6 Chronic Abdominal Pain in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

And Diaphragm (Chilaiditi's Syndrome) in Children by A
Arch Dis Child: first published as 10.1136/adc.32.162.151 on 1 April 1957. Downloaded from INTERPOSITION OF THE COLON BETWEEN LIVER AND DIAPHRAGM (CHILAIDITI'S SYNDROME) IN CHILDREN BY A. D. M. JACKSON and C. J. HODSON From the Institute of Child Health, University ofLondon, and the Queen Elizabeth Hospitalfor Children, London (RECEIVED FOR PUBLICATION SEPTEMBER 24, 1956) In 1910 Chilaiditi published a paper in which he positions. On one occasion during the fluoroscopy the described three adult patients with gaseous ab- ascent of the colon and the displacement of the liver were dominal distension and intermittent displacement actually observed as the patient was rotated from the supine to the left lateral position. Fluoroscopy after an of the liver by a distended loop of colon. Although opaque meal excluded any form of intestinal obstruction there had been some earlier brief reports, for example and the interposed loop of bowel was identified as the those of Gontermann (1890), Cohn (1907) and hepatic flexure. Weinberger (1908), this was the first really detailed PROGRESS. During the six months following his first account of the condition which has come to be visit to hospital the child had recurrent attacks of severe known as Chilaiditi's syndrome. abdominal pain with vomiting and his mother became During the last 45 aware of his swallowing air. He was admitted to hos- years many more cases have copyright. been reported but very few of these have been pital in June, 1951, and put to bed. The attacks promptly children. It will be of some interest, therefore, ceased, although the abdominal distension persisted and the position of the liver could still be altered with posture. -
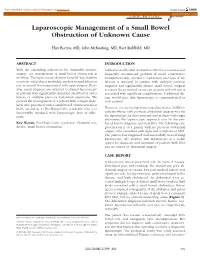
Laparoscopic Management of a Small Bowel Obstruction of Unknown Cause
View metadata, citation and similar papers at core.ac.uk brought to you by CORE CASE REPORT provided by PubMed Central Laparoscopic Management of a Small Bowel Obstruction of Unknown Cause E´lan Burton, MD, John McKeating, MD, Kurt Stahlfeld, MD ABSTRACT INTRODUCTION With the expanding indications for minimally invasive Adhesive small bowel obstruction (SBO) is a common and surgery, the management of small bowel obstruction is frequently encountered problem. If initial conservative evolving. The laparoscope shortens hospital stay, hastens management fails, operative exploration, and lysis of ad- recovery, and reduces morbidity, such as wound infection hesions is required. In patients with multiple previous and incisional hernia associated with open surgery. How- surgeries and significantly dilated small bowel, surgical ever, many surgeons are reluctant to attempt laparoscopy access to the peritoneal cavity can be quite difficult and is in patients with significantly distended small bowel and a associated with significant complications. Traditional dic- history of multiple previous abdominal operations. We tum would state that laparoscopy is contraindicated in present the management of a patient with a virgin abdo- such patients. men who presented with a small bowel obstruction most likely secondary to Fitz-Hugh-Curtis syndrome who was However, we are seeing an increased incidence of SBO in successfully managed with laparoscopic lysis of adhe- patients whose only previous abdominal surgery was via sions. the laparoscope. In these patients, and in those with virgin abdomens, the laparoscopic approach may be the pre- Key Words: Fitz-Hugh-Curtis syndrome, Chilaiditi syn- ferred way to diagnose and treat SBO. The following case drome, Small bowel obstruction. -

Chilaiditi's Syndrome Complicated by Colon Perforation
CASE REPORT Chilaiditi’s syndrome complicated by colon perforation: a case report Turan Acar, M.D., Erdinç Kamer, M.D., Nihan Acar, M.D., Ahmet Er, M.D., Mustafa Peşkersoy, M.D. Department of Surgery, Izmir Katip Celebi University Ataturk Training and Research Hospital, Izmir ABSTRACT Hepatodiaphragmatic interposition of the small or large intestine is known as Chilaiditi syndrome, whichis a rare disease diagnosed incidentally. Chilaiditi syndrome is typically asymptomatic, but it can be associated with symptoms ranging from intermittent, mild ab- dominal pain to acute intestinal obstruction, constipation, chest pain and breathlessness. A 54-year-old male patient was admitted to the hospital with a history of abdominal pain, nausea and vomiting. Chest X-ray revealed an elevation of the right hemidiaphragma caused by the presence of a dilated colonic loop below. The patient underwent urgent surgery with perforation as preliminary diagnosis. The pa- tient underwent right hemicolectomy and ileocolic anastomosis because of the intestinal obstruction related to Chilaiditi’s Syndrome. Due to the rarity of this syndrome and typical radiological findings, this case was aimed to be presented. Key words: Abdominal pain; Chilaiditi’s syndrome; surgery. INTRODUCTION CASE REPORT Interposition of the bowel (usually transverse colon or he- A 54-year-oldmale patient was admitted to the Emergency patic flexura) or the small intestine between the liver and Department of Surgery, Izmir Katip Celebi University Ataturk diaphragm, which is a rare anomaly, was first defined by the Training and Research Hospital with a 24-hour history of right Greek radiologist Demetrius Chilaiditi in 1910.[1,2] It is inci- upper abdominal pain, nausea and vomiting. -

En 17-Chilaiditi™S Syndrome.P65
Nagem RG et al. SíndromeRELATO de Chilaiditi: DE CASO relato • CASE de caso REPORT Síndrome de Chilaiditi: relato de caso* Chilaiditi’s syndrome: a case report Rachid Guimarães Nagem1, Henrique Leite Freitas2 Resumo Os autores apresentam um caso de síndrome de Chilaiditi em uma mulher de 56 anos de idade. Mesmo tratando-se de condição benigna com rara indicação cirúrgica, reveste-se de grande importância pela implicação de urgência operatória que representa o diagnóstico equivocado de pneumoperitônio nesses pacientes. É realizada revisão da li- teratura, com ênfase na fisiopatologia, propedêutica e tratamento desta entidade. Unitermos: Síndrome de Chilaiditi; Sinal de Chilaiditi; Abdome agudo; Pneumoperitônio; Espaço hepatodiafragmático. Abstract The authors report a case of Chilaiditi’s syndrome in a 56-year-old woman. Although this is a benign condition with rare surgical indication, it has great importance for implying surgical emergency in cases where such condition is equivocally diagnosed as pneumoperitoneum. A literature review is performed with emphasis on pathophysiology, diagnostic work- up and treatment of this entity. Keywords: Chilaiditi’s syndrome; Chilaiditi’s sign; Acute abdomen; Pneumoperitoneum; Hepatodiaphragmatic space. Nagem RG, Freitas HL. Síndrome de Chilaiditi: relato de caso. Radiol Bras. 2011 Set/Out;44(5):333–335. INTRODUÇÃO RELATO DO CASO tricos, com pressão arterial de 130 × 90 mmHg. Abdome tenso, doloroso, sem irri- Denomina-se síndrome de Chilaiditi a Paciente do sexo feminino, 56 anos de tação peritoneal, com ruídos hidroaéreos interposição temporária ou permanente do idade, foi admitida na unidade de atendi- preservados. De imediato, foram solicita- cólon ou intestino delgado no espaço he- mento imediato com quadro de dor abdo- dos os seguintes exames: amilase: 94; PCR: patodiafragmático, causando sintomas. -

Dientamoeba Fragilis – the Most Common Intestinal Protozoan in the Helsinki Metropolitan Area, Finland, 2007 to 2017
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Helsingin yliopiston digitaalinen arkisto Research Dientamoeba fragilis – the most common intestinal protozoan in the Helsinki Metropolitan Area, Finland, 2007 to 2017 Jukka-Pekka Pietilä1, Taru Meri2, Heli Siikamäki1, Elisabet Tyyni3, Anne-Marie Kerttula3, Laura Pakarinen1, T Sakari Jokiranta4,5, Anu Kantele1,6 1. Inflammation Center, Infectious Diseases, Helsinki University Hospital and Helsinki University, Helsinki, Finland 2. Molecular and Integrative Biosciences Research Programme, Faculty of Biological and Environmental Sciences, University of Helsinki, Helsinki, Finland 3. Division of Clinical Microbiology, Helsinki University Hospital, HUSLAB, Helsinki, Finland 4. Medicum, University of Helsinki, Finland 5. SYNLAB Finland, Helsinki, Finland 6. Human Microbiome Research Program, Faculty of Medicine, University of Helsinki, Finland Correspondence: Anu Kantele ([email protected]) Citation style for this article: Pietilä Jukka-Pekka, Meri Taru, Siikamäki Heli, Tyyni Elisabet, Kerttula Anne-Marie, Pakarinen Laura, Jokiranta T Sakari, Kantele Anu. Dientamoeba fragilis – the most common intestinal protozoan in the Helsinki Metropolitan Area, Finland, 2007 to 2017. Euro Surveill. 2019;24(29):pii=1800546. https://doi.org/10.2807/1560- 7917.ES.2019.24.29.1800546 Article submitted on 08 Oct 2018 / accepted on 12 Apr 2019 / published on 18 Jul 2019 Background: Despite the global distribution of of Dientamoeba-like structures in formalin-fixed sam- the intestinal protozoan Dientamoeba fragilis, its ples, an approach applicable also in resource-poor clinical picture remains unclear. This results from settings. Symptoms of dientamoebiasis differ slightly underdiagnosis: microscopic screening methods from those of giardiasis; patients with distressing either lack sensitivity (wet preparation) or fail to symptoms require treatment. -

Ext Name Div Room Ext Name Div Room ______
EXT NAME DIV ROOM EXT NAME DIV ROOM __________________________________________________________________________________________________________________________ A 56407 ALUNG, Ashok CSAP D170 52673 ALVETRETI, Letizia CSPL D328 54157 ABABOUCH, Lahsen FIPX F405 54458 AMADO, Maria Blanca TCIB D503 55581 ABALSAMO, Stefania CIOO F713 53290 AMARAL, Cristina TCE C744 53264 ABBASSIAN, Abdolreza ESTD D804 55126 AMBROSIANO, Luciana AGDF C292 54511 ABBONDANZA, Carla CPA A143B 1709 AMEGEE, Emilienne CSSD SSC 52390 ABDELLA, Yesuf TCIA D557 56437 AMICI, Paolo ESSD C456 55396 ABDIRIZZAK, Tania FOED C474 53985 AMMATI, Mohammed AGPM B752 53485 ABE, Kaori TCE C751 54876 AMOROSO, Leslie ESN C214 54315 ABI NASSIF, Joseph CSDM B104 56891 AMROUK, El Mamoun ESTD D866 53963 ABI RACHED, Elie CPAM A281 53980 ANAMAN, Frederick CIOF B239 55087 ABITBOL, Nathalie TCIA D556 54213 ANAND, Sanjeev TCSD D611 56584 ABOU-RIZK, Margaret LEGP D371 53309 ANDARIAS DE PRADO, Rebeca CSAI D102 1716 ABRAHAM, Erika CSSD SSC 1725 ANDONOVSKA, Liljana CSSD SSC 56202 ABRAMO-GUARNA, Anna TCIA D554 53602 ANDRADE CIANFRINI, Graciela FOMD D468 55375 ABRAMOVA, Olga OSD D728 55742 ANELLO, Enrico OEKM C102 54178 ABRAMOVICI, Pierre CIOH C130 54441 ANGELINI, Chiara CPAP A487 56760 ABREU, Maria LEGD A442 54109 ANGELINI, Flavio CSAI D114 53296 ABRINA, Angelica Gavina OSPD B449 55313 ANGELONI, Marino CSAI D103 52709 ACCARDO-DELHOME, Jeanne FODP D435 53145 ANGELOZZI, Vanessa CSDU A042 53843 ACHOURI, Moujahed NRL B732 53720 ANGELUCCI, Federica ESTD D863 52294 ACOSTA, Natalia OEDD B452 52677 ANIBALDI, -

Case Study of 100 Cases of Intestinal Obstruction
CASE STUDY OF 100 CASES OF INTESTINAL OBSTRUCTION Dissertation submitted in partial fulfillment of the Requirement for the award of the degree of MS DEGREE EXAMINATION GENERAL SURGERY TIRUNELVELI TIRUNELVELI MEDICAL COLLEGE THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY CHENNAI,TAMILNADU APRIL 2013 CERTIFICATE This is to certify that the dissertation titled “CASE STUDY OF 100 CASES OF INTESTINAL OBSTRUCTION “ is the original work done by DR.VARGHESE THOMAS,post graduate in Dept. Of General Surgery,Tirunelveli medical college,to be submitted to the TAMIL NADUDr.MGR Medical University Chennai-32 towards the partial fulfillment of the requirement for the award of MS Degree in General Surgery, April 2013. Prof.Dr.S.Soundararajan MS Dr.M.Manoharan MS Unit Chief Professor & The DEAN Head Of Department Tirunelveli Medical College Department of General Surgery Tirunelveli Tirunelveli Medical College Tirunelveli ii ACKNOWLEDGEMENT It is a great pleasure to express my deep sense of gratitude and heartfelt thanks to My beloved teacher and guide, Dr.S.Soundararajan MS Prof & HOD Dept. of General Surgery, Tirunelveli medical college. For his patient guidance, constant inspiration, scholarly suggestions, timely advice and encouragement in my tenure as a postgraduate. I am extremely grateful to Dr.Maheswari MS, Dr. Pandy MS, Dr.Varadharajan MS. Dr.Alex Edward MS, Dr.Sreethar MS, Dr.Manoharan MS, for their profound knowledge, encouragement and guidance during the study period. I am extremely grateful to my Assistant Professors, Dr.Raju MS and Dr.Rajkumar MS for their constant inspiration, invaluable guidance, constant supervision and timely advice in preparing this dissertation and also in my tenure as a postgraduate. -

Original Article Dientamoeba Fragilis Diagnosis by Fecal Screening
Original Article Dientamoeba fragilis diagnosis by fecal screening: relative effectiveness of traditional techniques and molecular methods Negin Hamidi1, Ahmad Reza Meamar1, Lameh Akhlaghi1, Zahra Rampisheh2,3, Elham Razmjou1 1 Department of Medical Parasitology and Mycology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran 2 Preventive Medicine and Public Health Research Center, Iran University of Medical Sciences, Tehran, Iran 3 Department of Community Medicine, School of Medicine, Iran University of Medical Sciences, Tehran, Iran Abstract Introduction: Dientamoeba fragilis, an intestinal trichomonad, occurs in humans with and without gastrointestinal symptoms. Its presence was investigated in individuals referred to Milad Hospital, Tehran. Methodology: In a cross-sectional study, three time-separated fecal samples were collected from 200 participants from March through June 2011. Specimens were examined using traditional techniques for detecting D. fragilis and other gastrointestinal parasites: direct smear, culture, formalin-ether concentration, and iron-hematoxylin staining. The presence of D. fragilis was determined using PCR assays targeting 5.8S rRNA or small subunit ribosomal RNA. Results: Dientamoeba fragilis, Blastocystis sp., Giardia lamblia, Entamoeba coli, and Iodamoeba butschlii were detected by one or more traditional and molecular methods, with an overall prevalence of 56.5%. Dientamoeba was not detected by direct smear or formalin-ether concentration but was identified in 1% and 5% of cases by culture and iron-hematoxylin staining, respectively. PCR amplification of SSU rRNA and 5.8S rRNA genes diagnosed D. fragilis in 6% and 13.5%, respectively. Prevalence of D. fragilis was unrelated to participant gender, age, or gastrointestinal symptoms. Conclusions: This is the first report of molecular assays to screen for D. -
Clinical Appendix for Parasitic Diseases Seventh Edition
Clincal Appendix for the Seventh Edition Parasitic Diseases Despommier Griffin Gwadz Hotez Knirsch Parasites Without Borders, Inc. NY Dickson D. Despommier, Daniel O. Griffin, Robert W. Gwadz, Peter J. Hotez, Charles A. Knirsch Clinical Appendix for Parasitic Diseases Seventh Edition see full text of Parasitic Diseases Seventh Edition for references Parasites Without Borders, Inc. NY The organization and numbering of the sections of the clinical appendix is based on the full text of the seventh edition of Parasitic Diseases. Dickson D. Despommier, Ph.D. Professor Emeritus of Public Health (Parasitology) and Microbiology, The Joseph L. Mailman School of Public Health, Columbia University in the City of New York 10032, Adjunct Professor, Fordham University Daniel O. Griffin, M.D., Ph.D. CTropMed® ISTM CTH© Department of Medicine-Division of Infectious Diseases, Department of Biochemistry and Molecular Biophysics, Columbia University Vagelos College of Physicians and Surgeons, Columbia University Irving Medical Center New York, New York, NY 10032, ProHealth Care, Plainview, NY 11803. Robert W. Gwadz, Ph.D. Captain USPHS (ret), Visiting Professor, Collegium Medicum, The Jagiellonian University, Krakow, Poland, Fellow of the Hebrew University of Jerusalem, Fellow of the Ain Shams University, Cairo, Egypt, Chevalier of the Nation, Republic of Mali Peter J. Hotez, M.D., Ph.D., FASTMH, FAAP, Dean, National School of Tropical Medicine, Professor, Pediatrics and Molecular Virology & Microbiology, Baylor College of Medicine, Texas Children’s Hospital Endowed Chair of Tropical Pediatrics, Co-Director, Texas Children’s Hospital Center for Vaccine Development, Baker Institute Fellow in Disease and Poverty, Rice University, University Professor, Baylor University, former United States Science Envoy Charles A. -

BBO User Names ~ Sorted by BBO User Name
BBO User Names ~ Sorted by BBO User Name BPM BBO User Date User Name Last Name (1) First Name (2) Game Level Name Added Sutton Patricia 1108820 05/29/20 Beattie Laurie 2006898 05/26/20 Chrisman Roger 3338231 05/21/20 Stryker Mona 00monabs 06/15/20 Cole Jean 101rye 06/13/20 Ross Mary 1038mary 06/10/20 Barsodi Jacqueline 168bar 04/11/20 Moore Tom 1947Deacon 04/04/20 Glaze Brenda 1954queen 06/01/20 Smith Jinny 1986north 299er 03/31/20 Robinson Blair 1Blair1 05/13/20 Drake Kathleen 1sK90b8c0 05/10/20 LaMothe Ribs 1spareribs Open 03/23/20 Herman Linda 1TBCLinda 05/22/20 Hammond Myra 2012ariel 299er/Open 03/26/20 LaCava Frank 3frankl 299er/Open 03/18/20 Layton Mike 44mybaby 05/24/20 Layton Dee 46Granny 05/24/20 Reese Sherre 57 Ransom 05/27/20 Martin Mary Ellen 7215mar 5er 06/10/20 Howard Mike 76howard 05/30/20 Fortado Avis aaf8844 Open 03/27/20 Nason Scott AAFlyer Open 03/23/20 Sterrantino Cyndy abbiy 99er 03/31/20 Cardinal Alain ac_idic 04/29/20 Sax Robbie Ace1795 05/16/20 Bralower Meryl Acksba 04/16/20 Ackerman Steven acksteveni 06/23/20 Curti Anne acurt 05/26/20 Downing Amy Adowning Open 06/06/20 Wiles Alex afwprivate 04/27/20 Ruhe Mary agildog 04/07/20 Batchelder Ann ahb808 07/07/20 Aide Barbara aidesifuen Open 03/19/20 Bricker Diane Air51 07/07/20 McKee Jeff akjxxx 06/09/20 Ludwig Alan al1942 07/06/20 Murdoch Joan albany2020 04/16/20 DeLaRosa Anne ALD8 49er 04/05/20 Compton Morgan alexis95 49er 03/19/20 Parmelee Carolyn Algona 05/22/20 Pharr Susan allisonp 299er 03/28/20 Hatch Deanna AlyceJake 04/21/20 Mason Annie amasonid 04/10/20 Flank -

Chilaiditi's Sign and the Acute Abdomen
ACS Case Reviews in Surgery Vol. 3, No. 2 Chilaiditi’s Sign and the Acute Abdomen AUTHORS: CORRESPONDENCE AUTHOR: AUTHOR AFFILIATION: Devecki K; Raygor D; Awad ZT; Puri R Ruchir Puri, MD, MS, FACS University of Florida College of Medicine, University of Florida College of Medicine Department of Surgery, Department of General Surgery Jacksonville, FL 32209 653 W. 8th Street Jacksonville, FL 32209 Phone: (904) 244-5502 E-mail: [email protected] Background Chilaiditi’s sign is a rare radiologic sign where the colon or small intestine is interposed between the liver and the diaphragm. Chilaiditi’s sign can be mistaken for pneumoperitoneum and can be alarming in the setting of an acute abdomen. Summary We present two cases of Chilaiditi’s sign resulting from vastly different pathologies. The first patient was a 67-year-old male who presented with right upper quadrant pain. He was found to have Chilaiditi’s sign on the upright chest X ray. A CT scan revealed a cecal bascule interposed between the liver and diaphragm with concomitant acute appendicitis. Diagnostic laparoscopy confirmed imaging findings, and he underwent an open right hemicolectomy. The second patient was a 59-year-old female who presented with acute onset of right-sided abdominal pain. An upright chest X ray revealed air under the right hemidiaphragm, and the CT scan demonstrated a large, right-sided Morgagni-type diaphragmatic hernia. She underwent an elective laparoscopic hernia repair, which confirmed the presence of an anteromedial diaphragmatic hernia containing small bowel, colon, and omentum. Conclusion Chilaiditi’s sign can be associated with an acute abdomen. -

Company Name First Name Last Name Job Title Country
Company Name First Name Last Name Job Title Country 1StopWind Ltd Arran Bell Operations Manager United Kingdom 1StopWind Ltd. Alan Mckerns United Kingdom 1StopWind Ltd. Bernadette McAulay Finance Manager United Kingdom 1StopWind Ltd. Joel Telling General Manager United Kingdom 23 Degrees Renewables Ltd Ed Woodrow Business Development United Kingdom 24SEA bvba Gert De Sitter Owner Belgium 3S Europe GmbH Matthias Lamp Vice President of Sales & Marketing Germany 3sun Denmark ApS Christian Christensen Operations Director Denmark 3sun Group Limited Jody Potter United Kingdom 3sun Group Limited Graham Hacon VP Business Development, Offshore Wind United Kingdom 3sun Group Limited Sherri Smith Company Secretary United Kingdom 3W Industri Service Simon Øland Project manager - sales Denmark 3W Industri Service Kenneth Pedersen IWI-S Denmark 4C Offshore Lauren Anderson United Kingdom 4C Offshore Richard Aukland Director United Kingdom 4C Offshore Rosie Haworth Market Researcher United Kingdom 4C Offshore Vincenzo Poidomani Principal Geotechnical Engineer United Kingdom 8.2 Bruno ALLAIN CEO France 8.2 Monitoring GmbH Bernd Höring Managing director Germany 920338402 Ellinor Meling Ceo Norway A&P Group Emma Harrick United Kingdom A.P. Møller Holding Simon Ibsen Investor Denmark A/S Dan-Bunkering Ltd. Jens Kirk Denmark A/S Dan-Bunkering Ltd. Michael Brunø-Sørensen Senior Bunker Trader Denmark A1wind Aps Martin Jensen Director / A1wind Aps Denmark AAF Ltd Steven Brett Europe MFAS Aftermarket Sales Manager United Kingdom AAG Allan Tarp Sales Manager Denmark