Anatomy Mnemonics Inner Wall Bones of Orbit
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Brachium and Cubital Fossa
Anatomy Guy Dissection Sheet 1/15/2012 Brachium and Cubital Fossa Dr. Craig Goodmurphy Anatomy Guy Major Dissection Objectives – Anterior Compartment 1. Maintain the superficial veins but work the fascia of the brachium off the anterior compartment noting the intermuscular septae 2. Clean and identify the three muscle of the anterior arm and their attachments 3. Mobilize the contents of the brachial fascia as it extends from the axillary fascia to the elbow noting the median, ulnar and medial brachial and medial antebrachial cutaneous nerves 4. Follow the musculocutaneous nerve as it passes through the coracobrachialis and between the biceps and brachialis noting motor branches and the lateral antebrachial cutaneous nerve Major Dissection Objectives – Cubital Fossa & Posterior Compartment 6. Mobilize the cubital fossa veins and review the boundaries 7. Clean the biceps tendon and reflect the aponeurosis 8. Locate the contents of the fossa including the bifurcation of the brachial artery, median nerve and floor muscles 9. Have a partner elevate the arm to dissect posteriorly and remove the skin and fascia 10. Locate the three heads of the triceps and their attachments 11. Locate the profunda brachii artery and radial nerve at the triangular interval and between the brachialis and brachioradialis muscles Eastern Virginia Medical School 1 Anatomy Guy Dissection Sheet 1/15/2012 Brachium and Cubital Fossa Pearls & Problems Don’t 1. Cut the biceps muscle just mobilize it Do 2. Follow the cords and tubes from known to unknown as you clean them Do 3. Remove the duplicated deep veins but save the unpaired superficial veins Do 4. -

Elbow Checklist
Workbook Musculoskeletal Ultrasound September 26, 2013 Shoulder Checklist Long biceps tendon Patient position: Facing the examiner Shoulder in slight medial rotation; elbow in flexion and supination Plane/ region: Transverse (axial): from a) intraarticular portion to b) myotendinous junction (at level of the pectoralis major tendon). What you will see: Long head of the biceps tendon Supraspinatus tendon Transverse humeral ligament Subscapularis tendon Lesser tuberosity Greater tuberosity Short head of the biceps Long head of the biceps (musculotendinous junction) Humeral shaft Pectoralis major tendon Plane/ region: Logitudinal (sagittal): What you will see: Long head of biceps; fibrillar structure Lesser tuberosity Long head of the biceps tendon Notes: Subscapularis muscle and tendon Patient position: Facing the examiner Shoulder in lateral rotation; elbow in flexion/ supination Plane/ region: longitudinal (axial): full vertical width of tendon. What you will see: Subscapularis muscle, tendon, and insertion Supraspinatus tendon Coracoid process Deltoid Greater tuberosity Lesser tuberosity Notes: Do passive medial/ lateral rotation while examining Plane/ region: Transverse (sagittal): What you will see: Lesser tuberosity Fascicles of subscapularis tendon Supraspinatus tendon Patient position: Lateral to examiner Shoulder in extension and medial rotation Hand on ipsilateral buttock Plane/ region: Longitudinal (oblique sagittal) Identify the intra-articular portion of biceps LH in the transverse plane; then -

The Square Flap Technique for Burn Contractures: Clinical Experience and Analysis of Length Gain
Annals of Burns and Fire Disasters - vol. XXXI - n. 4 - December 2018 THE SQUARE FLAP TECHNIQUE FOR BURN CONTRACTURES: CLINICAL EXPERIENCE AND ANALYSIS OF LENGTH GAIN DOUBLE LAMBEAU RHOMBOÏDE POUR BRIDE SÉQUELLAIRE DE BRÛ- LURE: EXPÉRIENCE PRATIQUE ET ANALYSE DE LA LONGUEUR GAGNÉE Hifny M.A. Department of Plastic Surgery, Faculty of Medicine, Qena University Hospital, South Valley University, Egypt SUMMARY. Post-burn contractures, affecting the joints especially, are demanding problems. Many surgical techniques have been designated for burn contracture release. The aim of this study is to investigate the efficiency of the square flap technique to release a post-burn scar contracture, and assess the post-operative length gain that can be achieved by simple mathematical calculation. In this study, sixteen patients with linear contracture bands were treated with the square flap tech- nique. The anatomical distribution of the contractures was: axilla, cubital fossa, flank, perineum and popliteal fossa. Scar maturity ranged from 4 months - 9 years. Square flap width and contracture band length before and immediately after surgery were recorded by simple mathematical calculation. Flap complication was assessed. Patient satisfaction was also assessed during the follow-up period. All square flaps were effective in lengthening the contracture bands. The length of the contracture that was released ranged from 2 to 6 cm. The gain in length provided with this technique ranged from 212 to 350%, average 247%, and adequate contracture release was achieved in all cases postoperatively. All square flaps healed uneventfully except for one (6%), which demonstrated limited epidermolysis that healed by secondary intention. The fol- low-up interval ranged from 6 months to 1.5 years. -
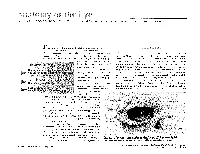
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Unusual Cubital Fossa Anatomy – Case Report
Anatomy Journal of Africa 2 (1): 80-83 (2013) Case Report UNUSUAL CUBITAL FOSSA ANATOMY – CASE REPORT Surekha D Shetty, Satheesha Nayak B, Naveen Kumar, Anitha Guru. Correspondence: Dr. Satheesha Nayak B, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka State, India. 576104 Email: [email protected] SUMMARY The median nerve is known to show variations in its origin, course, relations and distribution. But in almost all cases it passes through the cubital fossa. We saw a cubital fossa without a median nerve. The median nerve had a normal course in the upper part of front of the arm but in the distal third of the arm it passed in front of the medial epicondyle of humerus, surrounded by fleshy fibres of pronator teres muscle. Its course and distribution in the forearm was normal. In the same limb, the fleshy fibres of the brachialis muscle directly continued into the forearm as brachioradialis, there being no fibrous septum separating the two muscles from each other. The close relationship of the nerve to the epicondyle might make it vulnerable in the fractures of the epicondyle. The muscle fibres surrounding the nerve might pull up on the nerve and result in altered sensory-motor functions of the hand. Since the brachialis and brachioradialis are two muscles supplied by two different nerves, this continuity of the muscles might result in compression/entrapment of the radial nerve in it. Key words: Median nerve, cubital fossa, brachialis, brachioradialis, entrapment INTRODUCTION The median nerve is the main content of and broad tendon which is inserted into the cubital fossa along with brachial artery and ulnar tuberosity and to a rough surface on the biceps brachii tendon. -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. -

DEPARTMENT of ANATOMY IGMC SHIMLA Competency Based Under
DEPARTMENT OF ANATOMY IGMC SHIMLA Competency Based Under Graduate Curriculum - 2019 Number COMPETENCY Objective The student should be able to At the end of the session student should know AN1.1 Demonstrate normal anatomical position, various a) Define and demonstrate various positions and planes planes, relation, comparison, laterality & b) Anatomical terms used for lower trunk, limbs, joint movement in our body movements, bony features, blood vessels, nerves, fascia, muscles and clinical anatomy AN1.2 Describe composition of bone and bone marrow a) Various classifications of bones b) Structure of bone AN2.1 Describe parts, blood and nerve supply of a long bone a) Parts of young bone b) Types of epiphysis c) Blood supply of bone d) Nerve supply of bone AN2.2 Enumerate laws of ossification a) Development and ossification of bones with laws of ossification b) Medico legal and anthropological aspects of bones AN2.3 Enumerate special features of a sesamoid bone a) Enumerate various sesamoid bones with their features and functions AN2.4 Describe various types of cartilage with its structure & a) Differences between bones and cartilage distribution in body b) Characteristics features of cartilage c) Types of cartilage and their distribution in body AN2.5 Describe various joints with subtypes and examples a) Various classification of joints b) Features and different types of fibrous joints with examples c) Features of primary and secondary cartilaginous joints d) Different types of synovial joints e) Structure and function of typical synovial -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

MORPHOMETRIC and MORPHOLOGICAL ANALYSIS of FORAMEN OVALE in DRY HUMAN SKULLS Ashwini
International Journal of Anatomy and Research, Int J Anat Res 2017, Vol 5(1):3547-51. ISSN 2321-4287 Original Research Article DOI: https://dx.doi.org/10.16965/ijar.2017.109 MORPHOMETRIC AND MORPHOLOGICAL ANALYSIS OF FORAMEN OVALE IN DRY HUMAN SKULLS Ashwini. N.S *1, Venkateshu. K.V 2. *1 Assistant Professor, Department Of Anatomy,Sri Devaraj Urs Medical College ,Tamaka, Kolar, Karnataka, India. 2 Professor And Head, Department Of Anatomy ,Sri Devaraj Urs Medical College, Tamaka, Kolar, India. ABSTRACT Introduction: Foramen ovale is an important foramen in the middle cranial fossa. Foramen ovale is situated in the greater wing of sphenoid bone, posterior to the foramen rotandum. Through the foramen ovale the mandibular nerve, accessory meningeal artery, lesser petrosal nerve, emissary veins pass .The shape of the foramen ovale is usually oval compared to other foramen of the skull. Materials and Methods: The study was conducted on 55 dry human skulls(110 sides) in Department of Anatomy, Sri Devaraj Urs Medical college, Tamaka, Kolar. Skulls in poor condition or skulls with partially damaged surroundings around the foramen ovale were excluded from the study. Linear measurements were taken on right and left sides of foramen ovale using divider and meter rule. Results: The maximum length of foramen ovale was 14 mm on the right side and 17 mm on the left, its maximum breadth on the right side was 8mm and 10mm on the left . Through the statistical analysis of morphometric measurements between right and left foramen ovale which was found to be insignificant , the results of both sides marks as the evidence of asymmetry in the morphometry of the foramen ovale. -

Comprehensive Review of the Superficial Veins of the Forearm from a Historical, Anatomical and Clinical Point of View
IJAE Vol. 124, n. 2: 142-152, 2019 ITALIAN JOURNAL OF ANATOMY AND EMBRYOLOGY Circulatory system Comprehensive review of the superficial veins of the forearm from a historical, anatomical and clinical point of view Lucas Alves Sarmento Pires1,2,*, Albino Fonseca Junior1,2, Jorge Henrique Martins Manaia1,2, Tulio Fabiano Oliveira Leite3, Marcio Antonio Babinski1,2, Carlos Alberto Araujo Chagas2 1 Medical Sciences Post Graduation Program, Fluminense Federal University, Niterói, Rio de Janeiro, Brazil 2 Morphology Department, Fluminense Federal University, Niterói, Rio de Janeiro, Brazil 3 Interventional Radiology Unit, Radiology Institute, University of São Paulo Medical School, São Paulo, Brazil Abstract The superficial veins of the forearm are prone to possess different patterns of anastomosis. This is highly significant, as venipunctures in the upper limb are among the most performed procedures in the world and they often rely on the veins of the cubital fossa. In addition, the relationship of these veins to the cutaneous nerves are also prone to vary and are often uncer- tain. These veins are also manipulated in the creation of arteriovenous fistula for dialisis, which remains as the best choice of treatment for renal failure patients. Such fistulas are often per- formed on the wrist or the cubital fossa, with the cephalic vein or basilic vein. It is known that anatomical variations of the vessels and nerves on the cubital fossa may induce the profession- als to error, and one of the most common complications of venipuncture are accidental nerve puncture, which can lead to paresthesia and pain. We aim to perform a comprehensive review of the venous arrangements of the cubital fossa and their clinical aspects, as well as of veni- puncture from a historical perspective and of the complications of venipuncture and arterio- venous fistula from an anatomical point of view, with the purpose of compiling available data and help healthcare professionals to reduce puncture errors or arteriovenous fistula complica- tions and improve patient care.