Sudan University of Science and Technology College of $Edical Radiologicjfciences Department of Piagiiosticpechnology Project Ti
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Skeleton of the Upper Limb
SKELETON OF THE UPPER LIMB L E C T U R E 2 D E N T I S T R Y 2016 RNDR. MICHAELA RAČANSKÁ, PH.D. Skeleton of the upper limb (ossa membri superioris) Thirty-four bones form the skeletal framework of each upper limb I. Shoulder girdle (cingulum membri superioris) Collar bone, clavicle – clavicula Shoulder blade – scapula II. Bones of free part of the upper limb (ossa membri superioris liberi) Arm bone – humerus Radius – radius Ulna – ulna Carpal bones – ossa carpi 8 Metacarpal bones – ossa metacarpi 5 Phalanges, hand digits – ossa digitorum manus 14 Sesamoid - 2 Clavicula (collar bone) Connects upper limb with the trunk Connection with the shoulder blade Connection with the breast bone Clavicula (collar bone) Medial end (sternal end) extremitas sternalis (facies articularis sternalis) sternal articular facet tuberositas costalis Costal tuberosity (impressio ligamenti costoclavicularis) (impression for costoclavicular ligament) Lateral (acromial) end extremitas acromialis (facies articularis acromialis) tuberositas coracoidea (tuberculum conoideum et linea trapezoidea) conoid tubercle + trapezoid line Side orientation Left one –superior view Left one –inferior view Fracture of the collar bone X-ray of a left clavicle fracture https://en.wikipedia.org/wiki/Clavicle_fracture Scapula Connection to humerus, clavicle Margo: superior medialis lateralis angulus: superior, inferior, lateralis facies: costalis, dorsalis Facies costalis scapulae Lineae musculares (transverae) Fossa subscapularis Incisura scapulae (ligamentum transversum scapulae) Processus -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Applied Anatomy of the Shoulder Girdle
Applied anatomy of the shoulder girdle CHAPTER CONTENTS intra-articular disc, which is sometimes incomplete (menis- Osteoligamentous structures . e66 coid) and is subject to early degeneration. The joint line runs obliquely, from craniolateral to caudomedial (Fig. 2). Acromioclavicular joint . e66 Extra-articular ligaments are important for the stability of Sternoclavicular joint . e66 the joint and to keep the movements of the lateral end of the Scapulothoracic gliding mechanism . e67 clavicle within a certain range. Together they form the roof of Costovertebral joints . e68 the shoulder joint (see Standring, Fig. 46.14). They are the coracoacromial ligament – between the lateral border of the Muscles and their innervation . e69 coracoid process and the acromion – and the coracoclavicular Anterior aspect of the shoulder girdle . e69 ligament. The latter consists of: Posterior aspect of the shoulder girdle . e69 • The trapezoid ligament which runs from the medial Mobility of the shoulder girdle . e70 border of the coracoid process to the trapezoid line at the inferior part of the lateral end of the clavicle. The shoulder girdle forms the connection between the spine, • The conoid ligament which is spanned between the base the thorax and the upper limb. It contains three primary artic- of the coracoid process and the conoid tubercle just ulations, all directly related to the scapula: the acromioclavicu- medial to the trapezoid line. lar joint, the sternoclavicular joint and the scapulothoracic Movements in the acromioclavicular joint are directly related gliding surface (see Putz, Fig. 289). The shoulder girdle acts as to those in the sternoclavicular joint and those of the scapula. a unit: it cannot be functionally separated from the secondary This joint is also discussed inthe online chapter Applied articulations, i.e. -
Upper Limb Lecture One
Upper limb Lecture one Dr Amal Albtoosh LECTURE TOPIC NUMBER 1 Introduction, Bones of the shoulder and arm, forearm, hand 2 Fascial planes and muscles 3 brachial Plexus What is the limb? • Limb: a leg or arm of a human being The upper limb is a multijointed lever that is freely PROXIMAL movable on the trunk at the shoulder joint. At the distal end of the upper limb is the important organ, the hand. DISTAL Scapula: flat bone inverted triangle 3 borders Superior border medial border lateral border 3 angles superiomedial angle Superiolateral angle Inferior angle 3 Fossae supraspinous fossa infraspinous fossa Subscapular fossa 3 processes spine Acromion coracoid 2 surfaces anterior posterior The superior border has a Suprascapular notch the lateral border has the glenoid cavity above the cavity - supra- glenoid tubercle below it infra-glenoid tubercle Clavicle The clavicle is the only long bone that lies in a horizontal position in the body The clavicle has three regions: the medial end: sternal end of the clavicle the lateral end: acromial end of the clavicleIt also serves as an attachment point for two ligaments: Conoid tubercle – attachment point of the conoid ligament, the medial part of the coracoclavicular ligament. Trapezoid line – attachment point of the trapezoid ligament, the lateral part of the coracoclavicular ligament. and the shaft: acts as a point of attachment for several muscles – deltoid, trapezius, Subclavius, Pectoralis major, sternocleidomastoid and sternhyoid The humerus is the longest bone of the arm and is characterized by many distinct features that help to allow the upper extremity to move through a significant range of motion The following landmarks are found on the humerus: Head. -

Research Article Variability of Length and Osteometrical Study of Human
Scholars Academic Journal of Biosciences (SAJB) ISSN 2321-6883 (Online) Sch. Acad. J. Biosci., 2015; 3(9):814-820 ISSN 2347-9515 (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Research Article Variability of length and Osteometrical study of human clavicle and its applied importance Dr. Gopalakrishna. K1*, Dr. BS. Rathna2 1Assistant Professor, Department of Anatomy, Malabar Medical College and Research Centre, Modakkallur, Atholi, Calicut- 673315. Kerala, India. 2Professor and Head, Department of anatomy, Malabar Medical College and Research Centre, Modakkallur, Atholi, Calicut- 673315. Kerala, India. *Corresponding author Dr. Gopalakrishna. K Email: [email protected] Abstract: To determine the bilateral variability in length of clavicle bones, its relationship with location of nutrient foramen and clavicular Osteometry and its applied importance. Length of clavicle differs with gender, population or race. The length has correlation with its Osteometry. It is essential for clavicular surgeries, designing or selecting the clavicular implants, sex determination in forensic science, anthropology and anatomy. This study was done on 120 dry clavicles (n=120) to determine the bilateral variability in length, correlation between location of nutrient foramen and length and to get data set of clavicular Osteometry of Indian population. ANOVA, correlation-regression analysis and descriptive statistics were done on the collected data. Mean length of clavicles in groups on right side, left side and of both sided was 138.99±5.006mm, 142.618±4.48mm and 140.685±4.88mm respectively. Significant difference was found between right and left side groups. Significant and Strong positive correlation was observed [r=0.9445 on right side and r=0.9654 on left side] between location of nutrient foramen and length. -

Anatomy, Shoulder and Upper Limb, Clavicle - Statpearls - NCBI Bookshelf
12/17/2018 Anatomy, Shoulder and Upper Limb, Clavicle - StatPearls - NCBI Bookshelf NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Shoulder and Upper Limb, Clavicle Authors Scott Hyland1; Matthew Varacallo2. Affilations 1 Edward Via College of OM Virginia 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: October 27, 2018. Introduction The clavicle is a sigmoidshaped long bone with a convex surface along its medial end when observed from cephalad position. It serves as a connection between the axial and appendicular skeleton in conjunction with the scapula, and each of these structures forms the pectoral girdle.[1] Though not as large as other supporting structures in the body, clavicular attachments allow for significant function and range of motion of the upper extremity as well as protection of neurovascular structures posteriorly. Each part of this long bone has a purpose in regards to its attachments that affects the overall physiology of the pectoral girdle. Medially, the clavicle articulates with the manubrial portion of the sternum, forming the sternoclavicular joint (SC joint). This joint, surrounded by a fibrous capsule, contains an intraarticular disc in between the clavicle and the sternum. Superiorly, the interclavicular ligament connects the ipsilateral and contralateral clavicle, together providing further stability.[2] Laterally, the clavicle articulates with the acromion, forming the acromioclavicular ligament (AC joint). The surrounding area provides an attachment for the joint capsule of the shoulder. This joint, like the SC joint, is also lined by fibrocartilage and contains an intraarticular disc. -

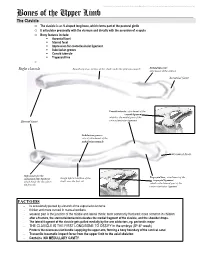
The Clavicle
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. The Clavicle o The clavicle is an S-shaped long bone, which forms part of the pectoral girdle o It articulates proximally with the sternum and distally with the acromion of scapula o Bony features include: . Acromial facet . Sternal facet . Impression for costoclavicular ligament . Subclavian groove . Conoid tubercle . Trapezoid line o Right clavicle Smooth superior surface of the shaft, under the platysma muscle Deltoid tubercle: attachment of the deltoid Acromial facet Conoid tubercle, attachment of the conoid ligament which is the medial part of the Sternal facet coracoclavicular ligament Subclavian groove: site of attachment of the subclavius muscle Acromial facet Impression for the Trapezoid line, attachment of the costoclavicular ligament Rough inferior surface of the trapezoid ligament which binds the clavicle to shaft, over the first rib which is the lateral part of the the first rib coracoclavicular ligament FACTOIDS - Its occasionally pierced by a branch of the supraclavicular nerve - thicker and more curved in manual workers - weakest part is the junction of the middle and lateral thirds: most commonly fractured; more common in children - after a fracture, the sternocleidomastoid elevates the medial fragment of the clavicle, and the shoulder drops. - The lateral fragment of the clavicle gets pulled medially by the arm adductors, eg. pectoralis major - THE CLAVICLE IS THE FIRST LONG BONE TO OSSIFY in the embryo (5th-6th week) - Protects the neurovascular bundle supplying the upper arm, forming a bony boundary of the cervical canal - Transmits traumatic impact force from the upper limb to the axial skeleton - Contains NO MEDULLARY CAVITY - . -
Bones of the Upper Limb
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Bones of the Upper Limb The Clavicle o The clavicle is an S-shaped long bone, which forms part of the pectoral girdle o It articulates proximally with the sternum and distally with the acromion of scapula o Bony features include: . Acromial facet . Sternal facet . Impression for costoclavicular ligament . Subclavian groove . Conoid tubercle . Trapezoid line o Right clavicle Smooth superior surface of the shaft, under the platysma muscle Deltoid tubercle: attachment of the deltoid Acromial facet Conoid tubercle, attachment of the conoid ligament which is the medial part of the Sternal facet coracoclavicular ligament Subclavian groove: site of attachment of the subclavius muscle Acromial facet Impression for the Trapezoid line, attachment of the costoclavicular ligament Rough inferior surface of the trapezoid ligament which binds the clavicle to shaft, over the first rib which is the lateral part of the the first rib coracoclavicular ligament FACTOIDS - Its occasionally pierced by a branch of the supraclavicular nerve - thicker and more curved in manual workers - weakest part is the junction of the middle and lateral thirds: most commonly fractured; more common in children - after a fracture, the sternocleidomastoid elevates the medial fragment of the clavicle, and the shoulder drops. - The lateral fragment of the clavicle gets pulled medially by the arm adductors, eg. pectoralis major - THE CLAVICLE IS THE FIRST LONG BONE TO OSSIFY in the embryo (5th-6th week) - Protects the neurovascular bundle supplying the upper arm, forming a bony boundary of the cervical canal - Transmits traumatic impact force from the upper limb to the axial skeleton - Contains NO MEDULLARY CAVITY - This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. -

Anatomy Lab: the Skeletal System Part I: Vertebrae and Thoracic Cage
ANA Lab: Bone 1 Anatomy Lab: The skeletal system Part I: Vertebrae and Thoracic cage Spine (Vertebrae) Body Vertebral arch Vertebral canal Pedicle Lamina Spinous process Transverse process Sup. articular facets Inf. articular facets Sup. vertebral notch Inf. vertebral notch Intervertebral foramen Cervical vertebrae: 7 Typical (C3-C6) Transverse foramen C1, Atlas C2, Axis: dens C7 Thoracic vertebrae: 12 Typical (T2-T10) T1 T11, 12 Lumbar vertebrae: 5 Typical (L1-4) Sacrum: 5 Ala Anterior sacral foramina Posterior sacral foramina Sacral canal ANA Lab: Bone 2 Sacral hiatus promontory median sacral crest intermediate crest lateral crest Coccyx Horns Transverse process Thoracic cages Ribs: 12 pairs Typical ribs (R3-R10): Head, 2 facets intermediate crest neck tubercle angle costal cartilage costal groove R1 R2 R11,12 Sternum Manubrium of sternum Clavicular notch for sternoclavicular joint body xiphoid process ANA Lab: Bone 3 Part II: Skull and Facial skeleton Skull Cranial skeleton, Calvaria (neurocranium) Facial skeleton (viscerocranium) Overview: identify the margin of each bone Cranial skeleton 1. Lateral view Frontal Temporal Parietal Occipital 2. Cranial base midline: Ethmoid, Sphenoid, Occipital bilateral: Temporal Viscerocranium 1. Anterior view Ethmoid, Vomer, Mandible Maxilla, Zygoma, Nasal, Lacrimal, Inferior nasal chonae, Palatine 2. Inferior view Palatine, Maxilla, Zygoma Sutures: external view vs. internal view Coronal suture Sagittal suture Lambdoid suture External appearance of skull Posterior view external occipital protuberance -

Bones, Part 1: the Appendicular Skeleton
PowerPoint® Lecture Slides The Appendicular Skeleton prepared by Leslie Hendon University of Alabama, Birmingham • Pectoral girdle • Attaches the upper limbs to the trunk Pelvic girdle C H A P T E R • 8 • Attaches the lower limbs to the trunk Part 1 • Upper and lower limbs differ in function Bones, • Share the same structural plan Part 1: The Appendicular Skeleton Copyright © 2011 Pearson Education, Inc. Copyright © 2011 Pearson Education, Inc. The Pectoral Girdle The Pectoral Girdle • Consists of the clavicle and the scapula • Provides attachment for many muscles that • Pectoral girdles do not quite encircle the move the upper limb body completely • Girdle is very light and upper limbs are • Medial end of each clavicle articulates with mobile the manubrium and first rib • Only clavicle articulates with the axial skeleton • Laterally—the ends of the clavicles join the • Socket of the shoulder joint (glenoid cavity) is scapulae shallow • Scapulae do not join each other or the axial • Good for flexibility, bad for stability skeleton Copyright © 2011 Pearson Education, Inc. Copyright © 2011 Pearson Education, Inc. Articulated Pectoral Girdle Clavicles Sternal (medial) Clavicle end Acromio- clavicular Scapula Posterior joint Anterior Acromial (lateral) end (b) Right clavicle, superior view Acromial end Anterior Trapezoid line Sternal end Posterior Tuberosity for PLAY Shoulder Conoid tubercle costoclavicular ligament (a) Articulated pectoral girdle (c) Right clavicle, inferior view Copyright © 2011 Pearson Education, Inc. Figure 8.1a Copyright © 2011 Pearson Education, Inc. Figure 8.1b, c 1 Scapulae Structures of the Scapula Acromion Suprascapular notch Superior border • Lie on the dorsal surface of the rib cage Coracoid Superior process angle • Located between ribs 2–7 Glenoid cavity • Have three borders • Superior • Medial (vertebral) • Lateral (axillary) Subscapular Lateral border fossa • Have three angles Medial border • Lateral, superior, and inferior (a) Right scapula, anterior aspect Inferior angle Copyright © 2011 Pearson Education, Inc. -

Upper Extremities
Bones I. Sternum (G. sternon, the chest) A. Manubrium (L. handle) attachments - pectoralis major m. 1. Clavicular notch (L. clavicula, small key) function - articulates with clavicle 2. Jugular notch (L. jugulm, throat) B. Body attachments - pectoralis major m. C. Xiphoid process (G. xiphos, sword) II. Clavicle A. Acromial end (G. akromion, tip + osmos, shoulder) function - articulates with acromion B. Sternal end function - articulates with sternum C. Superior surface attachments - sternocleidomastoid muscle m. D. Inferior surface 1. Conoid tubercle (cone shaped; L. tuber, swelling) attachments - conoid lig. 2. Trapezoid line attachments - trapezoid lig. E. Anterior border attachments - pectoralis major & deltoid m. F. Posterior border attachments - trapezius m. III. Scapula A. Borders 1. Medial attachments - rhomboids & serratus anterior m. 2. Superior attachments - omohyoid m. & transverse scapular lig. a. Suprascapular notch (indentation at the edge of a bone) function - transmits suprascapular n. 3. Lateral attachments - teres minor m. B. Angles 1. Superior attachments - levator scapulae m. 2. Inferior attachments - teres major m. 3. Lateral C. Fossa (L. trench or ditch) 1. Subscapular attachments - subscapularis m. 2. Supraspinous attachments - supraspinatus m. 3. Infraspinous attachments - infraspinatus m. D. Spine (short, sharp thorn-like process of a bone) 1. Crest (L. crista, bony ridge) attachments - trapezius m. 2. Acromion attachments - deltoid m. function - articulates with clavicle 3. Spinoglenoid notch function - transmits the suprascapular n., a. & v. E. Glenoid cavity (G. glenoeides, resembles eye) function - articulates with head of humerus 1. Supraglenoid tubercle (L. tuber, swelling) attachments - biceps (long) m. 2. Infraglenoid tubercle attachments - triceps (long) m. F. Coracoid process (G. korakodes, like a raven's beak) attachments - conoid & trapezoid lig., pectoralis minor, coracobrachialis & biceps (short) m. -

Ligaments and Joints of the Upper Limb
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Ligaments and Joints of the Upper Limb Sternoclavicular joint Type of joint Saddle type synovial joint; but it functions like a ball-and-socket joint Interclavicular ligament ATYPICAL: fibrocartilage cover articular surfaces Articulating surfaces Articular disc Sternal facet of clavicle, clavicular facet of manubrium There is also an ARTICULAR DISC Articular capsule Surrounds the joint, including the clavicular epiphysis Attached to the articular disc Lined with synovial membrane, contains synovial fluid Ligaments Anterior and posterior sternoclavicular ligaments Interclavcular ligament Costoclavicular ligament Anterior sternoclavicular ligament Stability factors Costoclavicular ligament Not many muscles around, and the surfaces are incongruous, so the joint relies on the ligaments for stability. Anterior and posterior sternoclavicular ligaments reinforce it anteriorly and posteriorly Interclavicular ligament reinforces it superiorly Costoclavicular ligament reinforces it inferiorly Articular disc limits medial displacement Posterior sternoclavicular ligament Movements Articular disc: attached to the anterior and posterior Flexion, extension, rotation, anterior and posterior sternoclavicular ligaments movement, circumduction Blood supply Internal thoracic and subscapular arteries Nerve supply Nerve to subclavius Anterior sternoclavicular ligament Medial supraclavicular nerve All joint