API Textbook of Medicine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cons 103020 Sf.Pdf
OUTSTANDING AMOUNT IN ASSET DATE OF DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR PAN_DIR1 DIN FOR DIRECTOR SRNO PARTY CREDIT GRANTOR STATE CREDIT GRANTOR BRANCH REGISTERED ADDRESS SUIT OTHER BANK DIRECTOR 1 PAN_DIR1 DIN FOR DIRECTOR 1 DIRECTOR 2 PAN_DIR2 DIRECTOR 3 PAN_DIR3 DIRECTOR 4 PAN_DIR4 DIRECTOR 5 PAN_DIR5 DIRECTOR 6 PAN_DIR6 DIN FOR DIRECTOR 6 DIRECTOR 7 PAN_DIR7 DIRECTOR 8 PAN_DIR8 DIN FOR DIRECTOR 8 DIRECTOR 9 PAN_DIR9 DIRECTOR 10 PAN_DIR10 DIRECTOR 11 PAN_DIR11 DIRECTOR 12 PAN_DIR12 DIRECTOR 13 DIRECTOR 14 PAN_DIR14 DIRECTOR 15 DIRECTOR 16 DIRECTOR 17 DIRECTOR 18 DIRECTOR 19 DIRECTOR 20 LACS CLASSIFICATION CLASSIFICATION 2 3 4 5 7 9 10 11 12 3 13 14 5 15 6 16 7 17 8 18 9 19 1 Datar Switchgears Ltd. HDFC BANK LTD Maharashtra Nasik Datar Commpercial Complex, Vakil Wadi, Nasik 422 001. 1086 Loss Assets 31.08.2001 Suit Rajan Datar Shobhana Datar Sophi, 18 New Kanta Wadi Road, Off.Perry Cross Road, Bandra, 2 East West Travels & Trade Links HDFC BANK LTD Maharashtra Mumbai 194 Loss Assets 31.03.2001 Suit Thakiyudeen Wahid Naserudhin Wahid Mumbai - 400 050. 604/65, Keshava Building, Bandra Kurla Complex, Bandra (East), 3 Kedia Distilleries Ltd. HDFC BANK LTD Maharashtra Mumbai 309 Loss Assets 30.04.1998 Suit K.P. Kedia Vinay Kedia P.K. Deora T.C. -

Acrs Je 2014
LIST OF ACRS OF JUNIOR ENGINERS (CIVIL) UP to 31.03.2014 S.No Name Designation D.O.B D.O.A Period 1 Pana Lal J.E 22.11.66 11.05.87 11.05.87 to31.03.2009 2 Paran Chand J.E 03.03.57 20.07.78 20.07.78 to 2008 3 Duni Chand J.E 04.01.56 24.07.78 24.07.78 & 01.08.03 to 31.03.10 4 Monaj kumar J.E 08.05.69 18.03.96 01.04.97 to 31.05.99 &01.04.04 to 31.03.112 5 Rajneesh Bansal J.E 04.10.67 23.01.95 23.01.95 to 31.03.2008 6 Paresh Chaun\han J.E 16.06.67 28.02.2004 01.03.2004 to 31.03.2012 7 Anil pathik J.E 03.05.65 28.02.04 01.04.2004 to 31.03.2012 8 Rajender Singh J.E 11.02.68 17.11.97 01.04.98 to 31.03.2009 Bagga 9 Rattan Chand J.E 22.08.60 01.04.85 01.04.85 to 31.03.98 10 Navneet Gupta J.E 03.04.72 12.08.97 12.08.97 to 31.03.2002 & 1.04.2006 yo 31.03.13 11 Mohan Rajeev J.E 23.07.63 24.01.85 01.04.85 to31.03.2004 12 Ravinder Kumar J.E 05.05.62 29.09.86 29.09.86 to 31.03.2013 13 Rajesh Kumar J.E 23.10.58 02.02.77 01.04.91 to31.03.210 14 Anil Kumar J.E 20.12.62 06.03.86 06.03.86 to31.03.2001 &01.04.2006 to31.03.2010 15 Skinder Singh J.E 03.03.68 19.07.93 19.07.93 to31.03.2010 16 Partap Singh J.E 02.01.60 08.12.86 01.04.2009 to 31.03.2012 17 18 Kishor Kumar J.E 04.07.67 10.01.97 01.04.99 to31.03.2012 19 Jagdish Chand J.E 28.01.62 16.02.96 01.04.08 to3 1.03.12 20 Anil Kumar J.E 06.06.66 14.06.91 01.04.08 to 31.03.12 21 Ashok Kumar J.E 18.04.69 13.11.2009 01.04.2010 to 31.03.2012 22 Pardeep Kumar J.E 06.03.62 01.01.97 01.01.97 to 31.03.12 Sharma 23 Pardeep kumar J.E 13.01.69 30.12.2005 01.04.2007 to 31.03.12 24 Ravinder Pal J.E 28.01.65 02.01.87 01.07.90 -
MGT-7 Submission
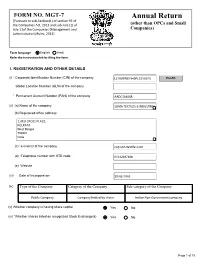
FORM NO. MGT-7 Annual Return [Pursuant to sub-Section(1) of section 92 of the Companies Act, 2013 and sub-rule (1) of (other than OPCs and Small rule 11of the Companies (Management and Companies) Administration) Rules, 2014] Form language English Hindi Refer the instruction kit for filing the form. I. REGISTRATION AND OTHER DETAILS (i) * Corporate Identification Number (CIN) of the company L51909WB1940PLC010070 Pre-fill Global Location Number (GLN) of the company * Permanent Account Number (PAN) of the company AADCS0405R (ii) (a) Name of the company SOMA TEXTILES & INDUSTRIES (b) Registered office address 2, RED CROSS PLACE, KOLKATA West Bengal 700001 India (c) *e-mail ID of the company [email protected] (d) *Telephone number with STD code 03322487406 (e) Website (iii) Date of Incorporation 29/03/1940 (iv) Type of the Company Category of the Company Sub-category of the Company Public Company Company limited by shares Indian Non-Government company (v) Whether company is having share capital Yes No (vi) *Whether shares listed on recognized Stock Exchange(s) Yes No Page 1 of 15 (a) Details of stock exchanges where shares are listed S. No. Stock Exchange Name Code 1 BSE LIMITED 1 2 National Stock Exchange of India 1,024 (b) CIN of the Registrar and Transfer Agent U67190MH1999PTC118368 Pre-fill Name of the Registrar and Transfer Agent LINK INTIME INDIA PRIVATE LIMITED Registered office address of the Registrar and Transfer Agents C-101, 1st Floor, 247 Park, Lal Bahadur Shastri Marg, Vikhroli (West) (vii) *Financial year From date 01/04/2020 (DD/MM/YYYY) To date 31/03/2021 (DD/MM/YYYY) (viii) *Whether Annual general meeting (AGM) held Yes No (a) If yes, date of AGM (b) Due date of AGM 30/09/2021 (c) Whether any extension for AGM granted Yes No II. -

53Rd AIIMS ANNUAL REPORT 2008–2009
53rd AIIMS ANNUAL REPORT 2008–2009 All India Institute of Medical Sciences New Delhi 110029 Edited jointly by: Dr Sunil Chumber, Additional Professor, Department of Surgical Disciplines and Sub-Dean (Academic) Dr Tanuj Dada, Associate Professor, Dr R.P. Centre for Ophthalmic Sciences Dr Venkata Karthikeyan C, Assistant Professor, Department of Otorhinolaryngology (ENT) Dr S.K. Maulik, Professor, Department of Pharmacology Dr Raj D. Mehra, Professor, Department of Anatomy Dr Kameshwar Prasad, Professor, Department of Neurology Dr S. Rastogi, Professor, Department of Orthopaedics Dr Sushma Sagar, Assistant Professor, JPNA Trauma Centre Dr Peush Sahni, Professor, Department of Gastrointestinal Surgery Dr Pratap Sharan, Professor, Department of Psychiatry Dr D.N. Sharma, Assistant Professor, Dr BRA, Institute Rotary Cancer Hospital Dr Subrata Sinha, Professor and Head, Department of Biochemistry Dr Sanjay Kumar Sood, Assistant Professor, Department of Physiology Dr Sachin Talwar, Assistant Professor, Department of C.T.V.S. February 2010 Printed at Saurabh Printers Pvt. Ltd., A-16, Sector-IV, NOIDA (U.P.) All India Institute of Medical Sciences The All India Institute of Medical Sciences (AIIMS) was established in 1956 as an institution of national importance by an Act of Parliament with the objects to develop patterns of teaching in undergraduate and postgraduate medical education in all its branches so as to demonstrate a high standard of medical education to all medical colleges and other allied institutions in India; to bring together in one place educational facilities of the highest order for the training of personnel in all important branches of health activity and to attain self-sufficiency in postgraduate medical education. -
(Public Section) Padma Awards Directory (1954-2009) Year-Wise List Sl
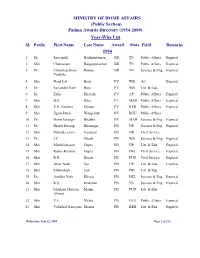
MINISTRY OF HOME AFFAIRS (Public Section) Padma Awards Directory (1954-2009) Year-Wise List Sl. Prefix First Name Last Name Award State Field Remarks 1954 1 Dr. Sarvapalli Radhakrishnan BR TN Public Affairs Expired 2 Shri Chakravarti Rajagopalachari BR TN Public Affairs Expired 3 Dr. Chandrasekhara Raman BR TN Science & Eng. Expired Venkata 4 Shri Nand Lal Bose PV WB Art Expired 5 Dr. Satyendra Nath Bose PV WB Litt. & Edu. 6 Dr. Zakir Hussain PV AP Public Affairs Expired 7 Shri B.G. Kher PV MAH Public Affairs Expired 8 Shri V.K. Krishna Menon PV KER Public Affairs Expired 9 Shri Jigme Dorji Wangchuk PV BHU Public Affairs 10 Dr. Homi Jehangir Bhabha PB MAH Science & Eng. Expired 11 Dr. Shanti Swarup Bhatnagar PB UP Science & Eng. Expired 12 Shri Mahadeva Iyer Ganapati PB OR Civil Service 13 Dr. J.C. Ghosh PB WB Science & Eng. Expired 14 Shri Maithilisharan Gupta PB UP Litt. & Edu. Expired 15 Shri Radha Krishan Gupta PB DEL Civil Service Expired 16 Shri R.R. Handa PB PUN Civil Service Expired 17 Shri Amar Nath Jha PB UP Litt. & Edu. Expired 18 Shri Malihabadi Josh PB DEL Litt. & Edu. 19 Dr. Ajudhia Nath Khosla PB DEL Science & Eng. Expired 20 Shri K.S. Krishnan PB TN Science & Eng. Expired 21 Shri Moulana Hussain Madni PB PUN Litt. & Edu. Ahmed 22 Shri V.L. Mehta PB GUJ Public Affairs Expired 23 Shri Vallathol Narayana Menon PB KER Litt. & Edu. Expired Wednesday, July 22, 2009 Page 1 of 133 Sl. Prefix First Name Last Name Award State Field Remarks 24 Dr. -
Padma Vibhushan S. No. Name of the Awardee Discipline State/Domicile
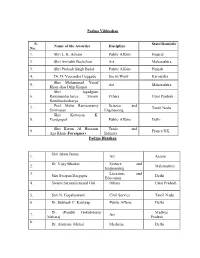
Padma Vibhushan S. State/Domicile Name of the Awardee Discipline No. 1. Shri L. K. Advani Public Affairs Gujarat 2. Shri Amitabh Bachchan Art Maharashtra 3. Shri Prakash Singh Badal Public Affairs Punjab 4. Dr. D. Veerendra Heggade Social Work Karnataka Shri Mohammad Yusuf 5. Art Maharashtra Khan alias Dilip Kumar Shri Jagadguru 6. Ramanandacharya Swami Others Uttar Pradesh Rambhadracharya Prof. Malur Ramaswamy Science and 7. Tamil Nadu Srinivasan Engineering Shri Kottayan K. 8. Venugopal Public Affairs Delhi Shri Karim Al Hussaini Trade and 9. France/UK Aga Khan ( Foreigner) Industry Padma Bhushan Shri Jahnu Barua 1. Art Assam Dr. Vijay Bhatkar Science and 2. Maharashtra Engineering 3. Literature and Shri Swapan Dasgupta Delhi Education 4. Swami Satyamitranand Giri Others Uttar Pradesh 5. Shri N. Gopalaswami Civil Service Tamil Nadu 6. Dr. Subhash C. Kashyap Public Affairs Delhi Dr. (Pandit) Gokulotsavji Madhya 7. Art Maharaj Pradesh 8. Dr. Ambrish Mithal Medicine Delhi 9. Smt. Sudha Ragunathan Art Tamil Nadu 10. Shri Harish Salve Public Affairs Delhi 11. Dr. Ashok Seth Medicine Delhi 12. Literature and Shri Rajat Sharma Delhi Education 13. Shri Satpal Sports Delhi 14. Shri Shivakumara Swami Others Karnataka Science and 15. Dr. Kharag Singh Valdiya Karnataka Engineering Prof. Manjul Bhargava Science and 16. USA (NRI/PIO) Engineering 17. Shri David Frawley Others USA (Vamadeva) (Foreigner) 18. Shri Bill Gates Social Work USA (Foreigner) 19. Ms. Melinda Gates Social Work USA (Foreigner) 20. Shri Saichiro Misumi Others Japan (Foreigner) Padma Shri 1. Dr. Manjula Anagani Medicine Telangana Science and 2. Shri S. Arunan Karnataka Engineering 3. Ms. Kanyakumari Avasarala Art Tamil Nadu Literature and Jammu and 4. -
IFL Annual Return 2018-19
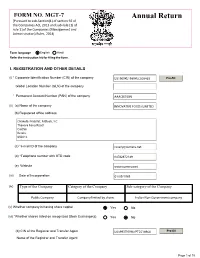
FORM NO. MGT-7 Annual Return [Pursuant to sub-Section(1) of section 92 of the Companies Act, 2013 and sub-rule (1) of rule 11of the Companies (Management and Administration) Rules, 2014] Form language English Hindi Refer the instruction kit for filing the form. I. REGISTRATION AND OTHER DETAILS (i) * Corporate Identification Number (CIN) of the company Pre-fill Global Location Number (GLN) of the company * Permanent Account Number (PAN) of the company (ii) (a) Name of the company (b) Registered office address (c) *e-mail ID of the company (d) *Telephone number with STD code (e) Website (iii) Date of Incorporation (iv) Type of the Company Category of the Company Sub-category of the Company (v) Whether company is having share capital Yes No (vi) *Whether shares listed on recognized Stock Exchange(s) Yes No (b) CIN of the Registrar and Transfer Agent Pre-fill Name of the Registrar and Transfer Agent Page 1 of 15 Registered office address of the Registrar and Transfer Agents (vii) *Financial year From date 01/04/2018 (DD/MM/YYYY) To date 31/03/2019 (DD/MM/YYYY) (viii) *Whether Annual general meeting (AGM) held Yes No (a) If yes, date of AGM 24/09/2019 (b) Due date of AGM 30/09/2019 (c) Whether any extension for AGM granted Yes No II. PRINCIPAL BUSINESS ACTIVITIES OF THE COMPANY *Number of business activities 1 S.No Main Description of Main Activity group Business Description of Business Activity % of turnover Activity Activity of the group code Code company I I2 III. PARTICULARS OF HOLDING, SUBSIDIARY AND ASSOCIATE COMPANIES (INCLUDING JOINT VENTURES) *No. -

Activity Report 2009 – 2010
Activity Report 2009 – 2010 L V Prasad Eye Institute Kallam Anji Reddy Campus L V Prasad Marg, Banjara Hills Hyderabad 500 034, India Tel: 91 40 3061 2345 Fax: 91 40 2354 8271 e-mail: [email protected] L V Prasad Eye Institute Patia, Bhubaneswar 751 024 Orissa, India Tel: 91 0674 3989 2020 Fax: 91 0674 3987 130 e-mail: [email protected] L V Prasad Eye Institute G M R Varalakshmi Campus Door No: 11-113/1 Hanumanthawaka Junction Visakhapatnam 530 040 Andhra Pradesh, India Tel: 91 0891 3989 2020 Fax: 91 0891 398 4444 L V Prasad Eye Institute e-mail: [email protected] Excellence • Equity • Effi ciency Art with vision, for vision Artist-in-residence Sisir Sahana in his workshop on A view of the Art Gallery on Level 6 at Hyderabad LVPEI’s Kallam Anji Reddy campus, Hyderabad creating campus, where several works by Mr Surya Prakash, one of his signature glass sculptures. Inset: A piece from our senior artist-in-residence are on display. his latest collection, entitled “The long climb”. Inset: The hand that wields the paintbrush! L V Prasad Eye Institute Committed to excellence and equity in eye care Activity Report April 2009 – March 2010 Collaborating Centre for Prevention of Blindness L V Prasad Eye Institute, a not-for-profi t charitable organization, is governed by two trusts: Hyderabad Eye Institute and Hyderabad Eye Research Foundation. Donations to Hyderabad Eye Research Foundation are 175% exempt under section 35 (i) (ii) and donations made to Hyderabad Eye Institute are 50% exempt under section 80G of the Income Tax Act. -

Dear Aspirant with Regard
DEAR ASPIRANT HERE WE ARE PRESENTING YOU A GENRAL AWERNESS MEGA CAPSULE FOR IBPS PO, SBI ASSOT PO , IBPS ASST AND OTHER FORTHCOMING EXAMS WE HAVE UNDERTAKEN ALL THE POSSIBLE CARE TO MAKE IT ERROR FREE SPECIAL THANKS TO THOSE WHO HAS PUT THEIR TIME TO MAKE THIS HAPPEN A IN ON LIMITED RESOURCE 1. NILOFAR 2. SWETA KHARE 3. ANKITA 4. PALLAVI BONIA 5. AMAR DAS 6. SARATH ANNAMETI 7. MAYANK BANSAL WITH REGARD PANKAJ KUMAR ( Glory At Anycost ) WE WISH YOU A BEST OF LUCK CONTENTS 1 CURRENT RATES 1 2 IMPORTANT DAYS 3 CUPS & TROPHIES 4 4 LIST OF WORLD COUNTRIES & THEIR CAPITAL 5 5 IMPORTANT CURRENCIES 9 6 ABBREVIATIONS IN NEWS 7 LISTS OF NEW UNION COUNCIL OF MINISTERS & PORTFOLIOS 13 8 NEW APPOINTMENTS 13 9 BANK PUNCHLINES 15 10 IMPORTANT POINTS OF UNION BUDGET 2012-14 16 11 BANKING TERMS 19 12 AWARDS 35 13 IMPORTANT BANKING ABBREVIATIONS 42 14 IMPORTANT BANKING TERMINOLOGY 50 15 HIGHLIGHTS OF UNION BUDGET 2014 55 16 FDI LLIMITS 56 17 INDIAS GDP FORCASTS 57 18 INDIAN RANKING IN DIFFERENT INDEXS 57 19 ABOUT : NABARD 58 20 IMPORTANT COMMITTEES IN NEWS 58 21 OSCAR AWARD 2014 59 22 STATES, CAPITAL, GOVERNERS & CHIEF MINISTERS 62 23 IMPORTANT COMMITTEES IN NEWS 62 23 LIST OF IMPORTANT ORGANIZATIONS INDIA & THERE HEAD 65 24 LIST OF INTERNATIONAL ORGANIZATIONS AND HEADS 66 25 FACTS ABOUT CENSUS 2011 66 26 DEFENCE & TECHNOLOGY 67 27 BOOKS & AUTHOURS 69 28 LEADER”S VISITED INIDIA 70 29 OBITUARY 71 30 ORGANISATION AND THERE HEADQUARTERS 72 31 REVOLUTIONS IN AGRICULTURE IN INDIA 72 32 IMPORTANT DAMS IN INDIA 73 33 CLASSICAL DANCES IN INDIA 73 34 NUCLEAR POWER -

Medicine Update 2016) Brothers
Progress in Medicine 2016 (Medicine Update 2016) Brothers Jaypee For Private Circulation Only Progress in Medicine and Medicine Update 2016 The publication of this book has been made possible by Unconditional educational grant from: USV Limited The scientific committee is also thankful for the unconditionalBrothers grants from: India Medtronic Abbott Healthcare Mankind Pharma MICRO Labs Cipla Limited Dr Reddy’s Lab Eris Lifesciences, Intas Pharma, Macleods Pharma, Abbott Vasc., Zydus Cadila, IPCA, Sanofi Aventis, Novo Nordisk, and Emcure Pharma Volume 26–2016 ISBN: 978-93-5250-199-1 © All rights reserved. No part of this book may be reproduced by Xerox, microfilm or any other means without written permission from the editors and publisher. The editors have checked the validity of information provided in the book, and to the best of their knowledge, it is as per the standards accepted at the time of publication. The views and opinions of the authors do not represent the policies of The AssociationJaypee of Physicians of India or the editors. Published by Gurpreet S Wander, KK Pareek Design, Typeset, Print and Distributed by Jaypee Brothers Medical Publishers (P) Ltd Progress in Medicine 2016 (Medicine Update 2016) 1st VOLUME Chief Editors KK Pareek MD Senior Consultant in MedicineBrothers and Director SN Pareek Memorial Hospital and Research Center Kota, Rajasthan, India Gurpreet S Wander MD DM Professor and Head Department of Cardiology Hero DMC Heart Institute Dayanand Medical College and Hospital Ludhiana, Punjab, India Foreword Siddharth -

List of Fellows (Name-Wise) Upto 2016
LIST OF FELLOWS (NAME-WISE) UPTO 2016 0. Description Year 1. Abdul Kalam, A.P.J. Biomedical Engineering July 1995 DMIT. Former President, Republic of India. Res: 10 Rajaji Marg, New Delhi-110001. Permanent Address: No. 2, Mosque Street, Rameswaram, Ramanathapuram District, Tamil Nadu-623526. Tel: Off: (011) 3015321, 3014930, Res: (04567) 6493708, Fax: 2300756, E-mail: [email protected] (b 1931) (d.2015) Gen. Amir Chand Oration (NAMS, 1997-98) Padma Bhushan (1981); Padma Vibhushan (1990); Bharat Ratna (1997); D.Sc (h.c.) from several Universities; National Design Award; Dr. Biren Roy Space Award; Om Prakash Bhasin Award; National Nehru Award by Govt. of Madhya Pradesh; GM Modi Award for Science 1996; HK Firodia Award for Excellence in S&T 1996; Veer Savarkar Award 1998; Hon Fellow-Institution of Electronics and Telecommunication Engineers. 2. Abraham, Jacob Neurosurgery 1984 MS, MS (Neuro), FACS, FACA. Res: 10, 15th Avenue, Harrington Road, Chennai- 600031. Tel: Res: (044) 28363211, 42849258, Mobile: 09940118382, E-mail: [email protected] (b.1931). Basanti Devi Amir Chand Prize (ICMR, 1984); Sachs Memorial Lecturer, USA (1989). 3. Achari, Kamala Obstetrics and Gynecology 1982 MS, FRCOG, FICS, FACS. Emeritus Professor, Patna Medical College, Patna-800001 (Bihar). Res: 'Tirumalai', 21/D Road No.10, Rajendra Nagar, Patna- 800016. (b.1924) (d. 2014). 4. Adithan, C. Pharmacology July 2003 MD, PhD, FIMSA, FIPS. Former Professor & Head, Department of Pharmacology, Jawaharlal Institute of Postgraduate Medical Education & Research, Pondicherry- 605006. Currently: Director-CIDRF and Professor of Pharmacology, Mahatma Gandhi Medical College and Research Institute, Pondicherry-607403. Res: Flat No. 1, Srinivas Towers, Vazhudavour Road, Kathirkamam, Pondicherry-605009. -

Punjab Medical Council Electoral Rolls Upto 31-01-2018
Punjab Medical Council Electoral Rolls upto 31-01-2018 S.No. Name/ Father Name Qualification Address Date of Registration Validity Registration Number 1. Dr. Yash Pal Bhandari S/o L.M.S.F. 1948 81, Vijay Nagar, Jalandhar 12.04.1948 45 22.10.2018 Sh. Ram Krishan M.B.B.S. 1961 M.D. 1965 2. Dr. Balwant Singh S/o LSMF 1952 1814, Maharaj nagar, Near Gate No.3, 28.10.1952 3266 17.03.2021 Sh. Suhawa Singh M.B.B.S. 1964 of P.A.U., Ludhiana 3. Dr. Kanwal Kishore Arora S/o M.B.B.S. 1952 392, Adarsh Nagar Jalandhar 15.12.1952 3312 09.03.2019 Sh. Lal Chand Pasricha 4. Dr. Gurbax Singh S/o LSMF 1952 B-5/442, Kulam Road, Tehsil 11.03.1953 3396 23.04.2019 Sh. Mangal Singh M.B.B.S. 1956 Nawanshahr Distt. SBS Nagar D.O. 1957 5. Dr. Jawahar Lal Luthra L.S.M.F. 1953 H.No.44, Sector 11-A, Chandigarh 27.10.1953 3555 07.10.2018 M.B.B.S. 1956 M.S. (Ophth.) 1970 6. Dr. Kirpal Kaur M.B.B.S. 1953 490, Basant Avenue, Amritsar 09.12.1953 3599 31.03.2019 M.D. 1959 7. Dr. Harbans Kaur Saini L.S.M.F. 1954 Railway Road, Nawan Shahr Doaba 31.05.55 4092 29.01.2019 8. Dr. Baldev Raj Bhateja L.S.M.F. 1955 Raj Poly Clinic and Nursing Home, Pt. 08-06-1955 4106 09.10.2018 Jai Dayal St., Muktsar.