IDL-47373.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Interim Report Fifth Council Meeting and Fourth Conference of ASSECAA Held in Rabat Morocco Day One 12Th November 2009
ASSOCIATION OF SENATES, SHOORA AND رابطة مجالس الشيوخ والشورى والمجالس EQUIVALENT COUNCILS المماثلة في أفريقيا والعالم العـربـي IN AFRICA AND THE ARAB WORLD ASSOCIATION DES SENATS, SHOORA ET CONSEILS EQUIVALENTS D’AFRIQUE ET DU MONDE ARABE Interim Report Fifth Council Meeting and Fourth Conference of ASSECAA Held in Rabat Morocco Day One 12th November 2009. COUNCIL MEETING The Outgoing Chairman of the Association, H.E Ali Yahiya Abdallah in the chair 1.0 Preamble 1.1 Under the supreme auspices of His Majesty, Mohammed VI, King of the Kingdom of Morocco and at the kind invitation of H.E Dr. Mohammed Al- Cheikh Baidallah, Speaker of the House of Counselors of Morocco, the fourth conference and the fifth Council meeting of the Association of Senates, Shoora and Equivalent Councils in Africa and the Arab world (ASSECAA) were held in Rabat, Morocco, from 12-13 November 2009. 1.2 The meetings were held in joyous atmosphere of optimism, constructive understanding and common keenness on enhancing cooperation and buttressing common interests of Africa and Arab world. ASSOCIATION OF SENATES, SHOORA AND رابطة مجالس الشيوخ والشورى والمجالس EQUIVALENT COUNCILS المماثلة في أفريقيا والعالم العـربـي IN AFRICA AND THE ARAB WORLD ASSOCIATION DES SENATS, SHOORA ET CONSEILS EQUIVALENTS D’AFRIQUE ET DU MONDE ARABE 1.3 The meetings were characterized by fervent enthusiasm and determination on the part of member countries, to attain the objectives for which the Association was established. 1.4 Foremost among such objectives is the consolidation of economic cooperation, bicameralism, development of common action at the political, socio-economic and cultural levels and coordination among the countries of the two regions with the aim of surmounting all obstacles to stability and development, eliminating all causes of tension and conflicts and harnessing the abundant potentials, available in the region, for the betterment of its nations. -

Download the Complete Volume for 2017
Midlands Historical Review Volume 1 2017 Cover Image. Detail from Britannia Saxonica (1695) by Robert Morden. Held within the Public Domain and accessed via Wikimedia Commons. Midlands Historical Review ISSN 2516-8568 Volume I, 2017 Published by the Midlands Historical Review With thanks to the editorial board. David Civil, Founding Editor David Robinson, Founding Editor Jonathan Roche, Founding Editor Gary Fisher, Founding Editor With thanks to the assistant editors Thomas Black Christopher Booth Kate Garland Joe Himsworth Joanne Lord Darcie Mawby Marco Panato Thomas Rose James Smith Kimberley Weir Published by Midlands Historical Review © 2018 Midlands Historical Review Midlands Historical Review Founded 2017 Midlands Historical Review is an interdisciplinary, peer-reviewed, student-led journal which showcases the best student research in the Arts and Humanities. It was founded in 2017 by a group of PhD students from diverse academic backgrounds and receives support from the University of Nottingham’s Department of History and School of Humanities. Students in the Arts and Humanities produce valuable contributions to knowledge which, once a degree has been awarded, are often forgotten. High quality research deserves an audience regardless of the level of education it was produced for. The research published by the Midlands Historical Review encourages and enables later cohorts of students to build upon previous students’ work. Contents Human Nature and the Joint Social Project: Towards a Coherent 1 Notion of Alienation Gaby Beckley Guess Who’s Coming to Dinner and Hollywood’s 17 Misrepresentation of the Politics of Interracial Relationships in 1960s America Sarah Dunne Ants and Cicadas: South American Football and National Identity 28 Mark Orton Pierre Nora, Memory, and the Myth of Elizabeth I 49 Tom Rose The Iconography of Kingship: Masques, Antimasques, and 66 Pastorals Thomas Black The “Russian” Woman? Cultural Exceptionalism among 88 Noblewomen in Late Imperial and Revolutionary Russia Darcie Mawby Book Reviews Belief and Unbelief in Medieval Europe. -

FIFA Arab Cup 2021 Will Capture Attention of Fans Everywhere: QFA Chief Sheikh Hamad
Cancun World QatarTribune Qatar_Tribune Tour Beach QatarTribuneChannel qatar_tribune Volleyball silver for Cherif and Ahmed again WEDNESDAY, APRIL 28, 2021 PAGE 14 FIFA Arab Cup 2021 will capture attention of fans everywhere: QFA chief Sheikh Hamad Nawaf Al Temyat, Deputy Vice-President of Saudi Arabia Football Federation holds out Qatar’s name during the FIFA Arab Cup 2021 draw at Katara Opera House on Tuesday. TRIBUNE NEWS NETWORK Committee for Delivery & Leg- DOHA acy Secretary-General Hassan Al Thawadi said, “This tour- THE first-ever FIFA Arab Cup nament will see elite teams 2021 will capture the imagi- from across the Arab world nation and attention of fans compete in a FIFA-sanctioned everywhere, said Qatar Foot- tournament for the first time. ball Association President HE A tournament of this magni- Sheikh Hamad bin Khalifa bin tude – played exactly a year Ahmed Al Thani on Tuesday. before the World Cup – is sure Sheikh Hamad was among to excite our football crazy the many dignitaries who at- region as we continue prepa- tended the draw ceremony for rations for 2022. We look the firstFIFA Arab Cup 2021 forward to hosting the FIFA FIFA President Gianni Infantino; HE Sheikh Joaan bin Hamad Al Thani, President, Qatar Olympic Committee; HE Sheikh Hamad bin Khalifa bin Ahmed Al Thani, President, Qatar at the Katara Opera House. Arab Cup and using the tour- Football Association; Hassan Al Thawadi, Secretary-General, Supreme Committee for Delivery & Legacy; Nasser Al Khater, CEO, FIFA World Cup Qatar 2022; and others during the “Qatar is very excited to nament to confirm our plans FIFA Arab Cup 2021 draw ceremony at Katara Opera House on Tuesday. -
Qnbfs.Com.Qa Doha, Qatar
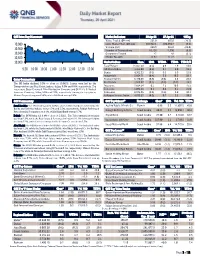
QSE Intra-Day Movement Market Indicators 28 Apr 21 27 Apr 21 %Chg. Value Traded (QR mn) 581.0 693.8 (16.3) 10,980 Exch. Market Cap. (QR mn) 632,952.1 634,394.7 (0.2) Volume (mn) 269.9 355.0 (24.0) 10,960 Number of Transactions 10,426 11,390 (8.5) 10,940 Companies Traded 47 48 (2.1) Market Breadth 14:32 21:22 – 10,920 10,900 Market Indices Close 1D% WTD% YTD% TTM P/E Total Return 21,657.54 (0.3) 0.9 7.9 18.6 9:30 10:00 10:30 11:00 11:30 12:00 12:30 13:00 All Share Index 3,454.08 (0.2) 0.7 8.0 19.3 Banks 4,502.33 (0.1) 0.1 6.0 15.8 Industrials 3,664.71 (0.4) 3.6 18.3 29.1 Qatar Commentary Transportation 3,470.53 (0.9) (0.8) 5.3 23.2 The QE Index declined 0.3% to close at 10,940.6. Losses were led by the Real Estate 1,915.97 (0.4) (0.9) (0.7) 18.2 Transportation and Real Estate indices, falling 0.9% and 0.4%, respectively. Top Insurance 2,654.54 0.3 1.5 10.8 25.5 losers were Qatar Cinema & Film Distribution Company and QLM Life & Medical Telecoms 1,094.26 0.1 0.4 8.3 25.0 Insurance Company, falling 9.9% and 2.0%, respectively. Among the top gainers, Consumer 8,374.05 (0.2) (0.6) 2.9 30.1 Mannai Corporation gained 5.4%, while Ahli Bank was up 2.4%. -

SENATE of the FEDERAL REPUBLIC of NIGERIA VOTES and PROCEEDINGS Tuesday, 9Th June, 2015
8TH NATIONAL ASSEMBLY FIRST SESSION No.1 1 SENATE OF THE FEDERAL REPUBLIC OF NIGERIA VOTES AND PROCEEDINGS Tuesday, 9th June, 2015 1. The Senate met at 10: 00 a.m. pursuant to the proclamation by the President of the Federal Republic of Nigeria, Muhammadu Bubari. //·····\;·n~l'. 1r) I" .,"-~~:~;;u~~;~)'::.Y1 PRESIDENT, FEDERAL REPUBLIC OF NIGERIA Your Excellency, PROCLAMATION FOR THE HOLDING OF THE FIRST SESSION OF THE NATIONAL ASSEMBLY WHEREASit is provided in Section 64(3) of the Constitution of the Federal Republic of Nigeria, 1999 (As Amended) that the person Elected as President shall have power to issue a proclamation for the holding of the First Session of the National Assembly immediately after his being sworn-in. NOW,mEREFORE,I Muhammadu Buhari, President, Commander-in-Chief of the Armed Forces of the Federal Republic of Nigeria, in exercise of thepowers bestowed upon me by Section (64) aforesaid, and of all other powers enabling me in that behalf hereby proclaim that the First Session of the eight (8h) National Assembly shall hold at 10.00 a.m. on Tuesday, 9th June, 2015 in the National Assembly, Abuja. Given under my hand and the Public Seal of the Federal Republic of Nigeria at Abuja, this P Day of June, 2015. Yours Sincerely, (Signed) Muhammadu Buhari President, Commander-in-Chief of the Armed Forces Federal Republic of Nigeria 2. At 10.04 a.m. the Clerk to the National Assembly called the Senate to order and informed Senators-Elect that writs had been received in respect of the elections held on 28th March, 2015 in accordance with the Constitution. -

The Falling Netanyahu Takes Down a Cantankerous Political Class
WWW.TEHRANTIMES.COM I N T E R N A T I O N A L D A I L Y 8 Pages Price 50,000 Rials 1.00 EURO 4.00 AED 43rd year No.13954 Saturday MAY 29, 2021 Khordad 8, 1400 Shawwal 17, 1442 Elections is Brighton’s Alireza Steel ingot export Germany recognizes competition to Jahanbakhsh to decide rises 135% in colonial-era massacres in serve people Page 2 on his future Page 3 a month on year Page 4 Namibia as genocide Page 5 Unity is the secret behind the Resistance’s victories: Amir-Abdollahian TEHRAN - Hossein Amir-Abdollahian, the resistance and steadfastness victory could special aide to the speaker of the Iranian be achieved. This victory sent an important Parliament on international affairs, has re- message that the Zionist enemy only under- flected on the secret behind the recent victory stands the language of force and resistance,” of the Palestinian resistance against Israel. he told the Lebanese Al-Ahed News. Amir-Abdollahian said the 2006 victo- The Iranian diplomat added, “This ry of the Lebanese resistance movement victory and other victories achieved by against Israel raised faith in the resistance the resistance, especially the victory of and sent a message that Israel understands July 2006, were achieved in light of the only the language of power. unity of the Lebanese people and the gold- “The flight of the Zionist entity from en equation in Lebanon – the army, the southern Lebanon raised faith in the resist- people, and the resistance. Crabs in ance among the Lebanese, and that through Continued on page 3 Tehran, Moscow confer on joint investment in agricultural sector TEHRAN – Iranian Agriculture Minis- investment in various agricultural fields. -

Smokeless Tobacco and Public Health: a Global Perspective
Chapter 12 Smokeless Tobacco Use in the African Region 353 Blank page. Smokeless Tobacco and Public Health: A Global Perspective Chapter Contents Description of the Region ........................................................................................................................357 Prevalence of Smokeless Tobacco Use....................................................................................................358 Types of Products and Patterns of Use ....................................................................................................362 Toxicity and Nicotine Profiles .................................................................................................................365 Health Problems Associated With Product Use.......................................................................................365 Marketing and Production Practices of Industry .....................................................................................367 Production ..........................................................................................................................................367 Distribution ........................................................................................................................................367 Marketing ...........................................................................................................................................368 Current Policy and Interventions .............................................................................................................369 -

Annual Report (Jan 2011—Mar 2012)
FOOTBALL ASSOCIATION OF SINGAPORE ANNUAL REPORT (JAN 2011—MAR 2012) 30th FAS ANNUAL GENERAL MEETING JALAN BESAR STADIUM 30 JULY 2012 FAS Annual Report (Jan 2011—Mar 2012) CONTENTS Page A. Significant Events 3 B. The Administraon 12 C. Standing Commiees 16 D. Affiliaon / Membership 17 E. S.League Review 22 F. Football Excellence 39 G. Grassroots & Community Outreach 63 H. Compeons 65 I. Referees 69 J. Disciplinary 80 K. Women’s Football 83 L. Medical 87 M. Appendix 91—156 (Full Results of Regional, Internaonal Compeons, Matches & Training Tours and Other Local Compeons) N. Financial Report 157—188 Page 2 F A S A n n u a l R e p o r t ( J a n 2 0 1 1—M a r 2 0 1 2 ) SIGNIFICANT EVENTS 1st January 2011—31st March 2012 INTRODUCTION 2011 marked the second year of the implementaon of the FAS Strategic Plan 2010- 2015, and FAS are pleased to inform members, partners and stakeholders, that together we have made progress in the implementaon of this Plan both on and off-the-field. On the field, our Naonal ‘A’ Team met the target of qualifying for the Third Round of the 2014 FIFA World Cup Asian Qualifiers while our Naonal Youth teams performed well in the 23rd Lion City Cup tournament that was held at the Jalan Besar Stadium in June 2011. Off the field, FAS was recognised by FIFA for its various development programmes and iniaves aimed at taking Singapore football to the next level as envisaged by our FAS Strategic Plan 2010-2015. -

Nnamdi Kanu Leader of the Indigenous People Of
Received by NSD/FARA Registration Unit 05/15/2020 6:30:11 PM April 29, 2020 Hon. David Perdue United States Member of Congress 455 Russell Senate Office Building Washington, DC 20510 Dear Senator Perdue, As concerned citizens, constituents, and members of the Nigerian diaspora in the United States, we write to call your attention to the volatile and violent situation in Nigeria in which minority groups and those with dissenting views, including the Indigenous People of Biafra (IPOB), are being victimized and persecuted with impunity while the Buhari government stands silently by - and in some instances participates. Without urgent attention and the assistance of the international community, conditions will continue to deteriorate, compromising U.S. interests in the region and repeating the atrocities and bloodshed the world has witnessed far too often in this part of the globe. Over the past five years, there has been a sharp increase in criminality and spreading insecurity; widespread failure by the federal authorities to investigate and hold perpetrators accountable, even for mass killings; and a generalized break down of the rule of law. This has been exacerbated by the proliferation of small and military-grade weapons made readily available as a result of regional instability and originating from as far north as the Libyan conflict. Despite this recognized humanitarian crisis, the Nigerian government has increasingly dismissed religious and human rights concerns, and continued to perpetrate violations of its own. There are many documented incidences of violence led by state security actors, but no mechanisms by which to hold the Administration accountable. In its 2018 Nigeria Human Rights Report, the U.S. -

SENATE of the FEDERAL REPUBLIC of NIGERIA ORDER PAPER Thursday, 12Th March, 2020
9TH NATIONAL ASSEMBLY FIRST SESSION NO. 118 437 SENATE OF THE FEDERAL REPUBLIC OF NIGERIA ORDER PAPER Thursday, 12th March, 2020 1. Prayers 2. Approval of the Votes and Proceedings 3. Oaths 4. Announcements (if any) 5. Petitions PRESENTATION OF BILLS 1. Animal Health and Husbandry Technologists Registration Board (Est, etc) Bill, 2020 (HB. 374) - First Reading Sen. Abdullahi, Yahaya Abubakar (Kebbi North-Senate Leader). 2. 1999 Constitution of the Federal Republic of Nigeria (Alteration) Bill, 2020 (SB. 361) - First Reading Sen. Tanimu, Philip Aduda (F.C.T Senate). 3. 1999 Constitution of the Federal Republic of Nigeria (Alteration) Bill, 2020 (SB. 351) - First Reading Sen. Ekwunife, Uche Lilian (Anambra Central). 4. 1999 Constitution of the Federal Republic of Nigeria (Alteration) Bill, 2020 (SB.398) - First Reading Sen. Dahiru, Aishatu Ahmed (Adamawa Central). 5. Open Defecation (Prohibition) Bill, 2020 (SB. 337)- First Reading Sen. Ordia, Akhimienmona Clifford (Edo Central). ORDERS OF THE DAY CONSIDERATION OF BILLS 1. A Bill for an Act to alter the provisions of the Constitution of the Federal Republic of Nigeria, 1999 to provide for the amendment of Sections 65 (2) (a), 131 (d), Section 106 (c) and Section 177 (d) therein, to provide for minimum qualification for election into the National and States Assembly, Office of the President and Governors, and other related matters, 2020 (SB. 75)- Second Reading Sen. Gyang, Istifanus Dung (Plateau North). 2. A BilI for an Act to alter the provisions of the Constitution of the Federal Republic of Nigeria, 1999 to specify the period within which the President or Governor of a State presents the Appropriation Bill before the National Assembly of House of Assembly and for other related matters, 2020 (SB. -

COMPARATIVE POLITICS Directorate Of
COMPARATIVE POLITICS MA [Political Science] Second Semester POLS 802C First Semester II (POLS 702C) [ENGLISH EDITION] Directorate of Distance Education TRIPURA UNIVERSITY Reviewer Dr Nivedita Giri Assistant Professor, Jesus & Mary College, University of Delhi Authors: Dr Saidur Rahman (Unit: 1.2) © Dr. Saidur Rahman, 2016 Dr Biswaranjan Mohanty (Units: 2.2, 3.2, 4.2.2, 4.5) © Dr. Biswaranjan Mohanty, 2016 Dr Jyoti Trehan Sharma and Dr Monica M Nandi (Units: 2.6-2.6.1, 4.6) © Dr Jyoti Trehan Sharma and Dr Monica M Nandi, 2016 Vikas Publishing House (Units: 1.0-1.1, 1.3, 1.4-1.12, 2.0-2.1, 2.2.1, 2.3-2.5, 2.6.2-2.12, 3.0-3.1, 3.3-3.10, 4.0-4.2.1, 4.3-4.4, 4.7-4.11) © Reserved, 2016 Books are developed, printed and published on behalf of Directorate of Distance Education, Tripura University by Vikas Publishing House Pvt. Ltd. All rights reserved. No part of this publication which is material, protected by this copyright notice may not be reproduced or transmitted or utilized or stored in any form of by any means now known or hereinafter invented, electronic, digital or mechanical, including photocopying, scanning, recording or by any information storage or retrieval system, without prior written permission from the DDE, Tripura University & Publisher. Information contained in this book has been published by VIKAS® Publishing House Pvt. Ltd. and has been obtained by its Authors from sources believed to be reliable and are correct to the best of their knowledge. -

Regional Legends Look Forward to First FIFA Arab Cup in Qatar
Sport MONDAY 26 APRIL 2021 ACL:AC Al Duhail coach Lamouchi praises players'pla efforts after Esteghlal draw ItIt mightmigh not have been like the previous one in terms of chances and goals butbut it wasw a big and exciting match. We controlled the match very well and after wew took the lead, I thought that we were going to get the three points. Al Duhail coach Sabri Lamouchi Sport |19 AFC CHAMPIONS LEAGUE: GROUP STAGE Al Rayyan vs FC Goa (8:00pm), Al Sadd vs Foolad (9.00pm), Al Wahda vs Persepolis Draw ceremony to take place at Katara Opera House tomorrow Regional legends look forward Firstly, the Arab Cup will provide the Qatar 2022 organisers with an important final test of stadiums and all the related infrastructure that to first FIFA Arab Cup in Qatar will play a key role in hosting a successful World Cup: THE PENINSULA – DOHA Adel Khamis Egyptian legend Wael Gomaa Qatar will host the FIFA Arab We will have current and Cup later this year, with the draw for the tournament taking former continental champions place at Katara Opera House mixing it up with up-and- tomorrow at 9:00pm. coming teams – it will be an Twenty-three national exciting tournament and one teams will compete for the that shows teams from the trophy, with matches set to be played at six FIFA World Cup Arab region in the best Qatar 2022 venues. The tour- possible light: Former Qatari nament is regarded as a final star Khalid Salman rehearsal for the first World Cup in the Middle East and The Arab Cup will provide yet Arab world, which will take place from 21 November to 18 another important experience December 2022.