Rotator Cuff & Scapular Strengthening for the Shoulder Exercises
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Scapular Motion Tracking Using Acromion Skin Marker Cluster: in Vitro Accuracy Assessment
Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti, Claudio Rosso, Ara Nazarian, Joseph P. DeAngelis, Arun J. Ramappa & Ugo Della Croce Journal of Medical and Biological Engineering ISSN 1609-0985 J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 1 23 Your article is protected by copyright and all rights are held exclusively by Taiwanese Society of Biomedical Engineering. This e- offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 ORIGINAL ARTICLE Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti • Claudio Rosso • Ara Nazarian • Joseph P. DeAngelis • Arun J. Ramappa • Ugo Della Croce Received: 11 October 2013 / Accepted: 20 March 2014 Ó Taiwanese Society of Biomedical Engineering 2015 Abstract Several studies have recently investigated how estimated using an AMC combined with a single anatom- the implementations of acromion marker clusters (AMCs) ical calibration, the accuracy was highly dependent on the method and stereo-photogrammetry affect the estimates of specimen and the type of motion (maximum errors between scapula kinematics. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Evaluation of Humeral and Glenoid Bone Deformity in Glenohumeral Arthritis 5
Evaluation of Humeral and Glenoid Bone Deformity 1 in Glenohumeral Arthritis Brian F. Grogan and Charles M. Jobin Introduction glenoid bone wear helps the surgeon formulate a successful treatment plan and surgical goals Glenohumeral arthritis is the sequela of a vari- to address the pathoanatomy and improve the ety of pathologic shoulder processes, most durability of shoulder arthroplasty. The evalu- commonly degenerative osteoarthritis, but may ation of humeral and glenoid bone deformity also be secondary to post-traumatic conditions, in glenohumeral arthritis has profound surgical inflammatory arthritis, rotator cuff tear arthrop- implications and is fundamental to successful athy, and postsurgical conditions most com- shoulder arthroplasty. monly post-capsulorrhaphy arthritis. Patients with glenohumeral arthritis commonly demon- strate patterns of bony deformity on the glenoid Glenoid Deformity in Osteoarthritis and humerus that are caused by the etiology of the arthritis. For example, osteoarthritis com- Glenoid deformity and glenohumeral subluxation monly presents with posterior glenoid wear, are commonly seen in the setting of primary osteo- secondary glenoid retroversion, and posterior arthritis of the glenohumeral joint. The glenoid humeral head subluxation, while inflammatory wear tends to occur posteriorly and may be best arthritis routinely causes concentric glenoid viewed on axial radiographs or computed tomog- wear with central glenoid erosion. A thorough raphy (CT) axial images. Glenoid erosion, as first history and physical, as well as laboratory and characterized by Walch, is noted to be either central radiographic workup, are keys to understanding or posterior, with varying degrees of wear and pos- the etiology of arthritis and understanding the terior subluxation of the humerus [1, 2] (Fig. -

Integrating the Shoulder Complex to the Body As a Whole: Practical Applications for the Dancer
RESOURCE PAPER FOR TEACHERS INTEGRATING THE SHOULDER COMPLEX TO THE BODY AS A WHOLE: PRACTICAL APPLICATIONS FOR THE DANCER LISA DONEGAN SHOAF, DPT, PHD AND JUDITH STEEL MA, CMA WITH THE IADMS DANCE EDUCATORS’ COMMITTEE, 2018. TABLE OF CONTENTS 1. Introduction 2 2. Anatomy and Movements of the Shoulder Complex 3 3. Force Couples: Muscle Connections of the Scapula and Upper Extremity 12 4. The Shoulder Joint and Rotator Cuff Muscles 17 5. Integration of the Shoulder Girdle to the Trunk, Pelvis and Lower Extremities 20 6. Common Dancer Issues in the Upper Extremity 22 7. Summary 25 8. Illustration Credits 26 9. Recommended Reading 27 10. The Authors 28 1. INTRODUCTION Figure 1: Ease and elegance in the shoulder complex The focus in many forms of dance training is often on the movements of the lower body- the legs and feet. Movement of the upper body- trunk, shoulders, and arms, is often introduced later. Because so much emphasis is placed on function of the trunk and legs, and since most injuries for dancers occur in the lower body regions, it is easy to overlook the importance of optimal function of the shoulder and arms. The shoulder complex (defined as the humerus, clavicle, sternum, and scapula bones that form a girdle or shawl over the rib cage) in combination with its connection to the trunk and, ultimately, the lower body, has many components. There are three important concepts (listed below) that, when understood and experienced, can help dance educators and dancers better make the important connections to merge maximal range of motion with well aligned and supported movements that create full body artistic expressiveness. -
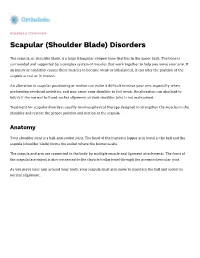
Scapular (Shoulder Blade) Disorders
DISEASES & CONDITIONS Scapular (Shoulder Blade) Disorders The scapula, or shoulder blade, is a large triangular-shaped bone that lies in the upper back. The bone is surrounded and supported by a complex system of muscles that work together to help you move your arm. If an injury or condition causes these muscles to become weak or imbalanced, it can alter the position of the scapula at rest or in motion. An alteration in scapular positioning or motion can make it difficult to move your arm, especially when performing overhead activities, and may cause your shoulder to feel weak. An alteration can also lead to injury if the normal ball-and-socket alignment of your shoulder joint is not maintained. Treatment for scapular disorders usually involves physical therapy designed to strengthen the muscles in the shoulder and restore the proper position and motion of the scapula. Anatomy Your shoulder joint is a ball-and-socket joint. The head of the humerus (upper arm bone) is the ball and the scapula (shoulder blade) forms the socket where the humerus sits. The scapula and arm are connected to the body by multiple muscle and ligament attachments. The front of the scapula (acromion) is also connected to the clavicle (collarbone) through the acromioclavicular joint. As you move your arm around your body, your scapula must also move to maintain the ball and socket in normal alignment. (Left) The bones of the shoulder. The scapula serves as a site for the attachment of multiple muscles around the shoulder. (Right) The muscles and soft tissues of the shoulder. -

Chapter 5 the Shoulder Joint
The Shoulder Joint • Shoulder joint is attached to axial skeleton via the clavicle at SC joint • Scapula movement usually occurs with movement of humerus Chapter 5 – Humeral flexion & abduction require scapula The Shoulder Joint elevation, rotation upward, & abduction – Humeral adduction & extension results in scapula depression, rotation downward, & adduction Manual of Structural Kinesiology – Scapula abduction occurs with humeral internal R.T. Floyd, EdD, ATC, CSCS rotation & horizontal adduction – Scapula adduction occurs with humeral external rotation & horizontal abduction © McGraw-Hill Higher Education. All rights reserved. 5-1 © McGraw-Hill Higher Education. All rights reserved. 5-2 The Shoulder Joint Bones • Wide range of motion of the shoulder joint in • Scapula, clavicle, & humerus serve as many different planes requires a significant attachments for shoulder joint muscles amount of laxity – Scapular landmarks • Common to have instability problems • supraspinatus fossa – Rotator cuff impingement • infraspinatus fossa – Subluxations & dislocations • subscapular fossa • spine of the scapula • The price of mobility is reduced stability • glenoid cavity • The more mobile a joint is, the less stable it • coracoid process is & the more stable it is, the less mobile • acromion process • inferior angle © McGraw-Hill Higher Education. All rights reserved. 5-3 © McGraw-Hill Higher Education. All rights reserved. From Seeley RR, Stephens TD, Tate P: Anatomy and physiology , ed 7, 5-4 New York, 2006, McGraw-Hill Bones Bones • Scapula, clavicle, & humerus serve as • Key bony landmarks attachments for shoulder joint muscles – Acromion process – Humeral landmarks – Glenoid fossa • Head – Lateral border • Greater tubercle – Inferior angle • Lesser tubercle – Medial border • Intertubercular groove • Deltoid tuberosity – Superior angle – Spine of the scapula © McGraw-Hill Higher Education. -

Muscles of the Upper Limb.Pdf
11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles of the Upper Limb Pectoralis minor ORIGIN: INNERVATION: anterior surface of pectoral nerves ribs 3 – 5 ACTION: INSERTION: protracts / depresses scapula coracoid process (scapula) (Anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Serratus anterior Subclavius ORIGIN: INNERVATION: ORIGIN: INNERVATION: ribs 1 - 8 long thoracic nerve rib 1 ---------------- INSERTION: ACTION: INSERTION: ACTION: medial border of scapula rotates scapula laterally inferior surface of scapula stabilizes / depresses pectoral girdle (Lateral view) (anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Trapezius Levator scapulae ORIGIN: INNERVATION: ORIGIN: INNERVATION: occipital bone / spinous accessory nerve transverse processes of C1 – C4 dorsal scapular nerve processes of C7 – T12 ACTION: INSERTION: ACTION: INSERTION: stabilizes / elevates / retracts / upper medial border of scapula elevates / adducts scapula acromion / spine of scapula; rotates scapula lateral third of clavicle (Posterior view) (Posterior view) 1 11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles Moving Arm Rhomboids Pectoralis major (major / minor) ORIGIN: INNERVATION: ORIGIN: INNERVATION: spinous processes of C7 – T5 dorsal scapular nerve sternum / clavicle / ribs 1 – 6 dorsal scapular nerve INSERTION: ACTION: INSERTION: ACTION: medial border of scapula adducts / rotates scapula intertubucular sulcus / greater tubercle flexes / medially rotates / (humerus) adducts -

Right Or Left Bones? Clavicle Ulna
Right or Left Bones? Clavicle Ulna . Together, the clavicles make a . Lay the ulna on the table. “handlebar” shape (low at the middle . Can you see the radial notch? of the chest, higher near the shoulders). o If yes, the open side of the . The blunt tip (sternal end) touches the trochlear (semilunar) notch tells sternum at the middle of the chest. you the bone orientation (see . The round tip (acromial end) touches the photo 1). scapula at the shoulder. o If no, the open side of the . The bumpy side of the clavicle faces the trochlear (semilunar) notch is the rib cage. opposite of the bone orientation . The smooth side of the clavicle faces (see photo 2). outward Radius Fibula . The styloid process always touches the . The smoother tip (head of the fibula) thumb. touches the knee. If the lower end of the radius (near the . The rougher tip (lateral malleolus) styloid process) is rough, you are touches the ankle. looking at the back of the wrist. The point of the lateral malleolus points . If the lower end of the radius is smooth, to the pinkie toe, not the middle of the you are looking at the inside of the wrist. foot. The front of the fibula (anterior view) has an edge. The back of the fibula (posterior view) is flat. References: University of Liverpool Faculty of Health and Life Sciences. (2013). Radius and ulna (right forearm) [Digital photograph]. Retrieved from https://www.flickr.com/photos/liverpoolhls/10819145494. . -

Scapula Fractures
Ministry of Defence Synopsis of Causation Scapula Fractures Author: Mr Darren P Forward, Queen’s Medical Centre, Nottingham Professor W Angus Wallace, Queen’s Medical Centre, Nottingham Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A scapular fracture is a break in the continuity of the cortex of the scapula bone. Scapular fractures are uncommon. They represent 1%1 of all fractures and 3%1 of shoulder-girdle injuries. 1.2. To aid prognosis, they can be classified into 3 groups.2 1.2.1. Type 1: 54% Fractures of the body. 1.2.2. Type 2: 17% Fractures of the acromion, spine, and coracoid process. 1.2.3. Type 3: 29% Fractures of the glenoid rim and fossa, and anatomical and surgical necks. 1.3. -

Scapular Winging Serratus Anterior Palsy, Long Thoracic Nerve Injury
Scapular Winging Serratus Anterior Palsy, Long Thoracic Nerve Injury Scapular winging is an uncommon nerve condition, causing pain and occasionally weakness in the shoulder. It involves injury to the long thoracic nerve in the back near the shoulder blade. The long thoracic nerve runs from the neck along the chest wall to the serratus anterior muscle. The nerve can be stretched due to a fall on the shoulder while the neck bends toward the other shoulder, it can be the result of repetitive injury, or it may occur without injury; sometimes it is associated with a viral illness. Injury to this nerve results in weakness of the serratus anterior muscle, causing the shoulder blade (scapula) to pull away from the chest wall with attempted shoulder movement, called winging. The scapula is the base from which the shoulder functions. With winging, the shoulder works off a weak base, making shoulder function weak as well. Frequent Signs and Symptoms • Pain and discomfort (burning or dull ache) that is poorly localized, often in the back of the shoulder or shoulder blade • Heaviness or fatigue of the arm • Loss of power of the shoulder • Difficulty raising the arm above shoulder level • Pain in the back when sitting in a chair with a high back due to the scapula hitting the back of the chair • Bump in the back of the shoulder (the scapula) that is more obvious when trying to do push- ups or reach forward overhead Etiology (Causes) • Viral illness • Repetitive stretch injury • Fall onto shoulder with the head and neck stretched away from the shoulder Risk Factors • Contact sports • Sports that require overhead throwing type activity, such as baseball, volleyball, and tennis • Poor physical conditioning (strength and flexibility) 630-324-0402 [email protected] Orthopaedic Surgery & Sports Medicine Teaching & Research Foundation stevenchudikmd.com otrfund.org Schedule online now © 2018 Steven Chudik MD Shoulder, Knee & Sports Medicine. -

The Scapula Scapulothoracic Dyskinesis
The Scapula The Normal Scapula The scapula is a triangular bone and the outer (lateral) end of this bone is the socket of the shoulder joint. Normal movement of the scapula allows us to use the shoulder and arm in sports, work and daily living. Upward and forward rotation allows us to raise our arms overhead. This is achieved by several muscles attaching to the scapula. The Serratus Anterior pulls the scapula forward and rotates the socket upward. The Trapezius rotates the scapula outward and the socket upward. Scapulothoracic Dyskinesis What is it? Scapulothoracic dyskenesis may be the result of fatigue of the scapular stabilizing muscles, and this may occur from overhead sports or work activities. Indeed, athletes with shoulder pain will often have abnormal scapular movement and this is an important part of their recovery with a physical therapy rehabilitation program. In its most severe form Scapulothoracic dyskenesis is the result of a nerve dysfunction either from trauma or idiopathic causes. Loss of scapular control is often missed. The patient may develop pain in his(her) shoulder and there may or may not be loss of overall shoulder motion. In some cases the patient may have shoulder instability due to failure of the scapula to fully rotate. Some patients present with pain that may seem like a rotator cuff problem. This is due to abnormal motion which allows the rotator cuff to hit against the acromion bone. This condition has been called impingement. Scapulothoracic Winging What is it? If one or more of the scapular stabilizing muscles does not work properly the scapula wings and moves in the opposite direction of the shoulder joint (Fig.