Care of the Patient with Acute Ischemic Stroke
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Research Brief March 2017 Publication #2017-16
Research Brief March 2017 Publication #2017-16 Flourishing From the Start: What Is It and How Can It Be Measured? Kristin Anderson Moore, PhD, Child Trends Christina D. Bethell, PhD, The Child and Adolescent Health Measurement Introduction Initiative, Johns Hopkins Bloomberg School of Every parent wants their child to flourish, and every community wants its Public Health children to thrive. It is not sufficient for children to avoid negative outcomes. Rather, from their earliest years, we should foster positive outcomes for David Murphey, PhD, children. Substantial evidence indicates that early investments to foster positive child development can reap large and lasting gains.1 But in order to Child Trends implement and sustain policies and programs that help children flourish, we need to accurately define, measure, and then monitor, “flourishing.”a Miranda Carver Martin, BA, Child Trends By comparing the available child development research literature with the data currently being collected by health researchers and other practitioners, Martha Beltz, BA, we have identified important gaps in our definition of flourishing.2 In formerly of Child Trends particular, the field lacks a set of brief, robust, and culturally sensitive measures of “thriving” constructs critical for young children.3 This is also true for measures of the promotive and protective factors that contribute to thriving. Even when measures do exist, there are serious concerns regarding their validity and utility. We instead recommend these high-priority measures of flourishing -
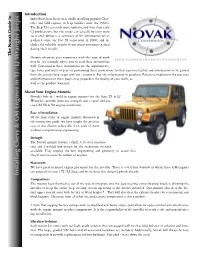
Installing Chevy & GM Engines in TJ / LJ W Rangler
Introduction Individuals have been successfully installing popular Chev- rolet and GM engines to Jeep vehicles since the 1960’s. The Jeep TJ is certainly more sophisticated than their early CJ predecessors, but the swaps can actually be even more successful. Below is a summary of the information we’ve gathered since our first TJ conversion in 2000, and in- cludes the valuable insight of our many customers gained during their installs. The Novak Guide to Despite whatever your experience with this type of work may be, we strongly advise you to read these instructions well. Contained in these instructions are the requirements, tips, hints and tricks of years of performing these conversions, both in our own facility and information we’ve gained from discussing these swaps with our customers. Put this information to good use. Failure to implement the practices and information in these pages may jeopardize the quality of your work, as well as the product warranty. About Your Engine Mounts Novak’s bolt-in / weld-in engine mounts for the Jeep TJ & LJ Wranglers provide immense strength and a rapid and pre- cise GM V6 & V8 engine installation. Ease of Installation Of the four styles of engine mounts discussed in this instruction guide, we have sought the greatest ease of installation achievable with each of them without compromising engineering. Strength The Novak mounts feature a thick 3/16 steel construc- tion and a welded box design for the maximum strength available. They employ the best engineering and geometry to assure that they’ll survive even the wildest of engines. -

The Origin of the Peculiarities of the Vietnamese Alphabet André-Georges Haudricourt
The origin of the peculiarities of the Vietnamese alphabet André-Georges Haudricourt To cite this version: André-Georges Haudricourt. The origin of the peculiarities of the Vietnamese alphabet. Mon-Khmer Studies, 2010, 39, pp.89-104. halshs-00918824v2 HAL Id: halshs-00918824 https://halshs.archives-ouvertes.fr/halshs-00918824v2 Submitted on 17 Dec 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Published in Mon-Khmer Studies 39. 89–104 (2010). The origin of the peculiarities of the Vietnamese alphabet by André-Georges Haudricourt Translated by Alexis Michaud, LACITO-CNRS, France Originally published as: L’origine des particularités de l’alphabet vietnamien, Dân Việt Nam 3:61-68, 1949. Translator’s foreword André-Georges Haudricourt’s contribution to Southeast Asian studies is internationally acknowledged, witness the Haudricourt Festschrift (Suriya, Thomas and Suwilai 1985). However, many of Haudricourt’s works are not yet available to the English-reading public. A volume of the most important papers by André-Georges Haudricourt, translated by an international team of specialists, is currently in preparation. Its aim is to share with the English- speaking academic community Haudricourt’s seminal publications, many of which address issues in Southeast Asian languages, linguistics and social anthropology. -

On Kernels, Β-Graphs, and Β-Graph Sequences of Digraphs Kevin D
On Kernels, b-graphs, and b-graph Sequences of Digraphs By Kevin D. Adams Submitted to the Department of Mathematics and the Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Master of Arts Margaret Bayer, Chairperson Committee members Jeremy Martin Yunfeng Jiang Date defended: 5-1-2015 The Master’s Thesis Committee for Kevin D. Adams certifies that this is the approved version of the following master’s thesis : On Kernels, b-graphs, and b-graph Sequences of Digraphs Margaret Bayer, Chairperson Date approved: 5-1-2015 ii Abstract We begin by investigating some conditions determining the existence of kernels in various classes of directed graphs, most notably in oriented trees, grid graphs, and oriented cycles. The question of uniqueness of these kernels is also handled. Attention is then shifted to g-graphs, structures associated to the minimum dominating sets of undirected graphs. I define the b-graph of a given digraph analogously, involving the minimum absorbant sets. Finally, attention is given to iterative construction of b- graphs, with an attempt to characterize for what classes of digraphs these b-sequences terminate. iii Acknowledgements I would like to thank my advisor Professor Marge Bayer for her patience and guid- ance, as well as my committee members Professors Jeremy Martin and Yunfeng Jiang for teaching me some very interesting algebra and combinatorics. Thanks to all of the professors from whom I’ve learned so very much during my time at KU. Thank you to my lovely fiancée Elise for her constant support and encouragement, even across long distances. -
Applications the Formula Y = Mx + B Sometimes Appears with Different
PRIMARY CONTENT MODULE Algebra I -Linear Equations & Inequalities T-71 Applications The formula y = mx + b sometimes appears with different symbols. For example, instead of x, we could use the letter C. Instead of y, we could use the letter F. Then the equation becomes F = mC + b. All temperature scales are related by linear equations. For example, the temperature in degrees Fahrenheit is a linear function of degrees Celsius. © 1999, CISC: Curriculum and Instruction Steering Committee The WINNING EQUATION PRIMARY CONTENT MODULE Algebra I -Linear Equations & Inequalities T-72 Basic Temperature Facts Water freezes at: 0°C, 32°F Water Boils at: 100°C, 212°F F • (100, 212) • (0, 32) C Can you solve for m and b in F = mC + b? © 1999, CISC: Curriculum and Instruction Steering Committee The WINNING EQUATION PRIMARY CONTENT MODULE Algebra I -Linear Equations & Inequalities T-73 To find the equation relating Fahrenheit to Celsius we need m and b F – F m = 2 1 C2 – C1 212 – 32 m = 100 – 0 180 9 m = = 100 5 9 Therefore F = C + b 5 To find b, substitute the coordinates of either point. 9 32 = (0) + b 5 Therefore b = 32 Therefore the equation is 9 F = C + 32 5 Can you solve for C in terms of F? © 1999, CISC: Curriculum and Instruction Steering Committee The WINNING EQUATION PRIMARY CONTENT MODULE Algebra I -Linear Equations & Inequalities T-74 Celsius in terms of Fahrenheit 9 F = C + 32 5 5 5 9 F = æ C +32ö 9 9è 5 ø 5 5 F = C + (32) 9 9 5 5 F – (32) = C 9 9 5 5 C = F – (32) 9 9 5 C = (F – 32) 9 Example: How many degrees Celsius is77°F? 5 C = (77 – 32) 9 5 C = (45) 9 C = 25° So 72°F = 25°C © 1999, CISC: Curriculum and Instruction Steering Committee The WINNING EQUATION PRIMARY CONTENT MODULE Algebra I -Linear Equations & Inequalities T-75 Standard 8 Algebra I, Grade 8 Standards Students understand the concept of parallel and perpendicular lines and how their slopes are related. -

Form Y-203-I, If You Had More Than One Job, Or If You Had a Job for Only Part of the Year
Department of Taxation and Finance Yonkers Nonresident Earnings Tax Return Y-203 For the full year January 1, 2020, through December 31, 2020, or fiscal year beginning and ending Name as shown on Form IT-201 or IT-203 Social Security number A Were you a Yonkers resident for any part of the taxable year? (mark an X in the appropriate box) Yes No (see instructions) (See the instructions for Form IT-201 or IT-203 for the definition of a resident.) If Yes: 1. Give period of Yonkers residence. From (mmddyyyy) to (mmddyyyy) 2. Are you reporting Yonkers resident income tax surcharge on your New York State return? ..................................................................................... Yes No (submit explanation) 3. You must complete and submit Form IT-360.1 (see instructions). B Did you or your spouse maintain an apartment or other living quarters in Yonkers during any part of the year?...................................................................................... Yes No If Yes, give address below and enter the number of days spent in Yonkers during 2020: days Address: C Are you reporting income from self-employment (on line 2 below)?......... Yes No If Yes, complete the following: Business name Business address Employer identification number Principal business activity Form of business: Sole proprietorship Partnership Other (explain) Calculation of nonresident earnings tax 1 Gross wages and other employee compensation (see instructions; if claiming an allocation, include amount from line 22) ............................................... 1 .00 2 Net earnings from self-employment (see instructions; if claiming an allocation, include amount from line 32; if a loss, write loss on line 2) ............................................................................................... 2 .00 3 Add lines 1 and 2 (if line 2 is a loss, enter amount from line 1) ........................................................... -

Ffontiau Cymraeg
This publication is available in other languages and formats on request. Mae'r cyhoeddiad hwn ar gael mewn ieithoedd a fformatau eraill ar gais. [email protected] www.caerphilly.gov.uk/equalities How to type Accented Characters This guidance document has been produced to provide practical help when typing letters or circulars, or when designing posters or flyers so that getting accents on various letters when typing is made easier. The guide should be used alongside the Council’s Guidance on Equalities in Designing and Printing. Please note this is for PCs only and will not work on Macs. Firstly, on your keyboard make sure the Num Lock is switched on, or the codes shown in this document won’t work (this button is found above the numeric keypad on the right of your keyboard). By pressing the ALT key (to the left of the space bar), holding it down and then entering a certain sequence of numbers on the numeric keypad, it's very easy to get almost any accented character you want. For example, to get the letter “ô”, press and hold the ALT key, type in the code 0 2 4 4, then release the ALT key. The number sequences shown from page 3 onwards work in most fonts in order to get an accent over “a, e, i, o, u”, the vowels in the English alphabet. In other languages, for example in French, the letter "c" can be accented and in Spanish, "n" can be accented too. Many other languages have accents on consonants as well as vowels. -

(3) (Y'(Uf)\L + 2A(U)B(Y(U))\\O
proceedings of the american mathematical society Volume 34, Number 1, July 1972 PROPERTIES OF SOLUTIONS OF DIFFERENTIAL EQUATIONS OF THE FORM / 4- a(t)b(y) = 0 ALLAN KROOPNICK Abstract. Two theorems are presented which guarantee the boundedness and oscillation of solutions of certain classes of second order nonlinear differential equations. In this paper we shall show boundedness of solutions of the differential equation y"+a(t)b(y)=0 with appropriate conditions on a(t) and b(y). Furthermore, all solutions will be oscillatory subject to a further condition. By oscillatory we shall mean a function having arbitrarily large zeros. The first theorem is an extension of a result of Utz [1] in which he con- siders b(y)=y2n~1. We now prove a result for boundedness of solutions. Theorem I. If a(t)> a>0 and da/dt^O on [T, oo), b(y) continuous, and limj,^±00B(y)=$yb(u) du=co then all solutions of (1) / + a(t)b(y)=0 are bounded as r—>-oo. Proof. Multiply (1) by 2/ to get (2) 2y'y" + 2a(t)b(y)y' = 0. Upon integration by parts we have (3) (y'(uf)\l+ 2a(u)B(y(u))\\o- 2 P df B(y)du = 0. J ir, Uli Thus (4) y'(tf + 2a(t)B(y(t))- 2 f ^ B(y)du = K Jto du where K=y'(t0)2-r-2a(to)B(y(to)). Now the above implies \y'\ and \y\ remain bounded. If not, the left side of (4) would become infinite which is impossible. -
У^C/ ^Xaxxlty^Yy Yyy- Y/A М /A XX
1 5 2 Va X A y // /^ //X A ^ M a i Y'YY/ ’^y y y -ì - A Y & y n / X X - y7 AAl/XX /AlAX AA /X y ^z^s -i o y ^ y y H ^ - z ^ A c ^ J Ì^Ystn^XUY Y LY X ’YYi yl^-CY7 A/ y A A Y ^ t V Y f AC-, C x ix x r~/Y- CYtS Vy* X{ l à / ¿ Y l ^ l Y A". A X r u / , A / C A ut Y A l' T O tl / V l X ^ ì y y Z A ^/Aa ^ A y y A c y ^ yl A A t d l f H ^ c ò / a AtA r t / ^ ¿ ù a / z Cy/ X X-CAX? yCA %-O > yCCfl/Cj t L ^ H ' Ì ^ ì y AC A & A / c i Cy y ^ ehf yZy y y Y- ACC y i C C A A ^ tiY 'l'VZY-YcZo 'SA y y - Z-eY^Y A iaA a ^ C c' A^ . 7 ' Y ^ C / / ¿ H y/yi-C-td A#A y -AA Yy y y A 'iCA uX ZY lls X^^y y y y y y y A y '* 1 Xt i 'l-tA Y V Y l' '/A A in - r iY -t^Y d X y v A y y > y Y Y Y y CitYYyACAty C/ y y y 'lA 'V ¿A,A a 4 aC y y A i Y Y y 'Y> '-/AYYA •■*yv/ ’a a a i a U ^ t & l i - AA-Y>t/ACy-7A ^ < / A - '" 'X X X 'X t X d'PY'. -

1. First Examples a Differential Equation for a Variable U(X, Y, . . .)
1. First examples A differential equation for a variable u(x; y; : : : ), which depends on the independent variables x, y, . , is an equation which involves u and some of its partial derivatives. Differential equations have traditionally played a huge role in the sciences and so they have been heavily studied in mathematics. If u depends on x and y, there are two partial derivatives, @u @u and : @x @y Since partial differential equations might involve lots of variables and derivatives, it is convenient to introduce some more compact notation. @u @u = u and = u : @x x @y y Note that @2u @2u @2u u = u = and u = : xx @x2 xy @x@y yy @y2 Recall some basic facts about derivatives. First of all derivatives are local, meaning if you only change the function away from a point then the derivative is unchanged (contrast this with the integral, which is far from local; the area under the graph depends on the global behaviour). Secondly if all 2nd derivatives exist and they are continuous then the mixed partials are equal: uxy = uyx: Example 1.1. Suppose that u(x; y) = sin(xy): Then ux = y cos(xy) and uy = x cos(xy): But then uyx = cos(xy) − xy sin(xy) and uxy = cos(xy) − xy sin(xy): Partial differential equations are in general very complicated and normally we can only make sense of the solutions of those equations which come from applications. If there are two space variables then we typically call them x and y but as usual t denotes a time variable and x a space variable. -

Acquisition of L2 Phonology – Spanish Meets Croatian
ACQUISITION OF L2 PHONOLOGY – SPANISH MEETS CROATIAN Maša Musulin University of Zagreb Article History: Submitted: 10.06.2015 Accepted: 08.08.2015 Abstract: The phoneme is conceived as a mental image that is stored in our mind and then represented by sounds in speech and graphemes in writing for phonologically based alphabets. The acquisition of L2 phonology includes two very important skills – reading and writing. The information stored in the mind of a speaker interferes with new information produced by the L2 (Robinson, Ellis 2008; Nathan, 2008). What is similar or equal in the target language to one's native language is, while unknown, incorporated one way or another into an existing model, based on prototypicality (Pompeian, 2004, Moreno Fernández, 2010). The process of teaching the sounds, letters and alphabet to foreign students is much shorter than for native speakers because to a foreign student must be given a tool for writing as soon as possible as they have to write what they are learning and memorize new language units (Celce-Murcia, Brinton, Goodwin, 1996). This paper discusses one type of difficulties Spanish learners of Croatian as L2 face when they are introduced to phonology through letters which represent Croatian sounds in order to display the influence of their preexisting phonological concepts. The subjects are ten students from Spain and Latin America. Their task was to read a group of words containing sounds that were predictably hard for them, minimal pairs and a short text. Keywords: phoneme, grapheme, letter, phonological awareness, foreign language 1. INTRODUCTION As literacy has a big impact on phonological awareness in languages with phonological writing, the graphemes that represent the phonemes, including letters, make an integral part of their mental image. -

Nastaleeq: a Challenge Accepted by Omega
Nastaleeq: A challenge accepted by Omega Atif Gulzar, Shafiq ur Rahman Center for Research in Urdu Language Processing, National University of Computer and Emerging Sciences, Lahore, Pakistan atif dot gulzar (at) gmail dot com, shafiq dot rahman (at) nu dot edu dot pk Abstract Urdu is the lingua franca as well as the national language of Pakistan. It is based on Arabic script, and Nastaleeq is its default writing style. The complexity of Nastaleeq makes it one of the world's most challenging writing styles. Nastaleeq has a strong contextual dependency. It is a cursive writing style and is written diagonally from right to left. The overlapping shapes make the nuqta (dots) and kerning problem even harder. With the advent of multilingual support in computer systems, different solu- tions have been proposed and implemented. But most of these are immature or platform-specific. This paper discuses the complexity of Nastaleeq and a solution that uses Omega as the typesetting engine for rendering Nastaleeq. 1 Introduction 1.1 Complexity of the Nastaleeq writing Urdu is the lingua franca as well as the national style language of Pakistan. It has more than 60 mil- The Nastaleeq writing style is far more complex lion speakers in over 20 countries [1]. Urdu writing than other writing styles of Arabic script{based lan- style is derived from Arabic script. Arabic script has guages. The salient features`r of Nastaleeq that many writing styles including Naskh, Sulus, Riqah make it more complex are these: and Deevani, as shown in figure 1. Urdu may be • Nastaleeq is a cursive writing style, like other written in any of these styles, however, Nastaleeq Arabic styles, but it is written diagonally from is the default writing style of Urdu.