • Achondroplasia • OI type II • OI type I, III, IV • Achondrogenesis • Hypochondroplasia -

Fetal Skeletal Dysplasias
There’s a Short Long Bone, What Now? Fetal Skeletal Dysplasias TERRY HARPER, MD DIVISION CHIEF CLINICAL ASSOCIATE PROFESSOR MATERNAL FETAL MEDICINE UNIVERSITY OF COLORADO Over 450 types of Skeletal Dysplasias X-linked Spondyloepiphyseal Tarda Thanatophoric dysplasia Osteogenesis Imperfecta Hypochondrogenesis Achondrogenesis Achondroplasia Otospondylomegaepiphyseal dysplasia Fibrochondrogenesis (OSMED) Hypochondroplasia Campomelic dysplasia Spondyloepiphyseal dysplasia congenita (SEDC) How will we come across this diagnosis? Third trimester size less than dates ultrasound at 33 4/7 weeks shows: What should our goal be at the initial visit? A. Genetic definitive diagnosis B. Termination of pregnancy C. Detailed anatomic survey including all long bones D. Assessment of likely lethality from pulmonary hypoplasia E. Amniocentesis or Serum Testing/Genetics Referral F. Referral to a Fetal Care Center What should our goal be at the initial visit? A. Genetic definitive diagnosis B. Termination of pregnancy C. Detailed anatomic survey including all long bones D. Assessment of likely lethality secondary to pulmonary hypoplasia E. Amniocentesis or Serum Testing/Genetics Referral F. Referral to a Fetal Care Center Detailed Ultrasound Technique Long bones Thorax Hands/feet Skull Spine Face Long bones Measure all including distal Look for missing bones Mineralization, curvature, fractures If limbs disproportional…. Does the abnormality effect: Proximal (rhizomelic) Middle (mesomelic) Distal (acromelic) Long bones Measure all extremities -

Non-Cardiac Manifestations of Marfan Syndrome
Keynote Lecture Series Non-cardiac manifestations of Marfan syndrome Anne H. Child Molecular and Clinical Sciences Research Institute, St George’s University of London, Cranmer Terrace, London, UK Correspondence to: Dr. Anne H. Child, MD, FRCP. Reader in Cardiovascular Genetics, Molecular and Clinical Sciences Research Institute, St George's University of London, Cranmer Terrace, London SW17 0RE, UK. Email: [email protected]. Because of the widespread distribution of fibrillin 1 in the body, Marfan syndrome (MFS) affects virtually every system. The expression of this single dominantly inherited gene is variable within a family, and between families. There is some genotype-phenotype correlation which is helpful in guiding long-term prognosis, and management. In general gene mutations have been reported in clusters, with those having mainly ocular manifestations occurring in exons 1 to 15 of this 65-exon gene; those causing cardiac problems often involving cysteine replacement in a calcium binding EGF-like sequence; the most severe mutations occurring in exons 25–32, causing neonatal MFS diagnosed at birth, and severe enough to cause death frequently before the age of 2. Other correlations will certainly be found in future. This condition is progressive, and the manifestations unfold according to age. For example, if the lens is going to dislocate this usually occurs by age 10; scoliosis usually presents itself between the ages of 8 and 15; height should be monitored carefully between the onset of puberty and cessation of growth approximately age 17 or 18. Holistic care should be offered by one doctor who oversees the patient’s welfare. This should be a paediatrician, paediatric cardiologist, or general practitioner in the case of an affected child. -

Current Overview of Osteogenesis Imperfecta
medicina Review Current Overview of Osteogenesis Imperfecta Mari Deguchi *, Shunichiro Tsuji , Daisuke Katsura , Kyoko Kasahara, Fuminori Kimura and Takashi Murakami Department of Obstetrics & Gynecology, Shiga University of Medical Science, Otsu 520-2192, Shiga, Japan; [email protected] (S.T.); [email protected] (D.K.); [email protected] (K.K.); [email protected] (F.K.); [email protected] (T.M.) * Correspondence: [email protected] Abstract: Osteogenesis imperfecta (OI), or brittle bone disease, is a heterogeneous disorder charac- terised by bone fragility, multiple fractures, bone deformity, and short stature. OI is a heterogeneous disorder primarily caused by mutations in the genes involved in the production of type 1 collagen. Severe OI is perinatally lethal, while mild OI can sometimes not be recognised until adulthood. Severe or lethal OI can usually be diagnosed using antenatal ultrasound and confirmed by various imaging modalities and genetic testing. The combination of imaging parameters obtained by ultrasound, computed tomography (CT), and magnetic resource imaging (MRI) can not only detect OI accurately but also predict lethality before birth. Moreover, genetic testing, either noninvasive or invasive, can further confirm the diagnosis prenatally. Early and precise diagnoses provide parents with more time to decide on reproductive options. The currently available postnatal treatments for OI are not curative, and individuals with severe OI suffer multiple fractures and bone deformities throughout their lives. In utero mesenchymal stem cell transplantation has been drawing attention as a promising therapy for severe OI, and a clinical trial to assess the safety and efficacy of cell therapy is currently ongoing. -
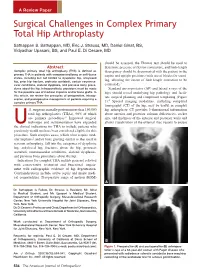
Surgical Challenges in Complex Primary Total Hip Arthroplasty
A Review Paper Surgical Challenges in Complex Primary Total Hip Arthroplasty Sathappan S. Sathappan, MD, Eric J. Strauss, MD, Daniel Ginat, BS, Vidyadhar Upasani, BS, and Paul E. Di Cesare, MD should be assessed, the Thomas test should be used to Abstract determine presence of flexion contracture, and limb-length Complex primary total hip arthroplasty (THA) is defined as discrepancy should be documented with the patient in the primary THA in patients with compromised bony or soft-tissue supine and upright positions (with use of blocks for stand- states, including but not limited to dysplastic hip, ankylosed hip, prior hip fracture, protrusio acetabuli, certain neuromus- ing, allowing the extent of limb-length correction to be 3 cular conditions, skeletal dysplasia, and previous bony proce- estimated). dures about the hip. Intraoperatively, provisions must be made Standard anteroposterior (AP) and lateral x-rays of the for the possible use of modular implants and/or bone grafts. In hips should reveal underlying hip pathology and facili- this article, we review the principles of preoperative, intraop- tate surgical planning and component templating (Figure erative, and postoperative management of patients requiring a 4 complex primary THA. 1). Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex .S. surgeons annually perform more than 150,000 hip arthroplasty. CT provides 3-dimensional information total hip arthroplasties (THAs), 90% of which about anterior and posterior column deficiencies, socket are primary procedures.1 Improved surgical size, and thickness of the anterior and posterior walls and technique and instrumentation have expanded allows visualization of the external iliac vessels to ensure Uthe clinical indications for THA to include patients who previously would not have been considered eligible for this procedure. -

Ultrasonic Demonstration of Fetal Skeletal Dysplasia Case Reports
222 SAMJ VOLUME 67 9 FEBRUARY 1985 Ultrasonic demonstration of fetal skeletal dysplasia Case reports L1NNIE M. MULLER, B. J. CREMIN Toshiba linear array scanners (with 3,5 mHz transducers) and a Philips SDU 7000 Sector/Static scanner. A routine obstetric Summary scan does not involve complete examination of all limbs, but Reports on prenatal diagnosis in cases of skeletal when a bony abnormality is noted a skeletal survey is dysplasia have mostly been in high-risk mothers attempted. Real-time ultrasound offers a flexible technique, with a suspect genetic background where the fetal and when the infant is in the prone vertex position the linear lesion could probably be predetermined. We deal array has the advantage of a wider range of skeletal visualiza with routine ultrasonographic appraisal of the fetal tion. skeleton when dysplasia is not initially suspected, A complete skeletal survey consists of an evaluation of the and relate our experience of the lethal forms of this bones of the skull, spine, thorax and limbs and of correlating these other fetal structures. We first measured the biparietal condition. During the 4-year period 1981 - 1984,6 cases of skeletal dysplasia, including thanatophoric diameter (BPD) and then noted the echogenic characteristics dysplasia, achondrogenesis, the Ellis-van Creveld of the skull and facial contours. A comprehensive evaluation of syndrome (chondro-ectodermal dysplasia) and the spine is possible from 17 weeks' gestation onwards. In a osteogenesis imperfecta, were detected; the ultra longitudinal plane the posterior elements form segmented sonographic findings are discussed. bands of echoes that conform to the fetal kyphosis, but it is not always possible to visualize the whole spine. -

Thieme: Teaching Atlas of Musculoskeletal Imaging
Teaching Atlas of Musculoskeletal Imaging Teaching Atlas of Musculoskeletal Imaging Peter L. Munk, M.D., C.M., F.R.C.P.C. Professor Departments of Radiology and Orthopaedics University of British Columbia Head Section of Musculoskeletal Radiology Vancouver General Hospital and Health Science Center Vancouver, British Columbia, Canada Anthony G. Ryan, M.B., B.C.H., B.A.O., F.R.C.S.I., M.Sc. (Engineering and Physical Sciences in Medicine), D.I.C., F.R.C.R., F.F.R.R.C.S.I. Consultant Musculoskeletal and Interventional Radiologist Waterford Regional Teaching Hospital Ardkeen, Waterford City, Republic of Ireland Radiologic Tutor and Clinical Instructor in Radiology The Royal College of Surgeons in Ireland Dublin, Republic of Ireland Thieme New York • Stuttgart [email protected] 66485438-66485457 Thieme Medical Publishers, Inc. 333 Seventh Ave. New York, NY 10001 Editor: Birgitta Brandenburg Assistant Editor: Ivy Ip Vice President, Production and Electronic Publishing: Anne T. Vinnicombe Production Editor: Print Matters, Inc. Vice President, International Marketing: Cornelia Schulze Sales Director: Ross Lumpkin Chief Financial Officer: Peter van Woerden President: Brian D. Scanlan Compositor: Compset, Inc. Printer: The Maple-Vail Book Manufacturing Group Library of Congress Cataloging-in-Publication Data Munk, Peter L. Teaching atlas of musculoskeletal imaging / Peter L. Munk, Anthony G. Ryan. p. ; cm. Includes bibliographical references and index. ISBN-13: 978-1-58890-372-3 (alk. paper) ISBN-10: 1-58890-372-9 (alk. paper) ISBN-13: 978-3-13-141981-1 (alk. paper) ISBN-10: 3-13-141981-4 (alk. paper) 1. Musculoskeletal system—Diseases—Imaging—Atlases. 2. Musculoskeletal system—Diseases—Case studies. -

2 Achondrogenesis, Type IB A
Achondrogenesis,Type IB 579 2 Achondrogenesis,Type IB A Fraccaro type Extremities • Extremely short tubular bones, with squared, Severely shortened long bones with loss of longitudi- trapezoid, or stellate appearance nal orientation; unossified fibulas; deficient ossifica- • Wide and cupped ends of the long bones, with lat- tion of vertebral bodies, pelvis, and sacrum eral spurs • Unossified fibulas Frequency: 1 in 50,000 births. Skull • Ossified or only mildly underossified calvarium Genetics Autosomal recessive (OMIM 600972), caused by mutations in the DTDST gene at 5q32-q33 Bibliography Clinical Features Beluffi G. Achondrogenesis, type I. Rofo Fortschr Geb Rönt- • Fetal hydrops, polyhydramnios genstr Nuklearmed 1977; 127: 341–4 • Borochowitz Z, Lachman R, Adominan GE, Spear G, Jones K, Premature birth, stillbirth or death within min- Rimoin DL. Achondrogenesis type I: delineation of further utes in large proportion of cases heterogeneity and identification of two distinct subgroups. • Marked micromelic dwarfism J Pediatr 1988; 112: 23–31 • Normocephaly, but head appearing large because Jaeger HJ, Schmitz-Stolbrink A, Hulde J, Novak M, Roggen- of small body kamp K, Mathias K. The boneless neonate: a severe form of • achondrogenesis type I. Pediatr Radiol 1994; 24: 319–21 Severe midface hypoplasia Maroteaux P, Lamy M: Le diagnostic des nanismes chrondro- • Low nasal bridge dystrophiques chez les nouveau-nés. Arch Fr Pediatr 1968; • Micrognathia 25: 241–62 • Short neck Spranger JW, Langer LO, Wiedemann HR. Bone dysplasias. An • Short trunk, barrel-shaped chest atlas of constitutional disorders of skeletal development. • W.B. Saunders Company, Philadelphia, 1974, pp. 24–5 Overdistended abdomen Superti-Furga A, Hastbacka J, Wilcox WR, Cohn DH, van der • Edema of soft tissues Harten HJ, Rossi A, Blau N, Rimoin DL, Steinmann B, Lan- • Prenatal detection of micromelia by ultrasound der ES, Gitzelmann R.