Subcostal Approach to Anterior Quadratus Lumborum Block for Pain Control Following Open Urological Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Unit #2 - Abdomen, Pelvis and Perineum
UNIT #2 - ABDOMEN, PELVIS AND PERINEUM 1 UNIT #2 - ABDOMEN, PELVIS AND PERINEUM Reading Gray’s Anatomy for Students (GAFS), Chapters 4-5 Gray’s Dissection Guide for Human Anatomy (GDGHA), Labs 10-17 Unit #2- Abdomen, Pelvis, and Perineum G08- Overview of the Abdomen and Anterior Abdominal Wall (Dr. Albertine) G09A- Peritoneum, GI System Overview and Foregut (Dr. Albertine) G09B- Arteries, Veins, and Lymphatics of the GI System (Dr. Albertine) G10A- Midgut and Hindgut (Dr. Albertine) G10B- Innervation of the GI Tract and Osteology of the Pelvis (Dr. Albertine) G11- Posterior Abdominal Wall (Dr. Albertine) G12- Gluteal Region, Perineum Related to the Ischioanal Fossa (Dr. Albertine) G13- Urogenital Triangle (Dr. Albertine) G14A- Female Reproductive System (Dr. Albertine) G14B- Male Reproductive System (Dr. Albertine) 2 G08: Overview of the Abdomen and Anterior Abdominal Wall (Dr. Albertine) At the end of this lecture, students should be able to master the following: 1) Overview a) Identify the functions of the anterior abdominal wall b) Describe the boundaries of the anterior abdominal wall 2) Surface Anatomy a) Locate and describe the following surface landmarks: xiphoid process, costal margin, 9th costal cartilage, iliac crest, pubic tubercle, umbilicus 3 3) Planes and Divisions a) Identify and describe the following planes of the abdomen: transpyloric, transumbilical, subcostal, transtu- bercular, and midclavicular b) Describe the 9 zones created by the subcostal, transtubercular, and midclavicular planes c) Describe the 4 quadrants created -

Anterior Abdominal Wall
Abdominal wall Borders of the Abdomen • Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below • Borders Superior: Costal cartilages 7-12. Xiphoid process: • Inferior: Pubic bone and iliac crest: Level of L4. • Umbilicus: Level of IV disc L3-L4 Abdominal Quadrants Formed by two intersecting lines: Vertical & Horizontal Intersect at umbilicus. Quadrants: Upper left. Upper right. Lower left. Lower right Abdominal Regions Divided into 9 regions by two pairs of planes: 1- Vertical Planes: -Left and right lateral planes - Midclavicular planes -passes through the midpoint between the ant.sup.iliac spine and symphysis pupis 2- Horizontal Planes: -Subcostal plane - at level of L3 vertebra -Joins the lower end of costal cartilage on each side -Intertubercular plane: -- At the level of L5 vertebra - Through tubercles of iliac crests. Abdominal wall divided into:- Anterior abdominal wall Posterior abdominal wall What are the Layers of Anterior Skin Abdominal Wall Superficial Fascia - Above the umbilicus one layer - Below the umbilicus two layers . Camper's fascia - fatty superficial layer. Scarp's fascia - deep membranous layer. Deep fascia : . Thin layer of C.T covering the muscle may absent Muscular layer . External oblique muscle . Internal oblique muscle . Transverse abdominal muscle . Rectus abdominis Transversalis fascia Extraperitoneal fascia Parietal Peritoneum Superficial Fascia . Camper's fascia - fatty layer= dartos muscle in male . Scarpa's fascia - membranous layer. Attachment of scarpa’s fascia= membranous fascia INF: Fascia lata Sides: Pubic arch Post: Perineal body - Membranous layer in scrotum referred to as colle’s fascia - Rupture of penile urethra lead to extravasations of urine into(scrotum, perineum, penis &abdomen) Muscles . -

The Female Pelvic Floor Fascia Anatomy: a Systematic Search and Review
life Systematic Review The Female Pelvic Floor Fascia Anatomy: A Systematic Search and Review Mélanie Roch 1 , Nathaly Gaudreault 1, Marie-Pierre Cyr 1, Gabriel Venne 2, Nathalie J. Bureau 3 and Mélanie Morin 1,* 1 Research Center of the Centre Hospitalier Universitaire de Sherbrooke, Faculty of Medicine and Health Sciences, School of Rehabilitation, Université de Sherbrooke, Sherbrooke, QC J1H 5N4, Canada; [email protected] (M.R.); [email protected] (N.G.); [email protected] (M.-P.C.) 2 Anatomy and Cell Biology, Faculty of Medicine and Health Sciences, McGill University, Montreal, QC H3A 0C7, Canada; [email protected] 3 Centre Hospitalier de l’Université de Montréal, Department of Radiology, Radio-Oncology, Nuclear Medicine, Faculty of Medicine, Université de Montréal, Montreal, QC H3T 1J4, Canada; [email protected] * Correspondence: [email protected] Abstract: The female pelvis is a complex anatomical region comprising the pelvic organs, muscles, neurovascular supplies, and fasciae. The anatomy of the pelvic floor and its fascial components are currently poorly described and misunderstood. This systematic search and review aimed to explore and summarize the current state of knowledge on the fascial anatomy of the pelvic floor in women. Methods: A systematic search was performed using Medline and Scopus databases. A synthesis of the findings with a critical appraisal was subsequently carried out. The risk of bias was assessed with the Anatomical Quality Assurance Tool. Results: A total of 39 articles, involving 1192 women, were included in the review. Although the perineal membrane, tendinous arch of pelvic fascia, pubourethral ligaments, rectovaginal fascia, and perineal body were the most frequently described structures, uncertainties were Citation: Roch, M.; Gaudreault, N.; identified in micro- and macro-anatomy. -

Hernias of the Abdominal Wall: Inguinal Anatomy in the Male
Hernias of the Abdominal Wall: Inguinal Anatomy in the Male Bob Caruthers. CST. PhD The surgical repair of an inguinal hernia, although one of the in this discussion. The anterolateral group consists of two mus- most common of surgical procedures, presents a special chal- cle groups whose bodies are near the midline and whose fibers lenge: Groin anatomy remains one of the more difficult topics are oriented vertically in the standing human: the rectus abdo- to master for both the entry-level student and the first assistant. minis and the pyramidalis. The muscle bodies of the other This article reviews the relevant anatomy of the male groin. three groups are more lateral, have significantly larger aponeu- roses, and have obliquely oriented fibers. These three groups MAJOR FASClAL AND UGAMENTAL STRUCTURES contribute the major portion of the fascia1 and ligamental The abdominal wall contains muscle groups representing two structures in the groin area.',!.' broad areas: anterolateral and posterior (see Figure 1).The At the level of the inguinal canal, the layers of the abdomi- posterior muscles, the quadratus lumborum, do not concern us nal wall include skin, subcutaneous tissue (Camper's and aponeurosis (cut edge) Internal abdominal (cut and turned down) Lacunar (Gimbernatk) ligament Inguinal (Poupart k) 11ganenr Cremaster muscle (medial origin) Cremaster muscle [lateral origin) Falx inguinalis [conjoined tendon) Cremaster muscle and fascia Reflected inguinal ligament External spermatic fascia (cut) Figun, 1-Dissection of rhe anterior ahdominal wall. Rectus sheath (posterior layerl , Inferior epigastric vessels Deep inguinal ring , Transversalis fascia (cut away) '.,."" -- Rectus abdomlnls muscle \ Antenor-supenor 111acspme \ -. ,lliopsoas muscle Hesselbach'sl triangle inguinalis (conjoined) , Tesricular vessels and genital branch of genitofmoral Scarpa's fascia), external oblique fascia, from the upper six ribs course downward inguinal (Poupart's) ligament. -

1 Anatomy of the Abdominal Wall 1
Chapter 1 Anatomy of the Abdominal Wall 1 Orhan E. Arslan 1.1 Introduction The abdominal wall encompasses an area of the body boundedsuperiorlybythexiphoidprocessandcostal arch, and inferiorly by the inguinal ligament, pubic bones and the iliac crest. Epigastrium Visualization, palpation, percussion, and ausculta- Right Left tion of the anterolateral abdominal wall may reveal ab- hypochondriac hypochondriac normalities associated with abdominal organs, such as Transpyloric T12 Plane the liver, spleen, stomach, abdominal aorta, pancreas L1 and appendix, as well as thoracic and pelvic organs. L2 Right L3 Left Visible or palpable deformities such as swelling and Subcostal Lumbar (Lateral) Lumbar (Lateral) scars, pain and tenderness may reflect disease process- Plane L4 L5 es in the abdominal cavity or elsewhere. Pleural irrita- Intertuber- Left tion as a result of pleurisy or dislocation of the ribs may cular Iliac (inguinal) Plane result in pain that radiates to the anterior abdomen. Hypogastrium Pain from a diseased abdominal organ may refer to the Right Umbilical Iliac (inguinal) Region anterolateral abdomen and other parts of the body, e.g., cholecystitis produces pain in the shoulder area as well as the right hypochondriac region. The abdominal wall Fig. 1.1. Various regions of the anterior abdominal wall should be suspected as the source of the pain in indi- viduals who exhibit chronic and unremitting pain with minimal or no relationship to gastrointestinal func- the lower border of the first lumbar vertebra. The sub- tion, but which shows variation with changes of pos- costal plane that passes across the costal margins and ture [1]. This is also true when the anterior abdominal the upper border of the third lumbar vertebra may be wall tenderness is unchanged or exacerbated upon con- used instead of the transpyloric plane. -

Review Article Ultrasound-Guided Quadratus Lumborum Block: an Updated Review of Anatomy and Techniques
Hindawi BioMed Research International Volume 2017, Article ID 2752876, 7 pages https://doi.org/10.1155/2017/2752876 Review Article Ultrasound-Guided Quadratus Lumborum Block: An Updated Review of Anatomy and Techniques Hironobu Ueshima,1 Hiroshi Otake,1 and Jui-An Lin2 1 Department of Anesthesiology, Showa University Hospital, Tokyo, Japan 2Department of Anesthesiology, Wan Fang Hospital, Taipei Medical University and Department of Anesthesiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan Correspondence should be addressed to Hironobu Ueshima; [email protected] Received 31 October 2016; Accepted 24 November 2016; Published 3 January 2017 Academic Editor: Eberval G. Figueiredo Copyright © 2017 Hironobu Ueshima et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Purpose of Review. Since the original publication on the quadratus lumborum (QL) block, the technique has evolved significantly during the last decade. This review highlights recent advances in various approaches for administering the QL block and proposes directions for future research. Recent Findings. The QL block findings continue to become clearer. We now understand that the QL block has several approach methods (anterior, lateral, posterior, and intramuscular) and the spread of local anesthetic varies with each approach. In particular, dye injected using the anterior QL block approach spread to the L1, L2, and L3 nerve roots and within psoas major and QL muscles. Summary. The QL block is an effective analgesic tool for abdominal surgery. However, the best approach is yet to be determined. -

2. Abdominal Wall and Hernias
BWH 2015 GENERAL SURGERY RESIDENCY PROCEDURAL ANATOMY COURSE 2. ABDOMINAL WALL AND HERNIAS Contents LAB OBJECTIVES ............................................................................................................................................... 2 Knowledge objectives .................................................................................................................................. 2 Skills objectives ............................................................................................................................................ 2 Preparation for lab .......................................................................................................................................... 2 1.1 ORGANIZATION OF THE ABDOMINAL WALL ............................................................................................ 4 Organization of the trunk wall .................................................................................................................... 4 Superficial layers of the trunk wall ............................................................................................................. 5 Musculoskeletal layer of the anterolateral abdominal wall ...................................................................... 7 T3/Deep fascia surrounding the musculoskeletal layer of the abdominal wall ..................................... 11 Deeper layers of the trunk wall ............................................................................................................... -
Fibrous Configuration of the Fascia Iliaca Compartment: an Epoxy Sheet
www.nature.com/scientificreports OPEN Fibrous confguration of the fascia iliaca compartment: An epoxy sheet plastination and confocal microscopy study Zhaoyang Xu1,2, Bin Mei3, Ming Liu4, Lili Tu1, Han Zhang5 & Ming Zhang2* Background and Objectives: The underlying anatomical mechanism of the ultrasound-guided fascia iliaca compartment (FIC) block for anaesthesia and analgesia in the lower limb has not been illuminated and numerous variations were attempted to achieve an optimal needle placement. This study aimed to defne the fbrous confguration of the FIC. Methods: A total of 46 adult cadavers were studied using dissection, latex injection, epoxy sheet plastination and confocal microscopy. Results: (1) The fascia iliaca originated from the peripheral fascicular aponeurotic sheet of the iliopsoas. (2) The FIC was a funnel-shaped adipose space between the fascia iliaca and the epimysium of the iliopsoas, had a superior and an inferior opening and contained the femoral and lateral femoral cutaneous nerves but not obturator nerve. (3) The estimated volume of the FIC in the cadavers was about 23 mls, of which about one third was below the level of the anterior superior iliac spine. Conclusions: This study revealed that the fascia iliaca was aponeurotic and may be less permeable for the local anesthetics. Conclusions: The FIC contained only the femoral and lateral femoral cutaneous nerves and communicated with the extraperitoneal space and femoral triangle adipose space via its superior and inferior opening, respectively. Te fascia iliaca compartment block (FICB) has been used for anaesthesia and analgesia in knee and hip surgery1 and acute pain management2. Te FICB technique is established on a hypothesis that the femoral, lateral femo- ral cutaneous (LFCN), genitofemoral and obturator nerves lie close together within the same fascial envelope, namely the fascia iliaca compartment (FIC)1,3, thus its key technical point is to deliver the local anaesthetic (LA) into this fascial envelope. -

Inguinal Canal)
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Abdomen and Pelvis, Inguinal Region (Inguinal Canal) Authors Faiz Tuma1; Matthew Varacallo2. Affiliations 1 Central Michigan University College of Medicine 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: January 10, 2019. Introduction The inguinal canal, located just above the inguinal ligament, is a small passage that extends medially and inferiorly through the lower part of the abdominal wall. This canal is about four to six centimeters in length and runs in a parallel fashion. The canal functions as a passageway for structures that extend from the abdominal cavity to the scrotum. In males, it transmits the spermatic cord, while in females, it transmits the round ligament of the uterus.[1] [2] Structure and Function The anatomy of the inguinal canal is important to know because it has clinical relevance. When defects occur in the abdominal wall in this location, hernias can develop. These often need to be surgically repaired to avoid long-term complications and to improve patient outcomes. It is important for surgeons to note that the mid-inguinal point marks the area between the anterior superior iliac spine and the pubic symphysis. Deep in this location, the femoral artery in the pelvic cavity enters the lower limb. The femoral artery can only be palpated below the inguinal ligament.[3][4] Embryology During embryogenesis, the testes are located in the posterior abdominal wall and gradually migrate into the scrotal area. -
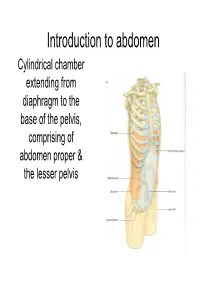
Introduction to Abdoman
Introduction to abdomen Cylindrical chamber extending from A diaphragm to the base of the pelvis, comprising of abdomen proper & the lesser pelvis -+------- Lower limb • Abdomen proper & lesser pelvis communicate with each other at the plane of inlet into lesser pelvis (upper border of pubic symphysis,pubic crests, arcuate line of innominate bones,sacral promontary) pelvis Pelvic inlet Inguinal ligament • Contents of Abdomen proper:- Most of the digestive tube, Liver, pancreas, spleen, kidneys, ureters (in part), supra renal gland & various blood &lymph vessels lymph nodes &nerves • Contents of lesser pelvis:- Terminal parts of ureters, urinary bladders, the sigmoid colon, rectum some coils of ileum, internal genitalia, blood & lymph vesels, lymph nodes & nerves Functions • Houses & protects major viscera Rib cage Assists in breathing of Relaxation of diaphragm diaphragm Relaxation of abdominal muscles Contraction of abdominal muscles Expiration Inspiration Changes in the intra abdominal pressure Laryngeai cav'ity c·1os 1erd Cr0ntrac ion of abdominal wal I ncrease in intra- abdominal pressure _..l,....._ Mictu ·ition Child birth Defecation Component parts ony Frame,vork of Abdomen • Wall- Skeletal elements Muscles • Muscles:- Superficial fascia • Anteriorly a Fatty layer Membranous layer (Camper's) (Scarpa's) segmented Transversalis fascia muscle Rectus [=E<trapedtoceru..; abdominis Parietal peritoneum Visceral peritoneum • Anterolateraly External oblique, internal oblique & trasversus abdominis ~.34 Transverse section showing the layers of the abdominal wa ll. Po~ t ei·i 01· .--\. lJcl 0111in a] \,-a]] • Posteriorly- Quadratus lumborum, psoas major & iliacus Abdominal regions Subcostal plane Midclavicular planes ,7 I I Left lowe ( I. _ quadr;mt Transumbilical plane Median plane Transtubercular plane Regions on anterior abdominal wall vertic~I plane Left ve rtical p,lane ' Hypochondriac Hypochondriac L / ' / ' ,/ '' / ' ✓ ' Subcostal plane ,-.;;'-~_,,:;.....,,,___ --i--------------~+-----'_ ......;;_..,,___. -

Quadratus Lumborum Block: a Technical Review
Current Anesthesiology Reports (2019) 9:257–262 https://doi.org/10.1007/s40140-019-00338-9 REGIONAL ANESTHESIA (P KUKREJA, SECTION EDITOR) Quadratus Lumborum Block: a Technical Review Avni Gupta1 & Rakesh Sondekoppam2 & Hari Kalagara3 Published online: 22 June 2019 # The Author(s) 2019, corrected publication November 2019 Abstract Purpose of Review Ultrasound-guided quadratus lumborum block (QLB) is gaining popularity in regional anesthesia for various surgical procedures. The purpose of this review is to understand the relevant clinical anatomy, different mechanisms of actions, and techniques used for the block and clinical evidence so far. Recent Findings The current data suggests a wide dermatomal distribution of the local anesthetic from T7-L2. The evidence regarding its utility is still evolving but has shown reduced opioid requirements for cesarean sections, lower abdominal surgery, and hip surgery. Prolonged analgesia has been reported as compared with more conventional transversus abdominis plane (TAP) block. This block has also been reported for above knee amputation, femoral-pop bypass, lumbar laminectomy and fusion, iliac crest bone graft, and iliac and acetabulum fracture. Summary Quadratus lumborum can be performed through different approaches which requires sound knowledge of anatomy. Further research to determine which approach yields best results is warranted. Keywords Quadratus lumborum block . Ultrasound . Regional anesthesia . Cesarean section . Abdominal procedures . Hip surgery Introduction blockade [7–9]. Further research regarding the best technique to do this block is warranted. Quadratus lumborum block (QLB) under ultrasound has been one of the interfascial plane blocks being popularized in re- gional anesthesia over the last few years given the vast number of indications in a variety of abdomino-pelvic surgeries in Anatomical Considerations pediatrics and adults. -

Concepts That Prevent Inguinal Hernia Formation – Revisited New Concepts of Inguinal Hernia Prevention
Central Annals of Emergency Surgery Bringing Excellence in Open Access Short Communication *Corresponding author M. P. Desarda, Department of surgery, Hernia Centre, Poona Hospital & Research Centre, 18, Vishwalaxmi Concepts that Prevent Inguinal Hsg. Society, Near Mayur Colony, Kothrud, Pune- 411038, India, Tel: 0091-7738181022; Email: Hernia Formation – Revisited Submitted: 29 November 2016 Accepted: 24 January 2017 New Concepts of Inguinal Published: 26 January 2017 Copyright Hernia Prevention © 2017 Desarda OPEN ACCESS M. P. Desarda1,2* 1Department of surgery, Poona Hospital & Research Centre, Pune Keywords 2Hernia Centre, Poona Hospital & Research Centre, Pune • Inguinal canal anatomy • Physiology • Theories that prevent hernia formation Abstract The author was not satisfied with the present concept about the strength of the transversalis fascia that is said to prevent inguinal hernia formation in the normal individuals. Therefore, this study was conducted to see the anatomical status of transversalis fascia and presence or absence of aponeurotic extensions in the posterior wall of the inguinal canals as were described by some stalwarts like Condon, Nehus etc. Methods: This is a prospective study of 30 inguinal canals opened for inguinal hernia surgery and 30 for varicocoele or lipoma of the cord (No hernia) surgery from January 2007 to December 2012. Inguinal canals were opened under local anesthesia and without any sedation. Lipoma were excised, varicocoele ligated and the hernia repaired by authors technique [1]. Observations were made about the structure of the inguinal canal, more particularly the posterior wall. Results: 30 inguinal canals opened for lipoma or varicocele surgery without hernia showed full cover of the aponeurotic extensions of varying density and out of 30 inguinal canals opened for hernia surgery, 24 did not show presence of the aponeurotic extensions and 6 canals showed deficient or scanty aponeurotic extensions.