Final Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MINMAP Région Du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX
MINMAP Région du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX N° Désignation des MO/MOD Nbre de Marchés Montant des Marchés N° page 1 Services déconcentrés Régionaux 19 2 278 252 000 4 Département de la Haute Sanaga 2 Services déconcentrés départementaux 6 291 434 000 7 3 COMMUNE DE BIBEY 2 77 000 000 8 4 COMMUNE DE LEMBE YEZOUM 8 119 000 000 8 5 COMMUNE DE MBANDJOCK 3 50 000 000 10 6 COMMUNE DE MINTA 5 152 500 000 10 7 COMMUNE DE NANGA-EBOKO 12 139 500 000 11 8 COMMUNE DE NKOTENG 5 76 000 000 13 9 COMMUNE DE NSEM 1 27 000 000 13 TOTAL 42 932 434 000 Département de la Lekié 10 Services déconcentrés départementaux 8 268 357 000 14 11 COMMUNE DE BATCHENGA 2 35 000 000 15 12 COMMUNE DE LOBO 8 247 000 000 15 13 COMMUNE DE MONATELE 11 171 500 000 16 14 COMMUNE DE SA'A 16 384 357 000 18 15 COMMUNE D'ELIG-MFOMO 7 125 000 000 20 16 COMMUNE D'EVODOULA 9 166 250 000 21 17 COMMUNE D'OBALA 14 223 500 000 22 18 COMMUNE D'OKOLA 22 752 956 000 24 19 COMMUNE D’EBEBDA 6 93 000 000 27 TOTAL 103 2 466 920 000 Département du Mbam et Inoubou 20 Services déconcentrés départementaux 4 86 000 000 28 21 COMMUNE DE BAFIA 5 75 500 000 28 22 COMMUNE DE BOKITO 12 213 000 000 29 23 COMMUNE DE KIIKI 4 134 000 000 31 24 COMMUNE DE KONYAMBETA 6 155 000 000 32 25 COMMUNE DE DEUK 2 77 000 000 33 26 COMMUNE DE MAKENENE 3 17 000 000 33 27 COMMUNE DE NDIKINIMEKI 4 84 000 000 34 28 COMMUNE D'OMBESSA 5 91 000 000 34 29 COMMUNE DE NITOUKOU 6 83 000 000 35 TOTAL 51 1 015 500 000 MINMAP/DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 88 N° Désignation -

Land Use and Land Cover Changes in the Centre Region of Cameroon
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 18 February 2020 Land Use and Land Cover changes in the Centre Region of Cameroon Tchindjang Mesmin; Saha Frédéric, Voundi Eric, Mbevo Fendoung Philippes, Ngo Makak Rose, Issan Ismaël and Tchoumbou Frédéric Sédric * Correspondence: Tchindjang Mesmin, Lecturer, University of Yaoundé 1 and scientific Coordinator of Global Mapping and Environmental Monitoring [email protected] Saha Frédéric, PhD student of the University of Yaoundé 1 and project manager of Global Mapping and Environmental Monitoring [email protected] Voundi Eric, PhD student of the University of Yaoundé 1 and technical manager of Global Mapping and Environmental Monitoring [email protected] Mbevo Fendoung Philippes PhD student of the University of Yaoundé 1 and internship at University of Liège Belgium; [email protected] Ngo Makak Rose, MSC, GIS and remote sensing specialist at Global Mapping and Environmental Monitoring; [email protected] Issan Ismaël, MSC and GIS specialist, [email protected] Tchoumbou Kemeni Frédéric Sédric MSC, database specialist, [email protected] Abstract: Cameroon territory is experiencing significant land use and land cover (LULC) changes since its independence in 1960. But the main relevant impacts are recorded since 1990 due to intensification of agricultural activities and urbanization. LULC effects and dynamics vary from one region to another according to the type of vegetation cover and activities. Using remote sensing, GIS and subsidiary data, this paper attempted to model the land use and land cover (LULC) change in the Centre Region of Cameroon that host Yaoundé metropolis. The rapid expansion of the city of Yaoundé drives to the land conversion with farmland intensification and forest depletion accelerating the rate at which land use and land cover (LULC) transformations take place. -

Proceedingsnord of the GENERAL CONFERENCE of LOCAL COUNCILS
REPUBLIC OF CAMEROON REPUBLIQUE DU CAMEROUN Peace - Work - Fatherland Paix - Travail - Patrie ------------------------- ------------------------- MINISTRY OF DECENTRALIZATION MINISTERE DE LA DECENTRALISATION AND LOCAL DEVELOPMENT ET DU DEVELOPPEMENT LOCAL Extrême PROCEEDINGSNord OF THE GENERAL CONFERENCE OF LOCAL COUNCILS Nord Theme: Deepening Decentralization: A New Face for Local Councils in Cameroon Adamaoua Nord-Ouest Yaounde Conference Centre, 6 and 7 February 2019 Sud- Ouest Ouest Centre Littoral Est Sud Published in July 2019 For any information on the General Conference on Local Councils - 2019 edition - or to obtain copies of this publication, please contact: Ministry of Decentralization and Local Development (MINDDEVEL) Website: www.minddevel.gov.cm Facebook: Ministère-de-la-Décentralisation-et-du-Développement-Local Twitter: @minddevelcamer.1 Reviewed by: MINDDEVEL/PRADEC-GIZ These proceedings have been published with the assistance of the German Federal Ministry for Economic Cooperation and Development (BMZ) through the Deutsche Gesellschaft für internationale Zusammenarbeit (GIZ) GmbH in the framework of the Support programme for municipal development (PROMUD). GIZ does not necessarily share the opinions expressed in this publication. The Ministry of Decentralisation and Local Development (MINDDEVEL) is fully responsible for this content. Contents Contents Foreword ..............................................................................................................................................................................5 -
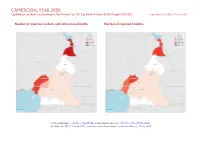
CAMEROON, YEAR 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 23 March 2021
CAMEROON, YEAR 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 23 March 2021 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, 6 May 2018b; administrative divisions: GADM, 6 May 2018a; incid- ent data: ACLED, 12 March 2021; coastlines and inland waters: Smith and Wessel, 1 May 2015 CAMEROON, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 MARCH 2021 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Violence against civilians 572 313 669 Conflict incidents by category 2 Battles 386 198 818 Development of conflict incidents from 2012 to 2020 2 Strategic developments 204 1 1 Protests 131 2 2 Methodology 3 Riots 63 28 38 Conflict incidents per province 4 Explosions / Remote 43 14 62 violence Localization of conflict incidents 4 Total 1399 556 1590 Disclaimer 5 This table is based on data from ACLED (datasets used: ACLED, 12 March 2021). Development of conflict incidents from 2012 to 2020 This graph is based on data from ACLED (datasets used: ACLED, 12 March 2021). 2 CAMEROON, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 MARCH 2021 Methodology on what level of detail is reported. Thus, towns may represent the wider region in which an incident occured, or the provincial capital may be used if only the province The data used in this report was collected by the Armed Conflict Location & Event is known. -

Est Centre Sud Littoral Ouest Est
Bazou IBRD 32132 5˚ 5˚ NDE NOUN 11˚ 12˚ 13˚ CAMEROON Tonga Nkongsamba OUEST PETROLEUMHAUT- DEVELOPMENT Bélabo AND PIPELINE PROJECT NKAM Nkongjok LOM-ET- Nginda Sanaga Towns and Villages Mentioned in Request Bafia DJEREM Ndikiniméki Mougué Rivers Mentioned in Request Pipeline Route Nanga Eboko Bakola Territory Nginda Ombessa MBAM Bakola Camps (1983 study, LOUNG, 1996) Ngamba Minta Bokito Rivers Wouri Yingui HAUTE-SANAGA YabassiMajor Rivers Nkoteng Paved Roads Ntuj All-Weather Roads Mbandjok Dim NKAM Ndom Nguélémendouka Unsurfaced Roads Saa Tracks/Trails Doume Railroads LITTORAL Monatélé Selected Towns/Villages Ngambé Department Capitals Obala Province Capital Nkon Ngok CENTRE National Capital LEKIE Essé Evodoula Abong Department Boundaries Sanaga Okola Mbang 4˚ 4˚ Province Boundaries Bot Makak Ngog Mapubi MEFOU Awaé NYONG-ET MFOUMOU Ayos 10˚ EST Pouma YAOUNDÉ Edéa Matomb Mbankomo Akonolinga Dzeng HAUT-NYONG SANAGA-MARITIME NYONG-ET-KELLE Mfou Messaména Messondo MFOUNDI Eséka Bikok Ngoumou Makak Nkongzok 1 Akono Mbalmayo Nyong Endom 10° 12° Lake 16° Elogbatindi Bengbis Chad ° 12 12° Nkoala'a CHAD CHAD Mvengué CAMEROON NYONG-ET-SO 10° 10° Ngovayang 2 Ngomedzap Bakola or Saballi Zoétélé Fifinda Bagyeli Bili-bi- Tchop Lolodorf Mbikiliki 8° 8° Bidjouka NIGERIA Lokoundjé Mougué Bikoui Gulf of Kouambo DJA-ET-LOBO CAMEROON Guinea Bandevouri Bipindi Ngoulemakong CENTRAL 6° Makouré 1 AFRICAN Dja 3˚ REPUBLIC 3˚ Kour Loundabele Tchangué Kribi Mintoum Sangmélima Area of Map Nkaga Zalé Ebolowa 4° 4° This map was produced by the YAOUNDE Mpango 0204060 80 100 Map Design Unit of The World Bank. OCEAN SUD The boundaries, colors, denominations Ebomé Kienké and any other information shown on this map do not imply, on the part of ATLANTIC For Detail, see Pembo River/swamp KILOMETERS The World Bank Group, any judgment OCEAN 10˚ Akom II 11˚ 12˚ on the legal status of any territory, or 13˚ IBRD 32148 any endorsement or acceptance of 2° NTEM such boundaries. -

Cameroon: June 2015
From experience to knowledge... From knowledge to action... From action to impact Country Strategy Evaluation Cameroon: An IDEV Country Strategy and Program Evaluation 2004–2013 Summary Report June 2015 Evaluation Syntheses IDEV conducts different types of evaluations — to achieve its Impact Evaluations Sector Evaluations (Public Sector) strategic objectives Project Performance Evaluations Thematic Evaluations Project Cluster Evaluations Project Performance Evaluations (Private Sector) Corporate Evaluations Regional Integration Strategy Evaluations Country Strategy Evaluation Country Strategy Evaluations From experience to knowledge... From knowledge to action... From action to impact Country Strategy Evaluation Cameroon: An IDEV Country Strategy and Program Evaluation 2004–2013 Summary Report June 2015 Acknowledgements This report was prepared by Herimandimby Razafindramanana, Evaluation Team Leader, under the supervision of Samer Hachem, Division Manager, with the support of a team composed of Samson Houetohossou, Research Assistant, and consultants Idir Kendel, Alain Rakotomavo, and Amacodou Ndiaye. This work benefited from the comments and contributions of colleagues from different Bank Departments, especially the Bank’s Field Office in Cameroon (CMFO) and country team. Independent Development Evaluation (IDEV) wishes to thank the Cameroonian Authorities, in particular, MINEPAT as well as all the people and institutions that contributed to the preparation of this report. IDEV is solely responsible for the contents. The publication -

Consultancy Report on Vegetable Seeds
Integrated Agricultural Systems for the Humidtropics, a CGIAR Research Project Consultancy Report on Vegetable Seeds Baseline survey for setting up smallholders’ sustainable vegetable seed supply and distribution system in humid tropics areas of Cameroon Team Members Tata Precillia Ijang (Team leader) Dr Ngome Francis Godswill Ntsomboh Ntsefong Ngayong Joseph Wirngo December 2013 Executive Summary The Cameroon seed sector is developing slowly and steadily and there is political will through government legislation and requirements to foster the development of the sector with a view to boosting the agricultural sector as well as stimulating the economy as a whole. The seed sector activity is regulated by law N o 2001/014 of 23 rd July 2001 relating to seed production and marketing and its instruments of application. Decision N o 541/MINADER/SG/DRCQ/SDRSQV of 7 th September 2006 on the homologation of official technical regulation of quality control of certain vegetable seeds complements the law of July 2001 and specifically applies to the production, importation and quality control and marketing of vegetable seeds. The public sector has a definite contribution to promote the development of the seed sector in Cameroon. Through the Department of Quality Regulation and Control of Inputs and Agricultural Products of the Ministry of Agriculture and Rural Development, the state ensures regulation of seeds and vegetable quarantine as well as the breeding of various species of seeds. At present this department controls one national breeding centre and ten regional ones that supply seeds to various stakeholders of the seed sector in Cameroon. The role of public sector is mainly catalytic in initiating seed production, quality control, seed certification, notification and registration of varieties and other regulatory systems. -

China in Cameroon's Forests
China in Cameroon’s forests A review of issues and progress for livelihoods and sustainability James Mayers, Samuel Nguiffo and Samuel Assembe-Mvondo This research report has been prepared as part of the China-Africa Forest Governance Project – a multi-country project that seeks to improve forest governance, by promoting sustainable and pro-poor Chinese trade and investment in Africa’s forest. Through research, dialogue and joint action with partners in China, Cameroon, the Democratic Republic of Congo, Mozambique and Uganda, the project contributes to improved policy and investment practice in China and Africa, in ways that foster good stewardship of forest resources and benefit local communities. The project is run by IIED with support from the UK government and partnerships with WWF and in-country practitioner teams with a strong track record of governance and enterprise engagement. Country reports, as well as other thematic and sectoral research products, on the state of Chinese investments in African land use are free to download at pubs.iied.org. For more information visit www.iied.org/china-africa-forest-governance-project. The China-Africa Forest Governance Platform, launched in 2013, is now a well-recognised multi-stakeholder forum which strengthens mutual understanding, partnerships and joint actions on forest governance between China and Africa. Platform participants have also had influence in key international policy arenas. While the China- Africa Forest Governance Project has been the main supporter of the platform to date, other organisations continue to increase their involvement. The platform has thus far brought together forest governance players, including heads of government forest departments from nine African countries; representatives from the Chinese Academy of Forestry; the Global Environmental Institute; the International Institute for Environment and Development; the World Wide Fund for Nature; and other international organisations. -
Catalogue Des Exposants De Mfou
Participation de la Commune de Mfou à la première Édition du comice agropastoral et social de la Mefou et Afamba (COMAF) Awae 2021 Catalogue des exposants de Mfou avec visage économique et institutionnel de la Commune Le COMAF en Bref Le COMAF, Comice Agropas- et de communication vers le reste de sont grandes ; il convient juste de les toral et Social de la Mefou et Afam- la Région du Centre, la Communauté identifier, de les organiser et de les ba, a pour objectif général d’exposer Nationale et Internationale. promouvoir. le fruit du travail des producteurs du La Mefou et Afamba entend L’organisation du COMAF est département de la Mefou et Afamba saisir cette opportunité pour enta- assurée par la COODEL (Conférence ainsi que leurs ambitions en matières mer sa propre révolution et être un des Organisations de Solidarité et De- économique, sociale et culturelle. Il exemple de réussite économique car veloppement Local de la Mefou et se veut aussi un espace d’ouverture les potentialités dans ce Département Afamba) Vision managériale de l’Exécutif Communal de Mfou MBEZELE EYENGA Xaverie épouse MANGA Francis NGOUMOU AMOUGOU ETOGO Roland La vision managériale de l’Exé- cutif Communale de Mfou ambitionne la modernisation institutionnelle et en environnementale d’une part et d’autre part l’amélioration du cadre et des condi- tions de vie des populations. Cette vision se décline sur plusieurs axes principaux dont : Les ressources humaines ; Les res- sources financières ; Le patrimoine com- munal ; La coopération ; La communi- cation et l’information. -

Cameroon's Forest Estate
13° E 14° E 15° E 16° E N N ° ° 3 3 CAMEROON'S FOREST ESTATE 1 1 MINISTRY OF December 2016 FORESTRY AND WILDLIFE p SUMMARY OF LAND USE ALLOCATION WITHIN LEGEND THE NATIONAL FOREST ESTATE IN 2016 Kalamaloué ! National Park N KOUSSÉRI N ° ° Permanent Forest Estate (PFE) 2 2 LLÉoGcEaNliDtyE 1 1 Allocation type Number Area (ha) Ç " Political capital Forest Management Units (FMU) 115 6 803 483 Ç ' Regional capital Designated with management plans approved 86 5 124 133 ! Town Proposed with management plans approved 13 817 329 Infrastructure Designated with management plans in process of elaboration 5 248 614 National road Proposed with management plans in process of elaboration 4 157 158 Regional road Designated and not managed 5 366 030 Railway Waza Proposed and not mananged 2 90 219 National Park Forest reserves 56 492 166 Forest Management Unit Protected areas (PA) 37 4 761 683 Designated, management plan approved ! N MORA N ° ° National Parks 26 3 645 994 Proposed, management plan approved 1 1 1 Mozogo Gokoro CHAD 1 Wildlife reserves 5 966 272 Designated, management plan in process National Park Sanctuaries 6 149 417 Proposed, management plan in process ! Hunting zones (ZIC/ZICGC) 67 5 340 858 Designated, not managed MOKOLO Council Forests (FC) 64 1 646 047 Proposed, not managed '! Council Forest Designated 41 1046 335 MAROUA Proposed 23 599 712 Designated Proposed Non Permanent Forest Estate (nPFE) ! Kalfou Community forests (Fcom) 544 1 864 388 Sale of standing volume Laf Madiam YAGOUA Provisional conventions 260 875 870 Active KAÉLÉ ! Final conventions 284 988 518 Inactive Ma Mbed Mbed N N ° National Park ° Sales of Standing Volume (SSV) 186 319 735 0 0 Protected area 1 !GUIDER 1 Agro-industrial parcels 74 415 937 Designated Areas in this table come from official documents (decree, public notice, management convention, etc.) for FMU, Proposed PA, ZIC&ZICGC, FC, Fcom and SSV. -

CAMEROUN (Plus De 2 000 000 Hab.) Aéroport, Aérodrome Plus De 2 000 000 Hab
12° vers NGUIGMI Capitale d'État Voie ferrée NIGER CAMEROUN (plus de 2 000 000 hab.) Aéroport, aérodrome Plus de 2 000 000 hab. vers MASSAKORI 16° Limite de région LAC TCHAD vers ATI Plus de 200 000 hab. (niveau moyen : 280 m) Plus de 100 000 hab. Limite de département Ngouma Makari Bertoua Capitale de région Fotokol Plus de 50 000 hab. Goulfey NDJAMENA Plus de 20 000 hab. Banyo Chef-lieu de département MaltMaltamam 12° Autre ville ou localité Barrage, chute DIKWA é 12° Kouss ri MAIDUGURI Route principale Logone Marais, terrain inondable Birni Route secondaire DAMATURU Parc national ou réserve HinalHinaléé BAMA Ndiguina T Autre route ou piste Waza PARC NAT. 0 100 200 km vers KANO vers GASHUA vers ZINDER DE WAZA C Kolofata H vers BOUSSO vers SARH versBANGUI A C R A Mora I vers POTISKUM R A D1442 N Ê A EXTR ME-NORD M Bogo A Méri H vers BAUCHI BIU Mokolo Maroua S T M Koré GOMBE I MUBI Bourrah Mindif BONGOR Yagoua A i t Kaélé Guibi CAMEROUN Dourbey Guider u o L . R l e M vers BAUCHI i i T Figuil bb FIANGA D . LÉRÉ Ké M yo Ma LO G NUMAN O N É Garoua PALA KÉLO E E Bibémi Boïli NU LAÏ BE B én YOLA oué Lagdo Touroua Dobinga o Béré vers JOS vers JOS v. DOBA r a WAMBA G F SHENDAM JALINGO Boumedjé Lac de Rey Bouba Lagdo A Tchamba PARC NAT. IK DE BOUBA MOUNDOU NT A NDJIDA LAFIA L 1886 Poli AL GANYE A T 1494 PARC NAT. -

Centre De Douala
AO/CBGI REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON Paix –Travail – Patrie Peace – Work – Fatherland -------------- --------------- MINISTERE DE LA FONCTION PUBLIQUE MINISTRY OF THE PUBLIC SERVICE ET DE LA REFORME ADMINISTRATIVE AND ADMINISTRATIVE REFORM --------------- --------------- SECRETARIAT GENERAL SECRETARIAT GENERAL --------------- --------------- DIRECTION DU DEVELOPPEMENT DEPARTMENT OF STATE HUMAN DES RESSOURCES HUMAINES DE L’ETAT RESSOURCES DEVELOPMENT --------------- --------------- SOUS-DIRECTION DES CONCOURS SUB DEPARTMENT OF EXAMINATIONS ------------------ -------------------- CONCOURS DIRECT POUR LE RECRUTEMENT DE 30 CONTRÔLEURS-ADJOINTS DU TRAVAIL ET DE LA PRÉVOYANCE SOCIALE SESSION 2020 CENTRE DE DOUALA LISTE DES CANDIDATS AUTORISÉS À SUBIR LES ÉPREUVES ÉCRITES DU 13 SEPTEMBRE 2020 RÉGION DÉPARTEMENT NO MATRICULE NOMS ET PRÉNOMS DATE ET LIEU DE NAISSANCE SEXE LANGUE D’ORIGINE D’ORIGINE 1. CATPD0617 ABDOUL MOUHAIMIN NOUROUDDINE 19/07/1993 A NGAOUNDERE M AD VINA F 2. CATPD1753 ABDOURAHMAN DJIBRILLA 12/12/1997 A MAROUA M EN DIAMARE F 3. CATPD0976 ABIBATOU MADONE TONGOU 13/10/1994 A NGAOUNDERE F AD DJEREM F 4. CATPD0752 ABOGO MARIUS BANDOUIN 20/01/1994 A EKOKOM M CE LEKIE F 5. CATPD1222 ADAMA SALISSOU 08/10/1995 A DOUALA F AD VINA F MINFOPRA/SG/DDRHE/SDC|Liste générale des candidats Contrôleurs-Adjoints du Travail et de la Prévoyance Sociale, session 2020_Douala Page 1 6. CATPD1617 ADAMOU SALIOU BAPETEL 04/04/1997 A TCHOUKE M NO MAYO REY F 7. CATPD0411 ADIDJA OUMARU 09/10/1992 A DOUALA F AD MAYO BANYO F 8. CATPD0527 ALANG ABOUEME MARTHE ROSE 15/03/1993 A DONENKENG BAFIA F CE MBAM ET INOUBOU F 9. CATPW0759 ALONGOH BIDJEHA STEVE FRED 01/02/1994 A BAFOUSSAM M ES HAUT NYONG F 10.