HHDW ICD-10 Code Documentation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
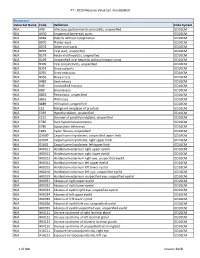
PT - 2020 Measure Value Set Avoidableed
PT - 2020 Measure Value Set_AvoidableED Numerator Value Set Name Code Definition Code System N/A A09 Infectious gastroenteritis and colitis, unspecified ICD10CM N/A A630 Anogenital (venereal) warts ICD10CM N/A B069 Rubella without complication ICD10CM N/A B070 Plantar wart ICD10CM N/A B078 Other viral warts ICD10CM N/A B079 Viral wart, unspecified ICD10CM N/A B179 Acute viral hepatitis, unspecified ICD10CM N/A B199 Unspecified viral hepatitis without hepatic coma ICD10CM N/A B309 Viral conjunctivitis, unspecified ICD10CM N/A B354 Tinea corporis ICD10CM N/A B355 Tinea imbricata ICD10CM N/A B356 Tinea cruris ICD10CM N/A B483 Geotrichosis ICD10CM N/A B49 Unspecified mycosis ICD10CM N/A B80 Enterobiasis ICD10CM N/A B852 Pediculosis, unspecified ICD10CM N/A B853 Phthiriasis ICD10CM N/A B889 Infestation, unspecified ICD10CM N/A C61 Malignant neoplasm of prostate ICD10CM N/A E039 Hypothyroidism, unspecified ICD10CM N/A E215 Disorder of parathyroid gland, unspecified ICD10CM N/A E780 Pure hypercholesterolemia ICD10CM N/A E786 Lipoprotein deficiency ICD10CM N/A E849 Cystic fibrosis, unspecified ICD10CM N/A G5600 Carpal tunnel syndrome, unspecified upper limb ICD10CM N/A G5601 Carpal tunnel syndrome, right upper limb ICD10CM N/A G5602 Carpal tunnel syndrome, left upper limb ICD10CM N/A H00011 Hordeolum externum right upper eyelid ICD10CM N/A H00012 Hordeolum externum right lower eyelid ICD10CM N/A H00013 Hordeolum externum right eye, unspecified eyelid ICD10CM N/A H00014 Hordeolum externum left upper eyelid ICD10CM N/A H00015 Hordeolum externum -

EAACI/ESCD Skin Allergy Meeting 2017 (SAM 2017)
Clin Transl Allergy 2017, 7(Suppl 4):47 DOI 10.1186/s13601-017-0184-5 Clinical and Translational Allergy MEETING ABSTRACTS Open Access EAACI/ESCD Skin Allergy Meeting 2017 (SAM 2017) Zurich, Switzerland. 27 – 29 April 2017 Published: 15 December 2017 Thursday, 27 April 2017 O02 Assessment of aggregate consumer exposure to isothiazolinones O01 via cosmetics and detergents Methylisothiazolinone contact allergy: a real outbreak Elena Garcia Hidalgo, Natalie Von Goetz, Konrad Hungerbühler Luis Amaral1, Emidio Silva2, Marcio Oliveira3, Ana Paula Cunha4 ETH Zürich, Zürich, Switzerland 1Serviço de Imunoalergologia, Centro Hospitalar de São João E.P.E., Porto, Correspondence: Elena Garcia Hidalgo ‑ [email protected] Portugal; 2Serviço de Medicina do Trabalho e Saúde Ocupacional, Centro Clinical and Translational Allergy 2017, 7(Supple 4):O02 Hospitalar do Baixo Vouga E.P.E., Aveiro, Portugal; 3Serviço de Saúde Ocu‑ pacional, Centro Hospitalar de São João E.P.E., Porto, Portugal; 4Serviço de Background: Isothiazoliones can cause allergic contact dermati- Dermatologia, Centro Hospitalar de São João E.P.E., Porto, Portugal tis and are present in a variety of consumer products, such as cos- Correspondence: Luis Amaral ‑ [email protected] metics, detergents and do-it-yourself products. Skin sensitization Clinical and Translational Allergy 2017, 7(Supple 4):O01 is induced following dermal exposure to a sensitizer in an amount exceeding the sensitization threshold. The critical determinant of Background: Methylisothiazolinone (MI) is used as a preservative in exposure for evaluating skin sensitization risks is dose per unit area occupational, domestic products and, since 2005, in cosmetics. It is a of exposed skin. -

Lameness in Fattening Pigs – Mycoplasma Hyosynoviae, Osteochondropathy and Reduced Dietary Phosphorus Level As Three Infuencing Factors: a Case Report
Lameness in fattening pigs – Mycoplasma hyosynoviae, osteochondropathy and reduced dietary phosphorus level as three inuencing factors: A case report Birte Wegner Veterinary Practice Duemmerland Jörg Tenhündfeld Vetland Dr. Tenhündfeld & Kollegen Johanna Vogels Stiftung Tierarztliche Hochschule Hannover Marius Beumer Stiftung Tierarztliche Hochschule Hannover Josef Kamphues Stiftung Tierarztliche Hochschule Hannover Florian Hansmann Stiftung Tierarztliche Hochschule Hannover Hanna Rieger Stiftung Tierarztliche Hochschule Hannover Elisabeth grosse Beilage Stiftung Tierarztliche Hochschule Hannover Isabel Hennig-Pauka ( [email protected] ) University of Veterinary Medicine Hannover https://orcid.org/0000-0003-3994-5979 Case report Keywords: Locomotor disorder, mineral supply, Mycoplasma hyosynoviae, nutrition, swine Posted Date: September 25th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-35962/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/28 Version of Record: A version of this preprint was published on December 15th, 2020. See the published version at https://doi.org/10.1186/s40813-020-00184-w. Page 2/28 Abstract Background: Multiple diagnostic procedures, their results and interpretation in a case with severe lameness in fattening pigs are described. It is shown that selected diagnostic steps lead to identication of various risk factors for disease development in the affected herd. One focus of this case report is the prioritization of diagnostic steps to verify the impact of the different conditions, which nally led to the clinical disorder. Disease is the consequence of previously acting factors, and the involved diagnostic institute is the last stage in the timeline. Some diagnostic ndings might therefore no longer be signicant. -

Download WAO White Book on Allergy
WORLD ALLERGY ORGANIZATION WAWAOO WhiteWhite BookBook onon AllergyAllergy WAO White Book on Allergy World Allergy Organization (WAO) White Book on Allergy Copyright 2011 World Allergy Organization WAO White Book on Allergy Editors Prof. Ruby Pawankar, MD, PhD Prof. Giorgio Walter Canonica, MD WAO President Elect (2010-2011) WAO Past President (2010-2011) Allergy and Rhinology Allergy & Respiratory Diseases Nippon Medical School Department of Internal Medicine 1-1-5 Sendagi, Bunkyo-ku University of Genoa Tokyo 113-8603 Padiglione Maragliano, Largo Rosanna Benzi 10 JAPAN 1-16132 Genoa ITALY Prof. Stephen T. Holgate, BSc, MD, DSc, FMed Sci Prof. Richard F. Lockey, MD Member, WAO Board of Directors (2010-2011) WAO President (2010-2011) Medical Research Council Clinical Professor of Division of Allergy & Immunology Immunopharmacology Joy McCann Culverhouse Chair in Allergy & Immunology Infection, Inflammation and Immunity University of South Florida College of Medicine School of Medicine James Haley Veterans Administration Medical Center (111D) University of Southampton 13000 Bruce B. Downs Boulevard Level F, South Block Tampa, Florida 33612 Southampton General Hospital USA Tremona Road Southampton SO16 6YD United Kingdom Acknowledgement On behalf of the World Allergy Organization (WAO), the editors and authors of the WAO White Book on Allergy express their gratitude to the charity, Asthma, Allergy, Inflammation Research (AAIR) and Asian Allergy Asthma Foundation (AAAF) for their support in the production of this publication. The Editors of the White book extend their gratitude to His Excellency Dr. APJ Abdul Kalam, Former President of India and Madame Ilora Finlay Baronness of the House of Lords for their Forewords to the White Book and to the International Primary Care Respiratory Group (IPCRG) and European Federation of Allergy and Airways Diseases Patients ‘Associations (EFA) for their supporting statements. -

N35.12 Postinfective Urethral Stricture, NEC, Female N35.811 Other
N35.12 Postinfective urethral stricture, NEC, female N35.811 Other urethral stricture, male, meatal N35.812 Other urethral bulbous stricture, male N35.813 Other membranous urethral stricture, male N35.814 Other anterior urethral stricture, male, anterior N35.816 Other urethral stricture, male, overlapping sites N35.819 Other urethral stricture, male, unspecified site N35.82 Other urethral stricture, female N35.911 Unspecified urethral stricture, male, meatal N35.912 Unspecified bulbous urethral stricture, male N35.913 Unspecified membranous urethral stricture, male N35.914 Unspecified anterior urethral stricture, male N35.916 Unspecified urethral stricture, male, overlapping sites N35.919 Unspecified urethral stricture, male, unspecified site N35.92 Unspecified urethral stricture, female N36.0 Urethral fistula N36.1 Urethral diverticulum N36.2 Urethral caruncle N36.41 Hypermobility of urethra N36.42 Intrinsic sphincter deficiency (ISD) N36.43 Combined hypermobility of urethra and intrns sphincter defic N36.44 Muscular disorders of urethra N36.5 Urethral false passage N36.8 Other specified disorders of urethra N36.9 Urethral disorder, unspecified N37 Urethral disorders in diseases classified elsewhere N39.0 Urinary tract infection, site not specified N39.3 Stress incontinence (female) (male) N39.41 Urge incontinence N39.42 Incontinence without sensory awareness N39.43 Post-void dribbling N39.44 Nocturnal enuresis N39.45 Continuous leakage N39.46 Mixed incontinence N39.490 Overflow incontinence N39.491 Coital incontinence N39.492 Postural -
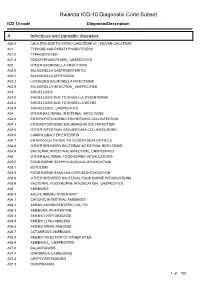
Rwanda ICD-10 Diagnostic Code Subset
Rwanda ICD-10 Diagnostic Code Subset ICD 10 code Diagnosis/Description A Infectious and parasitic diseases A00.0 CHOLERA DUE TO VIBRIO CHOLERAE 01_ BIOVAR CHOLERAE A01 TYPHOID AND PARATYPHOID FEVERS A01.0 TYPHOID FEVER A01.4 PARATYPHOID FEVER_ UNSPECIFIED A02 OTHER SALMONELLA INFECTIONS A02.0 SALMONELLA GASTROENTERITIS A02.1 SALMONELLA SEPTICEMIA A02.2 LOCALIZED SALMONELLA INFECTIONS A02.9 SALMONELLA INFECTION_ UNSPECIFIED A03 SHIGELLOSIS A03.0 SHIGELLOSIS DUE TO SHIGELLA DYSENTERIAE A03.2 SHIGELLOSIS DUE TO SHIGELLA BOYDII A03.9 SHIGELLOSIS_ UNSPECIFIED A04 OTHER BACTERIAL INTESTINAL INFECTIONS A04.0 ENTEROPATHOGENIC ESCHERICHIA COLI INFECTION A04.1 ENTEROTOXIGENIC ESCHERICHIA COLI INFECTION A04.4 OTHER INTESTINAL ESCHERICHIA COLI INFECTIONS A04.5 CAMPYLOBACTER ENTERITIS A04.7 ENTEROCOLITIS DUE TO CLOSTRIDIUM DIFFICILE A04.8 OTHER SPECIFIED BACTERIAL INTESTINAL INFECTIONS A04.9 BACTERIAL INTESTINAL INFECTION_ UNSPECIFIED A05 OTHER BACTERIAL FOOD-BORNE INTOXICATIONS A05.0 FOOD-BORNE STAPHYLOCOCCAL INTOXICATION A05.1 BOTULISM A05.4 FOOD-BORNE BACILLUS CEREUS INTOXICATION A05.8 OTHER SPECIFIED BACTERIAL FOOD-BORNE INTOXICATIONS A05.9 BACTERIAL FOOD-BORNE INTOXICATION_ UNSPECIFIED A06 AMEBIASIS A06.0 ACUTE AMEBIC DYSENTERY A06.1 CHRONIC INTESTINAL AMEBIASIS A06.2 AMEBIC NONDYSENTERIC COLITIS A06.3 AMEBOMA OF INTESTINE A06.4 AMEBIC LIVER ABSCESS A06.5 AMEBIC LUNG ABSCESS A06.6 AMEBIC BRAIN ABSCESS A06.7 CUTANEOUS AMEBIASIS A06.8 AMEBIC INFECTION OF OTHER SITES A06.9 AMEBIASIS_ UNSPECIFIED A07.0 BALANTIDIASIS A07.1 GIARDIASIS [LAMBLIASIS] -

Frequency and Criticality of Diagnoses in Family Medicine Practices: from the National Ambulatory Medical Care Survey (NAMCS)
J Am Board Fam Med: first published as 10.3122/jabfm.2018.01.170209 on 12 January 2018. Downloaded from ORIGINAL RESEARCH Frequency and Criticality of Diagnoses in Family Medicine Practices: From the National Ambulatory Medical Care Survey (NAMCS) Michael R. Peabody, PhD, Thomas R. O’Neill, PhD, Keith L. Stelter, MD, MMM, and James C. Puffer, MD Background: Family medicine is a specialty of breadth, providing comprehensive health care for the individual and the family that integrates the broad scope of clinical, social, and behavioral sciences. As such, the scope of practice (SOP) for family medicine is extensive; however, over time many family phy- sicians narrow their SOP. We sought to provide a nationally representative description of the most com- mon and the most critical diagnoses that family physicians see in their practice. Methods: Data were extracted from the 2012 National Ambulatory Medical Care Survey (NAMCS) to select all ICD-9 codes reported by family physicians. A panel of family physicians then reviewed 1893 ICD-9 codes to place each code into an American Board of Family Medicine Family Medicine Certifica- tion Examination test plan specifications (TPS) category and provide a rating for an Index of Harm (IoH). Results: An analysis of all 1893 ICD-9 codes seen by family physicians in the 2012 NAMCS found that 198 ICD-9 codes could not be assigned a TPS category, leaving 1695 ICD-9 codes in the dataset. Top 10 lists of ICD-9 codes by TPS category were created for both frequency and IoH. Conclusions: This study provides a nationally representative description of the most common diag- copyright. -

Successful Treatment of Genital Pruritus Using Topical Immunomodulators As a Single Therapy in Multi-Morbid Patients
Letters to the Editor 195 Successful Treatment of Genital Pruritus Using Topical Immunomodulators as a Single Therapy in Multi-morbid Patients Elke Weisshaar Clinical Social Medicine, Occupational and Environmental Dermatology, University Hospital Heidelberg, Thibautstrasse 3, DE-69115 Heidelberg, Germany. E-mail: [email protected] Accepted October 29, 2007. Sir, origin. He had been suffering from arterial hyperten- Anogenital pruritus is defined as pruritus affecting the skin sion, recurrent back pain and occasional heartburn. of the anus, perianal and genital area. In men it frequently Various topical treatments, including glucocortico- presents as scrotal pruritus and in females as vulval steroids and pimecrolimus 1% cream, did not relieve his pruritus. It may be caused by skin diseases (e.g. eczema, scrotal pruritus. Because of the history of encephalitis psoriasis, irritant or allergic contact dermatitis), infections he rejected any further diagnostic tests and systemic (e.g. candidiasis, parasitosis, lichen sclerosus, prema- treatments and requested symptomatic relief. The lignant or malignant conditions), as well as by systemic scrotum showed mild lichenifications. Topical tacro- diseases. Age, especially in female patients, determines limus 0.03% was started twice daily and the pruritus the initial most common differential diagnoses that need resolved completely within 2 weeks (VAS 0). After 6 to be considered (1). Acute genital pruritus is often caused weeks he continued to apply tacrolimus 0.03% twice a by infections, allergic or irritant contact dermatitis, leading week for a further period of 8 weeks. He has now been to prompt resolution after causal therapy. In a number of almost free of pruritus for one year and uses tacrolimus patients no underlying disease can be identified and the approximately 3 applications a week every 2 months condition is termed “pruritus of undetermined origin”. -

Immunopathologic Studies in Relapsing Polychondritis
Immunopathologic Studies in Relapsing Polychondritis Jerome H. Herman, Marie V. Dennis J Clin Invest. 1973;52(3):549-558. https://doi.org/10.1172/JCI107215. Research Article Serial studies have been performed on three patients with relapsing polychondritis in an attempt to define a potential immunopathologic role for degradation constituents of cartilage in the causation and/or perpetuation of the inflammation observed. Crude proteoglycan preparations derived by disruptive and differential centrifugation techniques from human costal cartilage, intact chondrocytes grown as monolayers, their homogenates and products of synthesis provided antigenic material for investigation. Circulating antibody to such antigens could not be detected by immunodiffusion, hemagglutination, immunofluorescence or complement mediated chondrocyte cytotoxicity as assessed by 51Cr release. Similarly, radiolabeled incorporation studies attempting to detect de novo synthesis of such antibody by circulating peripheral blood lymphocytes as assessed by radioimmunodiffusion, immune absorption to neuraminidase treated and untreated chondrocytes and immune coprecipitation were negative. Delayed hypersensitivity to cartilage constituents was studied by peripheral lymphocyte transformation employing [3H]thymidine incorporation and the release of macrophage aggregation factor. Positive results were obtained which correlated with periods of overt disease activity. Similar results were observed in patients with classical rheumatoid arthritis manifesting destructive articular changes. This study suggests that cartilage antigenic components may facilitate perpetuation of cartilage inflammation by cellular immune mechanisms. Find the latest version: https://jci.me/107215/pdf Immunopathologic Studies in Relapsing Polychondritis JERoME H. HERmAN and MARIE V. DENNIS From the Division of Immunology, Department of Internal Medicine, University of Cincinnati Medical Center, Cincinnati, Ohio 45229 A B S T R A C T Serial studies have been performed on as hematologic and serologic disturbances. -

Are Serum Aluminum Levels a Risk Factor in the Appearance of Spontaneous Pneumothorax?
Turk J Med Sci 2010; 40 (3): 459-463 Original Article © TÜBİTAK E-mail: [email protected] doi:10.3906/sag-0901-11 Are serum aluminum levels a risk factor in the appearance of spontaneous pneumothorax? Serdar HAN1, Rasih YAZKAN2, Bülent KOÇER3,*, Gültekin GÜLBAHAR3, Serdal Kenan KÖSE4, Koray DURAL3, Ünal SAKINCI3 Aim: To investigate the relationship between aluminum and spontaneous pneumothorax (SP) development. Materials and methods: A patient group and a control group were formed with 100 individuals in each. The serum aluminum levels of the groups were determined and statistically compared. Results: The mean serum aluminum levels were 5.6 ± 2.4 μg/L (1.6-11.9) and 23.2 ± 15.4 μg/L (2-81) in the control and SP groups, respectively (P < 0.001). The specificity and sensitivity of the measurement of aluminum level were 74.4% and 86.4% in the SP group. The risk of SP development was found to be 18 times higher in individuals with high serum levels of aluminum compared to that in individuals with low serum levels of aluminum. Conclusion: A high level of aluminum is a risk factor for the development of SP. Key words: Aluminum, pneumothorax, public health Spontan pnömotoraks gelişiminde serum aluminyum seviyeleri bir risk faktörü müdür? Amaç: Bu çalışmada spontan pnömotoraks (SP) gelişimi ile serum aluminyum düzeyleri arasındaki ilişkinin analiz edilmesi amaçlandı. Yöntem ve gereç: Yüz SP hastasından oluşan hasta grubunun yanı sıra 100 kişiden oluşan sağlıklı kontrol grubu çalışmaya dahil edildi. Gruplar serum aluminyum düzeyleri açısından istatistiksel olarak kıyaslandı. Bulgular: Ortalama serum aluminyum düzeyleri SP ve kontrol grupları için sırasıyla 5,6 ± 2,4 μg/L (1,6-11,9) ve 23,2 ± 15,4 μg/L (2-81) bulundu (P < 0,001). -

Diseases of the Digestive System (KOO-K93)
CHAPTER XI Diseases of the digestive system (KOO-K93) Diseases of oral cavity, salivary glands and jaws (KOO-K14) lijell Diseases of pulp and periapical tissues 1m Dentofacial anomalies [including malocclusion] Excludes: hemifacial atrophy or hypertrophy (Q67.4) K07 .0 Major anomalies of jaw size Hyperplasia, hypoplasia: • mandibular • maxillary Macrognathism (mandibular)(maxillary) Micrognathism (mandibular)( maxillary) Excludes: acromegaly (E22.0) Robin's syndrome (087.07) K07 .1 Anomalies of jaw-cranial base relationship Asymmetry of jaw Prognathism (mandibular)( maxillary) Retrognathism (mandibular)(maxillary) K07.2 Anomalies of dental arch relationship Cross bite (anterior)(posterior) Dis to-occlusion Mesio-occlusion Midline deviation of dental arch Openbite (anterior )(posterior) Overbite (excessive): • deep • horizontal • vertical Overjet Posterior lingual occlusion of mandibular teeth 289 ICO-N A K07.3 Anomalies of tooth position Crowding Diastema Displacement of tooth or teeth Rotation Spacing, abnormal Transposition Impacted or embedded teeth with abnormal position of such teeth or adjacent teeth K07.4 Malocclusion, unspecified K07.5 Dentofacial functional abnormalities Abnormal jaw closure Malocclusion due to: • abnormal swallowing • mouth breathing • tongue, lip or finger habits K07.6 Temporomandibular joint disorders Costen's complex or syndrome Derangement of temporomandibular joint Snapping jaw Temporomandibular joint-pain-dysfunction syndrome Excludes: current temporomandibular joint: • dislocation (S03.0) • strain (S03.4) K07.8 Other dentofacial anomalies K07.9 Dentofacial anomaly, unspecified 1m Stomatitis and related lesions K12.0 Recurrent oral aphthae Aphthous stomatitis (major)(minor) Bednar's aphthae Periadenitis mucosa necrotica recurrens Recurrent aphthous ulcer Stomatitis herpetiformis 290 DISEASES OF THE DIGESTIVE SYSTEM Diseases of oesophagus, stomach and duodenum (K20-K31) Ill Oesophagitis Abscess of oesophagus Oesophagitis: • NOS • chemical • peptic Use additional external cause code (Chapter XX), if desired, to identify cause. -

INVESTIGATION and TREATMENT of VAGINAL DISCHARGE and PRURITUS VULVAE L Chan
INVITED ARTICLE I INVESTIGATION AND TREATMENT OF VAGINAL DISCHARGE AND PRURITUS VULVAE L Chan ABSTRACT The causes of vaginal discharge for pruritus vulvae in a patient are considered in three categories: common causes like vaginal candidosis, Trichomonal vaginitis, Gardnerella vaginitis; less common causes like gonococ- cal infection, Chlamydia infection and T-mycoplasma infection; and uncommon causes which include allergy to nylon underwear, human papilloma infection and eczema. The clinical features of each and a suggested treatment regime are given. Keywords: Vaginal discharge, Pruritus vulvae. SING MED J. 1989; NO 30: 471 - 472 INTRODUCTION atedly. Vaginal examination usually reveals white curdy discharge. Microscopy will show fungal spores or Vaginal discharge and pruritus vulvae are common hyphae. Treatment of the infection is with a course of symptoms that patients present with when they visit a antifungal vaginal tablets, e.g. Tioconazole (Gyno- gynaecologist. These symptoms suggest vaginal infec- Trosyd) 100 mgm o.n. for 3 nights. Anti -fungal cream tion, but as with all clinical problems, the diagnosis be given if there is pruritus vulvae. Oral Ketoconazole rests on a careful history, a thorough clinical examina- (Nizoral) one b.d. can be given for 5 days if there is tion and appropriate investigations. recurrent vaginal candidosis. Persistent chronic candi - The patient can complain of vaginal discharge, dosis. ìs due to lowered resistance to fungal infection. pruritus vulvae or both of these symptoms. Firstly, one Occasionally, the husband harbours a candida infection must determine whether the complaint is made so that between the prepuce and the glans penis and this the patient can legitimise seeing the doctor for the real infection needs -to be eradicated.