Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Review of Intra-Arterial Therapies for Colorectal Cancer Liver Metastasis
cancers Review Review of Intra-Arterial Therapies for Colorectal Cancer Liver Metastasis Justin Kwan * and Uei Pua Department of Vascular and Interventional Radiology, Tan Tock Seng Hospital, Singapore 388403, Singapore; [email protected] * Correspondence: [email protected] Simple Summary: Colorectal cancer liver metastasis occurs in more than 50% of patients with colorectal cancer and is thought to be the most common cause of death from this cancer. The mainstay of treatment for inoperable liver metastasis has been combination systemic chemotherapy with or without the addition of biological targeted therapy with a goal for disease downstaging, for potential curative resection, or more frequently, for disease control. For patients with dominant liver metastatic disease or limited extrahepatic disease, liver-directed intra-arterial therapies including hepatic arterial chemotherapy infusion, chemoembolization and radioembolization are alternative treatment strategies that have shown promising results, most commonly in the salvage setting in patients with chemo-refractory disease. In recent years, their role in the first-line setting in conjunction with concurrent systemic chemotherapy has also been explored. This review aims to provide an update on the current evidence regarding liver-directed intra-arterial treatment strategies and to discuss potential trends for the future. Abstract: The liver is frequently the most common site of metastasis in patients with colorectal cancer, occurring in more than 50% of patients. While surgical resection remains the only potential Citation: Kwan, J.; Pua, U. Review of curative option, it is only eligible in 15–20% of patients at presentation. In the past two decades, Intra-Arterial Therapies for Colorectal major advances in modern chemotherapy and personalized biological agents have improved overall Cancer Liver Metastasis. -
Residency Essentials Full Curriculum Syllabus
RESIDENCY ESSENTIALS FULL CURRICULUM SYLLABUS Please review your topic area to ensure all required sections are included in your module. You can also use this document to review the surrounding topics/sections to ensure fluidity. Click on the topic below to jump to that page. Clinical Topics • Gastrointestinal • Genitourinary • Men’s Health • Neurological • Oncology • Pain Management • Pediatrics • Vascular Arterial • Vascular Venous • Women’s Health Requisite Knowledge • Systems • Business and Law • Physician Wellness and Development • Research and Statistics Fundamental • Clinical Medicine • Intensive Care Medicine • Image-guided Interventions • Imaging and Anatomy Last revised: November 4, 2019 Gastrointestinal 1. Portal hypertension a) Pathophysiology (1) definition and normal pressures and gradients, MELD score (2) Prehepatic (a) Portal, SMV or Splenic (i) thrombosis (ii) stenosis (b) Isolated mesenteric venous hypertension (c) Arterioportal fistula (3) Sinusoidal (intrahepatic) (a) Cirrhosis (i) ETOH (ii) Non-alcoholic fatty liver disease (iii) Autoimmune (iv) Viral Hepatitis (v) Hemochromatosis (vi) Wilson's disease (b) Primary sclerosing cholangitis (c) Primary biliary cirrhosis (d) Schistosomiasis (e) Infiltrative liver disease (f) Drug/Toxin/Chemotherapy induced chronic liver disease (4) Post hepatic (a) Budd Chiari (Primary secondary) (b) IVC or cardiac etiology (5) Ectopic perianastomotic and stomal varices (6) Splenorenal shunt (7) Congenital portosystemic shunt (Abernethy malformation) b) Measuring portal pressure (1) Direct -

Treatment of Primary Liver Tumors and Liver Metastases, Part 1: Nuclear Medicine Techniques
CONTINUING EDUCATION Treatment of Primary Liver Tumors and Liver Metastases, Part 1: Nuclear Medicine Techniques Nicholas Voutsinas, Safet Lekperic, Sharon Barazani, Joseph J. Titano, Sherif I. Heiba, and Edward Kim Department of Radiology, Icahn School of Medicine at Mount Sinai Hospital, New York, New York Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the different indications for 90Y radioembolization, (2) the technical aspects of performing the therapy and pre-planning angiography, and (3) the follow-up imaging findings and potential complications. Financial Disclosure: Dr. Kim discloses serving as a consultant for BTG and Philips Healthcare and serving on the advisory board for BTG and Boston Scientific. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest. CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through November 2021. the exposure of normal liver parenchyma to radiation, and it places 90Y radioembolization is an increasingly used treatment for both the highest possible dose of radiation adjacent to the tumor when primary and metastatic malignancy in the liver. Understanding the appropriately targeted (2). Additionally, the limited tissue penetra- biophysical properties, dosing concerns, and imaging appearance tion makes intraarterial injection safer for medical personnel and of this treatment is important for interventional radiologists and nu- the patient’s family (4). -
Liver Embolization MODERATORS: DAVID M
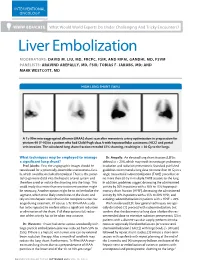
INTERVENTIONAL ONCOLOGY WWW EDUCATE What Would World Experts Do Under Challenging And Tricky Encounters? Liver Embolization MODERATORS: DAVID M. LIU, MD, FRCPC, FSIR, AND RIPAL GANDHI, MD, FSVM PANELISTS: ARAVIND AREPALLY, MD, FSIR; TOBIAS F. JAKOBS, MD; AND MARK WESTCOTT, MD HIGH LUNG SHUNT (36%) A Tc-99m microaggregated albumin (MAA) shunt scan after mesenteric artery optimization in preparation for yttrium-90 (Y-90) in a patient who had Child-Pugh class A with hepatocellular carcinoma (HCC) and portal vein invasion. The calculated lung shunt fraction revealed 37% shunting, resulting in > 30 Gy to the lungs. What techniques may be employed to manage Dr. Arepally: An elevated lung shunt fraction (LSF) is a significant lung shunt? defined as > 20%, which may result in nontarget pulmonary Prof. Jakobs: First, the angiographic images should be irradiation and radiation pneumonitis. Standard published reevaluated for a potentially detectable arteriovenous fistu- guidelines recommend a lung dose no more than 30 Gy in a la, which could be occluded/embolized. There is the poten- single transarterial radioembolization (TARE) procedure or tial to go more distal into the hepatic arterial system and no more than 50 Gy in multiple TARE sessions to the lung. therefore avoid or reduce the shunting into the lungs. This In addition, guidelines suggest decreasing the administered could imply that more than one treatment position might activity by 20% in patients with a 10% to 15% hepatopul- be necessary. Another option might be to coil embolize the monary shunt fraction (HPSF), decreasing the administered segment, which most likely contributes to the shunt, and activity by 40% in patients with a 15% to 20% HPSF, and rely on intrahepatic redistribution for complete tumor cov- avoiding radioembolization in patients with a HPSF > 20%. -

Neoadjuvant Transarterial Radiation Lobectomy for Colorectal Hepatic Metastases: a Small Cohort Analysis on Safety, Efficacy, and Radiopathologic Correlation
51 Case Report Neoadjuvant transarterial radiation lobectomy for colorectal hepatic metastases: a small cohort analysis on safety, efficacy, and radiopathologic correlation Jehan L. Shah1, Ivan R. Zendejas-Ruiz2, Linday M. Thornton1, Brian S. Geller1, Joseph R. Grajo1, Amy Collinsworth3, Thomas J. George Jr4, Beau Toskich1,5 1Department of Radiology, University of Florida, Post Office Box 100374, Gainesville, Florida 32610-0374, USA; 2Department of General Surgery, Innermountain Healthcare, Murray, UT 84107, USA; 3Department of Pathology, University of Florida, Immunology and Laboratory Medicine, Gainesville, FL 32608, USA; 4Department of Medicine, University of Florida, Gainesville, FL 32608, USA; 5Department of Radiology, Mayo Clinic, Jacksonville, FL 32224, USA Correspondence to: Jehan L. Shah, MD. Department of Radiology, University of Florida, Post Office Box 100374, Gainesville, Florida 32610-0374, USA. Email: [email protected]. Abstract: Colorectal cancer patients have a high incidence of liver metastasis (ml-CRC). Surgical resection is the gold standard for treatment of hepatic metastasis but only a small percent of patients are traditional candidates based on disease extent and adequate size of the future liver remnant (FLR). Interventions such as portal vein embolization (PVE) and associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) are performed to increase FLR for operative conversion. Limitations to PVE include intrahepatic disease progression, portal vascular invasion, and utilization with concurrent chemotherapy. ALPPS is associated with a high morbidly and mortality. Radiation lobectomy (RL) with yttrium-90 (Y-90) delivers transarterial ablative brachytherapy to the future hepatectomy site which generates FLR hypertrophy similar or greater than PVE. Early results indicate that RL is safe, effective, and may offer unique benefits by providing cytoreduction of hepatic metastases which extends FLR hypertrophy time and allows FLR surveillance to gauge disease biology. -

Safety of Selective Internal Radiation Therapy (SIRT) with Yttrium-90 Microspheres Combined with Systemic Anticancer Agents: Expert Consensus
1099 Review Article Safety of selective internal radiation therapy (SIRT) with yttrium-90 microspheres combined with systemic anticancer agents: expert consensus Andrew Kennedy1, Daniel B. Brown2, Jonas Feilchenfeldt3, John Marshall4, Harpreet Wasan5, Marwan Fakih6, Peter Gibbs7, Alexander Knuth3, Bruno Sangro8, Michael C. Soulen9, Gianfranco Pittari3, Ricky A. Sharma10 1Radiation Oncology Research, Sarah Cannon Research Institute, Nashville, Tennessee, USA; 2Department of Radiology and Radiologic Sciences, Vanderbilt University Medical Center, Nashville, Tennessee, USA; 3National Center for Cancer Care and Research, HMC, Doha, Qatar; 4Hematology and Oncology Lombardi Comprehensive Cancer Center, Georgetown University Medical Center, Washington DC, USA; 5Imperial College, Division of Cancer, Hammersmith Hospital, London, UK; 6Department of Medical Oncology & Therapeutics Research, City of Hope, Duarte, California, USA; 7Western Hospital, Footscray, Victoria, Australia; 8Liver Unit, Clinica Universidad de Navarra, IDISNA, CIBEREHD, Pamplona, Navarra, Spain; 9Abramson Cancer Center, University of Pennsylvania, Philadelphia, Pennsylvania, USA; 10NIHR University College London Hospitals Biomedical Research Centre, UCL Cancer Institute, University College London, London, UK Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Andrew Kennedy, MD. Physician in Chief, Radiation Oncology, Sarah Cannon Director, Radiation Oncology Research, Sarah Cannon Research Institute, 1100 Charlotte Avenue, Suite 800, Nashville, Tennessee 37203, USA. Email: [email protected]. Abstract: Selective internal radiation therapy (SIRT) with microspheres labelled with the β-emitter yttrium-90 (Y-90) enables targeted delivery of radiation to hepatic tumors. -

Yttrium-90 Selective Internal Radiation Therapy with Glass Microspheres
Review Article | Intervention http://dx.doi.org/10.3348/kjr.2016.17.4.472 pISSN 1229-6929 · eISSN 2005-8330 Korean J Radiol 2016;17(4):472-488 Yttrium-90 Selective Internal Radiation Therapy with Glass Microspheres for Hepatocellular Carcinoma: Current and Updated Literature Review Edward Wolfgang Lee, MD, PhD1*, Lourdes Alanis, MD, MPH1*, Sung-Ki Cho, MD2*, Sammy Saab, MD3* 1Division of Interventional Radiology, Department of Radiology, UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, USA; 2Division of Interventional Radiology, Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea; 3Division of Hepatology, Department of Medicine, Pfleger Liver Institute, University of California at Los Angeles, Los Angeles, CA 90024, USA Hepatocellular carcinoma is the most common primary liver cancer and it represents the majority of cancer-related deaths in the world. More than 70% of patients present at an advanced stage, beyond potentially curative options. Ytrrium-90 selective internal radiation therapy (Y90-SIRT) with glass microspheres is rapidly gaining acceptance as a potential therapy for intermediate and advanced stage primary hepatocellular carcinoma and liver metastases. The technique involves delivery of Y90 infused glass microspheres via the hepatic arterial blood flow to the appropriate tumor. The liver tumor receives a highly concentrated radiation dose while sparing the healthy liver parenchyma due to its preferential blood supply from portal venous blood. There are two commercially available devices: TheraSphere® and SIR-Spheres®. Although, Y90-SIRT with glass microspheres improves median survival in patients with intermediate and advanced hepatocellular carcinoma and has the potential to downstage hepatocellular carcinoma so that the selected candidates meet the transplantable criteria, it has not gained widespread acceptance due to the lack of large randomized controlled trials. -

Treatment of Primary Liver Tumors and Liver Metastases
Journal of Nuclear Medicine, published on August 2, 2018 as doi:10.2967/jnumed.116.186346 Interventional Oncology: Treatment of primary liver tumors and liver metastases. Part I: Nuclear medicine techniques (all about spheres) Running Title: Interventional Oncology and the Liver Authors: Nicholas Voutsinas MD Safet Lekperic MD Sharon Barazani BS Joseph J. Titano MD Sherif I. Heiba MD Edward Kim MD Affiliation for all authors: Department of Radiology, Icahn School of Medicine at Mount Sinai Hospital Corresponding and First Author: Nicholas Voutsinas MD PGY III 1 Gustave Levy Place Box 1234 New York, New York, 10029 [email protected] Manuscript Word Count (including figures and title page): 5125 Conflict of Interest Statement: Drs. Voutsinas, Lekperic, Titano and Heiba and Ms. Barazani report no potential conflicts of interest. Dr Kim discloses serving as a consultant for BTG and Philips Healthcare and serving on the advisory board for BTG and Boston Scientific. All the authors report that no outside funding was received for the creation of this manuscript. Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml. Abstract: Y-90 radioembolization is an increasingly utilized treatment for both primary and metastatic malignancy in the liver. Understanding the biophysical properties, dosing concerns, and imaging appearance of this treatment is important for interventional radiologists and nuclear medicine physicians to provide important therapy. Y-90 radioembolization is efficacious and safe, although the possibility of complications does exist. -
Imaging Evaluation Following 90Y Radioembolization of Liver Tumors
Review Article | Intervention https://doi.org/10.3348/kjr.2018.19.2.209 pISSN 1229-6929 · eISSN 2005-8330 Korean J Radiol 2018;19(2):209-222 Imaging Evaluation Following 90Y Radioembolization of Liver Tumors: What Radiologists Should Know Ijin Joo, MD1, Hyo-Cheol Kim, MD1, Gyoung Min Kim, MD2, Jin Chul Paeng, MD3 Departments of 1Radiology and 3Nuclear Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea; 2Department of Radiology, Severance Hospital, Seoul 03722, Korea Radioembolization using beta-emitting yttrium-90 microspheres is being increasingly used for the treatment of primary and metastatic liver cancers. It is a form of intra-arterial brachytherapy which delivers intense radiation to liver tumors with little embolic effect; this mode of action results in unique post-treatment imaging findings. It is important to understand these imaging findings to avoid misinterpretation of tumor response and to determine further management of the disease. Herein, we discuss the current concepts for assessing tumor response, common post-treatment imaging features, and associated complications following radioembolization. Keywords: Radioembolization; Yttrium-90; Selective internal radiation therapy; Liver cancer; Post-treatment imaging INTRODUCTION optimal radiation effects (3, 4). As a form of brachytherapy, radioembolization can Radioembolization, an increasingly used treatment option cause radiation-related changes in the adjacent structures for primary and metastatic liver cancers, involves intra- around the target lesion (5, 6). Moreover, the delivery of arterial delivery of microspheres containing yttrium-90 (90Y), radioactive microspheres to non-target organs can cause a high-energy pure beta-emitter (1, 2). Technical similarity complications such as cholecystitis and gastrointestinal to chemoembolization may be deduced based on the term ulceration (5, 6). -

Simultaneous 90Y and 99Mtc-MAA Injection for Two-Stage Selective Internal Radiation Therapy (SIRT) of Liver Metastases
Original Article Technical note: simultaneous 90Y and 99mTc-MAA injection for two-stage selective internal radiation therapy (SIRT) of liver metastases Arash Eftekhari, Daniel Worsley, Darren Klass, David M. Liu Department of Radiology, Faculty of Medicine, University of British Columbia, Vancouver, Canada Correspondence to: Arash Eftekhari, MD. Department of Radiology, Faculty of Medicine, University of British Columbia, 3350-950 W 10th Avenue, Vancouver BC V5Z 4E3, Canada. Email: [email protected]. Abstract: Transarterial Radioembolization (TARE) with 90-Yttrium (90Y) microspheres has been established in the management paradigm of a number of primary and metastatic liver neoplasms. Prior to treatment, angiographic assessment and 99mTc-macroaggregated albumin (Tc-MAA) hepatic arterial perfusion should be performed to detect extrahepatic shunting to the gastrointestinal tract or the lungs. Whole- liver radioembolization is not desirable in subjects with compromised hepatic reserve due to the increased likelihood of RE induced liver disease. In cases with diffuse hepatic involvement, superselective segmental and/or sequential lobar TARE is often utilized to decrease the side-effect profile with intra-arterial Tc-MAA injection playing a critical role in confirming pulmonary shunt fraction and the possibility of non-targeted embolization. Given the complexities of treatment planning, and in order to improve on the efficiencies of treatment without compromising safety, the feasibility of simultaneous 90Y RE and Tc-MAA injection into another segment/lobe for subsequent (second stage) treatment planning would be desirable to minimize additional angiography sessions. Here we present our initial experience with two patients undergoing sequential staged TARE therapy for diffuse hepatic metastases. Keywords: Transarterial Radioembolization (TARE); 90Y microspheres; 99mTc-MAA; two-stage; liver neoplasms Submitted Jun 07, 2013. -
International Recommendations for Personalised Selective Internal Radiation Therapy of Primary and Metastatic Liver Diseases with Yttrium-90 Resin Microspheres
European Journal of Nuclear Medicine and Molecular Imaging https://doi.org/10.1007/s00259-020-05163-5 GUIDELINES International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres Hugo Levillain1 & Oreste Bagni2 & Christophe M. Deroose3 & Arnaud Dieudonné4 & Silvano Gnesin5 & Oliver S. Grosser6 & S. Cheenu Kappadath7 & Andrew Kennedy8 & Nima Kokabi9 & David M. Liu10 & David C. Madoff11 & Armeen Mahvash12 & Antonio Martinez de la Cuesta13 & David C. E. Ng14 & Philipp M. Paprottka 15 & Cinzia Pettinato16 & Macarena Rodríguez-Fraile13 & Riad Salem17 & Bruno Sangro13 & Lidia Strigari18 & Daniel Y. Sze19 & Berlinda J. de Wit van der veen20 & Patrick Flamen 1 Received: 11 September 2020 /Accepted: 8 December 2020 # The Author(s) 2021 Abstract Purpose A multidisciplinary expert panel convened to formulate state-of-the-art recommendations for optimisation of selective internal radiation therapy (SIRT) with yttrium-90 (90Y)-resin microspheres. Methods A steering committee of 23 international experts representing all participating specialties formulated recommendations for SIRT with 90Y-resin microspheres activity prescription and post-treatment dosimetry, based on literature searches and the responses to a 61-question survey that was completed by 43 leading experts (including the steering committee members). The survey was validated by the steering committee and completed anonymously. In a face-to-face meeting, the results of the survey were presented and -

S00259-020-05163-5.Pdf
European Journal of Nuclear Medicine and Molecular Imaging (2021) 48:1570–1584 https://doi.org/10.1007/s00259-020-05163-5 GUIDELINES International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres Hugo Levillain1 & Oreste Bagni2 & Christophe M. Deroose3 & Arnaud Dieudonné4 & Silvano Gnesin5 & Oliver S. Grosser6 & S. Cheenu Kappadath7 & Andrew Kennedy8 & Nima Kokabi9 & David M. Liu10 & David C. Madoff11 & Armeen Mahvash12 & Antonio Martinez de la Cuesta13 & David C. E. Ng14 & Philipp M. Paprottka 15 & Cinzia Pettinato16 & Macarena Rodríguez-Fraile13 & Riad Salem17 & Bruno Sangro13 & Lidia Strigari18 & Daniel Y. Sze19 & Berlinda J. de Wit van der veen20 & Patrick Flamen 1 Received: 11 September 2020 /Accepted: 8 December 2020 / Published online: 12 January 2021 # The Author(s) 2021 Abstract Purpose A multidisciplinary expert panel convened to formulate state-of-the-art recommendations for optimisation of selective internal radiation therapy (SIRT) with yttrium-90 (90Y)-resin microspheres. Methods A steering committee of 23 international experts representing all participating specialties formulated recommendations for SIRT with 90Y-resin microspheres activity prescription and post-treatment dosimetry, based on literature searches and the responses to a 61-question survey that was completed by 43 leading experts (including the steering committee members). The survey was validated by the steering committee and completed anonymously. In a face-to-face