Chapter 25 SPORTS and RECREATION OPPORTUNITIES
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disability Classification System
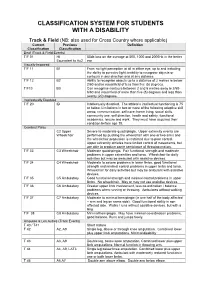
CLASSIFICATION SYSTEM FOR STUDENTS WITH A DISABILITY Track & Field (NB: also used for Cross Country where applicable) Current Previous Definition Classification Classification Deaf (Track & Field Events) T/F 01 HI 55db loss on the average at 500, 1000 and 2000Hz in the better Equivalent to Au2 ear Visually Impaired T/F 11 B1 From no light perception at all in either eye, up to and including the ability to perceive light; inability to recognise objects or contours in any direction and at any distance. T/F 12 B2 Ability to recognise objects up to a distance of 2 metres ie below 2/60 and/or visual field of less than five (5) degrees. T/F13 B3 Can recognise contours between 2 and 6 metres away ie 2/60- 6/60 and visual field of more than five (5) degrees and less than twenty (20) degrees. Intellectually Disabled T/F 20 ID Intellectually disabled. The athlete’s intellectual functioning is 75 or below. Limitations in two or more of the following adaptive skill areas; communication, self-care; home living, social skills, community use, self direction, health and safety, functional academics, leisure and work. They must have acquired their condition before age 18. Cerebral Palsy C2 Upper Severe to moderate quadriplegia. Upper extremity events are Wheelchair performed by pushing the wheelchair with one or two arms and the wheelchair propulsion is restricted due to poor control. Upper extremity athletes have limited control of movements, but are able to produce some semblance of throwing motion. T/F 33 C3 Wheelchair Moderate quadriplegia. Fair functional strength and moderate problems in upper extremities and torso. -

1-+ W / T:M/Rt=A-~
aker Environmental, Inc. Airport Office Park, Building 3 420 Rouser Road Coraopolis, Pennsylvania 15108 ( 412) ;s9-6000 FAX (412) 269-2002 October 29, 1998 ;}Lj I <D I ~ b ?_D _/ ~ pt - Mr. Wen C. Huang, P.E. 1-+ W/ Minnesota/Wisconsin Section t:m/Rt=A-~ RCRA Permitting Branch HRP-8J RegionS 77 West Jackson Boulevard Chicago, Illinois 60604-3590 Subject: Technical Scope ofWork and Proposed Project Schedule Tank Farm Area Closure PPG Industries, Inc. Oak Creek, Wisconsin WID 059 972 935 Dear Mr. Huang: As per your correspondence to Mr. Tom Yurick ofPPG dated October 8, 1998 attached please find a copy of the Teclmical Scope of Work (including an attached addendum) for the Tank Farm Area Closure (i.e., UST closure and soil and groundwater remediation) at PPG's Oak Creek Wisconsin facility. The proposed project schedule is presented below: Activity/Description Bids for Tank Fann Area Closure Received by PPG 1119/98 Contract Award 11/25/98 USTs Removed from Service 12/22/98 Field Mobilization of Tank Farm Area Closure Contractor 1/4/99* Submission of CMS Workplan to EPA 2/1/99 Tank Cleaning, Removal, and In-Place Closure Complete 3/1/99* Soil and Groundwater Remediation Start-up 4/1/99* Soil and Groundwater Remediation Complete 12/1/99* Activity dates assigned an asterisk are target dates which will be confinned upon the acceptance of the schedule proposed by the successful bidder. PPG will submit a revised schedule to EPA subsequent to a contract being awarded. PPG will submit a progress and monitoring report bi-monthly to EPA and with copies to Wisconsin DNR for the duration of Tank Farm Area Clos~re activities. -
Ifds Functional Classification System & Procedures
IFDS FUNCTIONAL CLASSIFICATION SYSTEM & PROCEDURES MANUAL 2009 - 2012 Effective – 1 January 2009 Originally Published – March 2009 IFDS, C/o ISAF UK Ltd, Ariadne House, Town Quay, Southampton, Hampshire, SO14 2AQ, GREAT BRITAIN Tel. +44 2380 635111 Fax. +44 2380 635789 Email: [email protected] Web: www.sailing.org/disabled 1 Contents Page Introduction 5 Part A – Functional Classification System Rules for Sailors A1 General Overview and Sailor Evaluation 6 A1.1 Purpose 6 A1.2 Sailing Functions 6 A1.3 Ranking of Functional Limitations 6 A1.4 Eligibility for Competition 6 A1.5 Minimum Disability 7 A2 IFDS Class and Status 8 A2.1 Class 8 A2.2 Class Status 8 A2.3 Master List 10 A3 Classification Procedure 10 A3.0 Classification Administration Fee 10 A3.1 Personal Assistive Devices 10 A3.2 Medical Documentation 11 A3.3 Sailors’ Responsibility for Classification Evaluation 11 A3.4 Sailor Presentation for Classification Evaluation 12 A3.5 Method of Assessment 12 A3.6 Deciding the Class 14 A4 Failure to attend/Non Co-operation/Misrepresentation 16 A4.1 Sailor Failure to Attend Evaluation 16 A4.2 Non Co-operation during Evaluation 16 A4.3 International Misrepresentation of Skills and/or Abilities 17 A4.4 Consequences for Sailor Support Personnel 18 A4.5 Consequences for Teams 18 A5 Specific Rules for Boat Classes 18 A5.1 Paralympic Boat Classes 18 A5.2 Non-Paralympic Boat Classes 19 Part B – Protest and Appeals B1 Protest 20 B1.1 General Principles 20 B1.2 Class Status and Protest Opportunities 21 B1.3 Parties who may submit a Classification Protest -

Reducts in Multi-Adjoint Concept Lattices
Reducts in Multi-Adjoint Concept Lattices Maria Eugenia Cornejo1, Jes´usMedina2, and Elo´ısa Ram´ırez-Poussa2 1 Department of Statistic and O.R., University of C´adiz.Spain Email: [email protected] 2 Department of Mathematics, University of C´adiz.Spain Email: fjesus.medina,[email protected] Abstract. Removing redundant information in databases is a key issue in Formal Concept Analysis. This paper introduces several results on the attributes that generate the meet-irreducible elements of a multi-adjoint concept lattice, in order to provide different properties of the reducts in this framework. Moreover, the reducts of particular multi-adjoint concept lattices have been computed in different examples. Keywords: attribute reduction, reduct, multi-adjoint concept lattice 1 Introduction Attribute reduction is an important research topic in Formal Concept Analysis (FCA) [1, 4, 10, 15]. Reducts are the minimal subsets of attributes needed in or- der to compute a lattice isomorphic to the original one, that is, that preserve the whole information of the original database. Hence, the computation of these sets is very interesting. For example, they are useful in order to obtain attribute implications and, since the complexity to build concept lattices directly depend on the number of attributes and objects, if a reduct can be detected before com- puting the whole concept lattice, the complexity will significantly be decreased. Different fuzzy extensions of FCA have been introduced [2, 3, 9, 14]. One of the most general is the multi-adjoint concept lattice framework [11, 12]. Based on a characterization of the meet-irreducible elements of a multi-adjoint concept lattice, a suitable attribute reduction method has recently been presented in [6]. -

Grade Conversion Tables for Study Abroad
Grade conversion tables for study abroad NB These tables should only be used to convert grades FROM study abroad TO University of Glasgow grades. They should NOT be used to indicate the equivalence of University of Glasgow Grades to those from other institutions. Translation of Grades Working Group – November 2020 [minor updates – August 2021] Revised March 2019 Minor correction November 2019 Argentina Argentina Glasgow Grade 10 A1 9 A4 8 B1 7 B3 6 C2 5 D1 4 D3 3 E2 2 F2 1 G2 Rationale The table is based on the current partnership with Universidad del Salvador. Subjects with Partners in Argentina: University-wide Australia Australia Glasgow Grade 90-100% A1 85-89 A3 80-84 A5 75-79 B1 70-74 B2 65-69 B3 60-64 C1 55-59 C3 50-54 D2 44-49 E1 39-43 E2 34-38 E3 29-33 F1 24-28 F2 19-23 F3 14-18 G1 9-13 G2 0-8 H 2 University of Queensland Grade Glasgow Grade 7 (High Distinction) A2 6 (Distinction) A4 5 (Credit) B2 4 (Pass) C2 3 (Limited Pass) D2 2 (Fail) E2 1 (Fail) F2 Queensland University of Technology Grade Glasgow Grade 7 (85-100%) A1 6 (80-84%) A4 6 (75-79%) B1 5 (70-74%) B2 5 (65-69%) B3 4 (60-64%) C1 4 (50-59%) C3 3 (47-49%) D2 2 (35-46%) E2 2 (25-34%) F2 1 (0-24%) G1 Rationale The University of Queensland uses a different scale which precludes it from the national table above. -

VMAA-Performance-Sta
Revised June 18, 2019 U.S. Department of Veterans Affairs (VA) Veteran Monthly Assistance Allowance for Disabled Veterans Training in Paralympic and Olympic Sports Program (VMAA) In partnership with the United States Olympic Committee and other Olympic and Paralympic entities within the United States, VA supports eligible service and non-service-connected military Veterans in their efforts to represent the USA at the Paralympic Games, Olympic Games and other international sport competitions. The VA Office of National Veterans Sports Programs & Special Events provides a monthly assistance allowance for disabled Veterans training in Paralympic sports, as well as certain disabled Veterans selected for or competing with the national Olympic Team, as authorized by 38 U.S.C. 322(d) and Section 703 of the Veterans’ Benefits Improvement Act of 2008. Through the program, VA will pay a monthly allowance to a Veteran with either a service-connected or non-service-connected disability if the Veteran meets the minimum military standards or higher (i.e. Emerging Athlete or National Team) in his or her respective Paralympic sport at a recognized competition. In addition to making the VMAA standard, an athlete must also be nationally or internationally classified by his or her respective Paralympic sport federation as eligible for Paralympic competition. VA will also pay a monthly allowance to a Veteran with a service-connected disability rated 30 percent or greater by VA who is selected for a national Olympic Team for any month in which the Veteran is competing in any event sanctioned by the National Governing Bodies of the Olympic Sport in the United State, in accordance with P.L. -

Importance of Physical Education, Sports and Yoga in the Life of Person
International Journal of Yogic, Human Movement and Sports Sciences 2019; 4(1): 1040-1043 ISSN: 2456-4419 Impact Factor: (RJIF): 5.18 Yoga 2019; 4(1): 1040-1043 Importance of physical education, sports and yoga in © 2019 Yoga www.theyogicjournal.com the life of person with disabilities Received: 10-11-2018 Accepted: 13-12-2018 Dr. Ruby Malik Dr. Ruby Malik, Neha Yadav and Aparna Lecturer, DIET, Moti Bagh. New Delhi, India Abstract According to World Bank, India has some 40 to 80 million persons with disability that translates to Neha Yadav roughly about size of population of United Kingdom. As per WHO “Disability is restriction or lack of Lecturer, DIET, Moti Bagh, ability to perform an activity in the manner or within the range considered normal for a normal human New Delhi, India being.” Precisely, one in twelve households has a member with disability. Although a number of sports Aparna events are held by government for disabled like Paralympics and awareness programmes by government Lecturer, DIET, Moti Bagh, regarding sports and disabled, a typical disabled person in a normal Indian house hold does not New Delhi, India participate in sports event nor he do exercises largely due to challenges posed by mobility and health issues along with mental and emotional barriers to exercise and hence, is more prone to diseases due to sedentary lifestyle and illnesses Research paper aims to emphasize on the importance of physical education, sports and yoga in the life of persons with disabilities and co-creating a society consisting people who are an asset to the country mainly through: Educating the disabled about various exercises and fitness techniques that can be performed easily at home and leads to a healthy lifestyle, Inclusion In Sports, through education and extensive overall sports programmes and spreading awareness among disabled. -

Recursive Syntactic Pattern Learning by Songbirds
Recursive syntactic pattern learning by songbirds Timothy Q. Gentner, Kimberly M. Fenn, Daniel Margoliash, and Howard C. Nusbaum Supplementary Information Table S1 provides an overview of all the training and testing conditions. Condition Stimulus 1 Baseline Training A2B2 and (AB)2, n=2 2 Transfer 1 Novel A2B2 and (AB)2, n=2 3 Probe Test 1 Familiar A2B2 and (AB)2, n=2 (80% of trials) Novel A2B2 and (AB)2, n=2 (10% of trials) Agrammatical AAAA, BBBB, ABBA, BAAB (10% of trials) 4 Probe Test 2 Familiar A2B2 and (AB)2, n=2 (80% of trials) Novel AnBn and (AB)n, n=3, 4 (20% of trials) 5 Probe Test 3 Familiar A2B2 and (AB)2, n=2 (80% of trials) A*B* (10% of trials) Novel AnBn and (AB)n, n=2,3,4 (10% of trials) Table S1. Overview of the training and testing conditions in order to which subjects were exposed. Stimuli marked with (*) comprised speech syllables instead of starling song motifs. Probe tests with novel A2B2 and (AB)2 stimuli Because the novel transfer stimuli were reinforced with the same response contingencies used in the initial training, the animals’ behaviour was changing (i.e. they were learning) as we measured generalization. To examine generalization without contingent reinforcement and thus without additional learning, we tested subjects using a “probe” procedure. The reinforcement regimen during probe sessions allowed us to measure generalization from the classes defined by the familiar CFG and FSG stimuli to novel stimuli without any direct effects of differential reinforcement learning on the latter (see Additional Methods). -
Field Indicators of Hydric Soils
United States Department of Field Indicators of Agriculture Natural Resources Hydric Soils in the Conservation Service United States In cooperation with A Guide for Identifying and Delineating the National Technical Committee for Hydric Soils Hydric Soils, Version 8.2, 2018 Field Indicators of Hydric Soils in the United States A Guide for Identifying and Delineating Hydric Soils Version 8.2, 2018 (Including revisions to versions 8.0 and 8.1) United States Department of Agriculture, Natural Resources Conservation Service, in cooperation with the National Technical Committee for Hydric Soils Edited by L.M. Vasilas, Soil Scientist, NRCS, Washington, DC; G.W. Hurt, Soil Scientist, University of Florida, Gainesville, FL; and J.F. Berkowitz, Soil Scientist, USACE, Vicksburg, MS ii In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, religion, sex, gender identity (including gender expression), sexual orientation, disability, age, marital status, family/parental status, income derived from a public assistance program, political beliefs, or reprisal or retaliation for prior civil rights activity, in any program or activity conducted or funded by USDA (not all bases apply to all programs). Remedies and complaint filing deadlines vary by program or incident. Persons with disabilities who require alternative means of communication for program information (e.g., Braille, large print, audiotape, American Sign Language, etc.) should contact the responsible Agency or USDA’s TARGET Center at (202) 720-2600 (voice and TTY) or contact USDA through the Federal Relay Service at (800) 877-8339. -

Today's Special Feature
2011 IIHF Asian Hockey Development Camp | Abu Dhabi, UAE F r i d a y , J u n e 1 7 , 2 0 1 1 41°C A b u D habi fun fact T O D A Y ’ S SPECIAL F E A T U R E The Emirates Palace Hotel in Abu Dhabi Zayed Sports City and the Armed Forces Officers Club: was the most expensive hotel ever built at the time it opened in 2005. The building is Our Homes for the Week nearly 1 km. long end to end and there are 114 domes, 302 rooms and 92 suites. The hotel has its own marina and helipad. HOCKEY F U N F A C T Ice hockey, field hockey and roller hockey aren’t the only types of hockey. There is also: air hockey, beach hockey, box hockey, deck hockey, mini-hockey, Nok hockey, power hockey, shinty, sponge, and even underwater hockey. DID YOU KNOW… This week we’re spending a lot of time in two specific locations in The highest mosque in the Abu Dhabi: the Zayed Sports City (ZSC) and the Armed Forces world is on the 158th floor of Officers Club (AFOC). Let’s get to know them a bit better! the Burj Khalifa in Dubai. ZSC was created in 1980 as a testament to the country’s passion for sports. ZSC includes a number of sports facilities besides a hockey rink, such as a bowling alley, tennis complex, rugby QUOTE OF THE DAY fields, a fitness center, softball fields, and a football/soccer "It is our attitude at the beginning of a stadium. -

Relationships Between the Velocity of the Ice Hockey
RELATIONSHIPS BETWEEN THE VELOCITY OF THE ICE HOCKEY WRIST SHOT AND SELECTED HUMAN FACTORS by PETER WILLIAM MOYLS B.P.E., The University of British Columbia, 1978 A THESIS SUBMITTED IN PARTIAL FULFILLMENTOOF THE REQUIREMENTS FOR THE DEGREE OF MASTERS OF PHYSICAL EDUCATION in THE FACULTY OF GRADUATE STUDIES (PHYSICAL EDUCATION) We accept this thesis as conforming to the required standard THE UNIVERSITY OF BRITISH COLUMBIA FEBRUARY .1981 ('cVeter Williatn'Moyls,"'1981 In presenting this thesis in partial fulfilment of the requirements for an advanced degree at the University of British Columbia, I agree that the Library shall make it freely available for reference and study. I further agree that permission for extensive copying of this thesis for scholarly purposes may be granted by the Head of my Department or by his representatives. It is understood that copying or publication of this thesis for financial gain shall not be allowed without my written permission. Department of Physical Education Graduate Studies The University of British Columbia 2075 Wesbrook Place Vancouver, Canada V6T 1W5 Date February 16,1981. ii ABSTRACT The main purpuse of this study was to investigate the relation• ships between the velocity of the ice hockey wrist shot and selected human factors in order to be able to predict the velocity of the wrist shot. A second objective was to identify the modifiable human factors most highly related with puck velocity in order to guide further research investigating the causal factors of a high speed wrist shot. Thirty-five subjects were selected from junior, intermediate, collegiate, senior and professional leagues to take part in the study. -

Cam Switches
Cam switches 10 Cam operated switches 11 General characteristics 12 Reference system 13 Technical data 14 Dimensions 18 Auxiliary contacts 19 Mounting possibilities 20 Mounting schemes 22 Special mountings 25 Accessories 31 Enclosures 32 Standard electrical schemes 46 Special diagrams 48 Main switches with undervoltage release 50 Discrepancy switches Cam switches Cam operated switches A5 cam operated switches have General characteristics been designed to operate as switch-disconnectors, main • Permits any electrical diagrams oxidation of their ferrous switches, load break switches, and makes the number of components. changeover switches, motor possible diagrams limitless. • High number of mechanical control switches,… • Abrupt breaking mechanism operations. with 30, 45, 60 o 90° positions, • According to RoHS standard. According to Standards according to diagram and requirements. • IEC 60947-3 • Contact decks made of self- • UL 508 extinguishing polyester reinforced with glass fi ber. • Silver alloy low resistance contacts with high arcing and welding characteristics. • Connection with protected cable clamps until 125A. • Electrolytic treatment against 10 low voltage electrical material Serie A5 low voltage electrical material General characteristics Simple "click" front plate fi xing Front plate designed for Internal and easy fi xing by simple push-in on the external links mounting plate Factory assembled links. Insulated external links protect against direct contact on live parts Metalic shaft Marking Optimal mechanical eff ort transmission