Health on Hills Draft Report of 4Th CRM: Arunachal Pradesh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Annual Report for the Year 2019-20
CIRCUIT HOUSE AT RUPA Completed during 2019-20 ARUNACHAL BHAWAN, MOHANBARI Completed during 2019-20 GOVERNMENT OF ARUNACHAL PRADESH PUBLIC WORKS DEPARTMENT ITANAGAR ANNUAL REPORT 2019-20 Visitor seating facility at Multipurpose Cultural Hall, Namsai Preface This Annual Report of the Public Works Department is prepared in the office of the Chief Engineer (SID&P) by compiling the achievements under the different zone during a financial year. The main objectives are to document and highlight the achievement of the department in execution of infrastructure as construction agency of the Gov- ernment. This process of publication of Annual Report is a legacy carried over from the process of submitting Annual Administrative Report during the time of CPWD in the State. During the year 2017-18, the achievements in construction of infrastructure under PWD were collected and the first edition of the annual report was published. The Annual Report 2017-18 & 2018-19 was circulated to all stake holders and made available in the official website www.arunachalpwd.org. The Annual Report 2018-19 was rated and ready reference source for important achieve- ments of PWD during 2018-19 and references for guidelines of CSS schemes being executed by PWD. In addition, while circulating the Annual Report 2018-19, it was requested that henceforth, the Annual Report shall be made an annual affair and to make it more befitting document for highlighting the achievements in each year, it was -re quested that the information may be submitted in time and as per the prescribed format, after the compilation of the financial and physical account of each preceding year. -

Ethnolinguistic Survey of Westernmost Arunachal Pradesh: a Fieldworker’S Impressions1
This is the version of the article/chapter accepted for publication in Linguistics of the Tibeto-Burman Area, 37 (2). pp. 198-239 published by John Benjamins : https://doi.org/10.1075/ltba.37.2.03bod This material is under copyright and that the publisher should be contacted for permission to re-use or reprint the material in any form Accepted version downloaded from SOAS Research Online: http://eprints.soas.ac.uk/34638 ETHNOLINGUISTIC SURVEY OF WESTERNMOST ARUNACHAL PRADESH: A FIELDWORKER’S IMPRESSIONS1 Linguistics of the Tibeto-Burman Area Timotheus Adrianus Bodt Volume xx.x - University of Bern, Switzerland/Tezpur University, India The area between Bhutan in the west, Tibet in the north, the Kameng river in the east and Assam in the south is home to at least six distinct phyla of the Trans-Himalayan (Tibeto-Burman, Sino- Tibetan) language family. These phyla encompass a minimum of 11, but probably 15 or even more mutually unintelligible languages, all showing considerable internal dialect variation. Previous literature provided largely incomplete or incorrect accounts of these phyla. Based on recent field research, this article discusses in detail the several languages of four phyla whose speakers are included in the Monpa Scheduled Tribe, providing the most accurate speaker data, geographical distribution, internal variation and degree of endangerment. The article also provides some insights into the historical background of the area and the impact this has had on the distribution of the ethnolinguistic groups. Keywords: Arunachal Pradesh, Tibeto-Burman, Trans-Himalayan, Monpa 1. INTRODUCTION Arunachal Pradesh is ethnically and linguistically the most diverse state of India. -

Histrical Background Changlang District Covered with Picturesque Hills Lies in the South-Eastern Corner of Arunachal Pradesh, Northeast India
Histrical Background Changlang District covered with picturesque hills lies in the south-eastern corner of Arunachal Pradesh, northeast India. It has an area of 4,662 sqr. Km and a population of 1,48,226 persons as per 2011 Census. According to legend the name Changlang owes its origin to the local word CHANGLANGKAN which means a hilltop where people discovered the poisonous herb, which is used for poisoning fish in the river. Changlang District has reached the stage in its present set up through a gradual development of Administration. Prior to 14th November 1987, it was a part of Tirap District. Under the Arunachal Pradesh Reorganization of Districts Amendment Bill, 1987,the Government of Arunachal Pradesh, formally declared the area as a new District on 14th November 1987 and became 10th district of Arunachal Pradesh. The legacy of Second World War, the historic Stilwell Road (Ledo Road), which was constructed during the Second World War by the Allied Soldiers from Ledo in Assam, India to Kunming, China via hills and valleys of impenetrable forests of north Burma (Myanmar) which section of this road is also passed through Changlang district of Arunachal Pradesh and remnant of Second World War Cemetery one can see at Jairampur – Nampong road. Location and Boundary The District lies between the Latitudes 26°40’N and 27°40’N, and Longitudes 95°11’E and 97°11’E .It is bounded by Tinsukia District of Assam and Lohit District of Arunachal Pradesh in the north, by Tirap District in the west and by Myanmar in the south-east. -

Changlang District the ICT Initiatives in the Land of Bio-Diversity
District Informatics Changlang District The ICT initiatives in The Land of Bio-diversity Edited by KAVITA BARKAKOTY he Changlang District, which is one of the easternmost districts of India, is located in the During the Covid-19 pandemic Tsouth-eastern corner of Arunachal Pradesh, having an international boundary with Myanmar period ICT services of the (Burma) in the east and the south. It has an area of National Informatics Centre, 4,662 sq. Km and a population of 1, 48,226 persons as per the 2011 Census. Changlang District was created Changlang District Centre became as the 10th District of the Arunachal Pradesh on 14 November 1987 by carving out part of Tirap District. all the more important. The NIC District Centre, Changlang District Centre in collaboration With its inception in July 1989, NIC Changlang district Centre started its journey with just one NIC with the State Centre officer and a single 386 machine with a handful of Changlang NIC Website has become a implemented various services, terminals. However, the modest resources did not come in their way towards providing ICT support to the single-window platform for accessing var- which facilitated the emergency district administration and in the implementation of ious citizen services, certificate applica- ICT-based citizen services and government schemes tions, Tender notices, Beneficiary details movement of people and goods. in the district. Being one of the remotest districts of Government schemes, and tourism-re- of the country with no other ISPs, in the early years lated information & services. Support was also provided to NICNET played a pivotal role in providing Internet 24x7 IVR helpline for public grievanc- es, e-passes, and online portal for goods help the District Administration in services to the district administration and other departments in the district. -

CENSUS HOUSES by PREDOMINANT MATERIAL of ROOF (Excluding Locked/Vacant Houses) Material of Roof
H-3A : CENSUS HOUSES BY PREDOMINANT MATERIAL OF ROOF (Excluding locked/vacant houses) Material of Roof Total/ Grass/ Thatch/ G.I./ State District Tahsil Town Total number of Hand Machine Table Name Area Name Rural/ Bamboo/ Plastic/ Burnt Metal/ Any other Code Code Code Code census houses made made Stone/Slate Concrete Urban Wood/ Mud, Polythene Brick Asbestos material Tiles Tiles etc. sheets 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 HL0303A 12 000 00000 000000 STATE - ARUNACHAL PRADESH Total 339,823 145,239 1,521 1,249 463 861 3,419 165,637 17,877 3,557 HL0303A 12 000 00000 000000 STATE - ARUNACHAL PRADESH Rural 249,860 131,972 1,157 827 203 318 1,898 106,948 3,853 2,684 HL0303A 12 000 00000 000000 STATE - ARUNACHAL PRADESH Urban 89,963 13,267 364 422 260 543 1,521 58,689 14,024 873 HL0303A 12 245 00000 000000 District - Tawang Total 11,151 938 15 10 6 10 99 9,137 871 65 HL0303A 12 245 00000 000000 District - Tawang Rural 9,052 912 14 10 6 9 81 7,667 294 59 HL0303A 12 245 00000 000000 District - Tawang Urban 2,099 26 1 - - 1 18 1,470 577 6 HL0303A 12 245 01556 000000 Sub-District - Zemithang Total 827 65 1 - 1 1 7 729 23 - HL0303A 12 245 01556 000000 Sub-District - Zemithang Rural 827 65 1 - 1 1 7 729 23 - HL0303A 12 245 01556 000000 Sub-District - Zemithang Urban - - - - - - - - - - HL0303A 12 245 01557 000000 Sub-District - Lumla Total 1,580 92 2 - 2 1 10 1,424 48 1 HL0303A 12 245 01557 000000 Sub-District - Lumla Rural 1,580 92 2 - 2 1 10 1,424 48 1 HL0303A 12 245 01557 000000 Sub-District - Lumla Urban - - - - - - - - - - HL0303A -

Districtwise Subsidy 1
DISTRICTWISE UNITS PRESENTLY ENJOYING BENEFITS UNDER THE CONETRAL TRANSPORT SUBSIDY SCHEME. SL. NAME OF NAME OF THE BENEFICIARY UNIT WITH ADDRESS NO. DISTRICTS 1 M/s Gamlin Fabrications, Industrial Estate, Naharlagun, Papum Pare District. Papum Pare 2 M/s Arunachal Furniture, Industrial Estate, Naharlagun, Papum Pare District Papum Pare 3 M/s L.T. Enterprise, Zero Point, Papum Pare District Papum Pare 4 M/s Tama Builders Consultant (P) Ltd., 'A' Sector, Naharlagun, Papum Pare District Papum Pare 5 M/s Kuku Engineering & Industrial Works, Naharlagun, Papum Pare District Papum Pare 6 M/s Taba Engineering Works, Naharlagun, Papum Pare District Papum Pare 7 M/s Premium Craft Korogation, Nirjuli, Papum Pare District Papum Pare 8 M/s Satyam Ispat, N.H. 52, Banderdewa, Papum Pare District Papum Pare 9 M/s SMS Smelters Ltd., Lekhi Village, Naharlagun, Papum Pare District Papum Pare 10 M/s Satyam Ispat NE Ltd., Banderdewa, Papum Pare District Papum Pare 11 M/s Satyam Coke, Banderdewa, Papum Pare District Papum Pare 12 M/s Dari Steel Fabrication, Palin, Kurung Kumey District Kurung Kumey 13 M/s Benzi Eastern Flour Mill, Tezu, Lohit District Lohit 14 M/s Topu Industries, Model Village, Naharlagun, Papum Pare District Papum Pare 15 M/s Taba Enterprise, Naharlagun, Papum Pare District Papum Pare 16 M/s Darbar Industries, Naharlagun, Papum Pare District Papum Pare 17 M/s Yangyio Fabrication Industries, Khimin, Papum Pare District Papum Pare 18 M/s Yayum Weaving Centre, khimin, Papum Pare District Papum Pare 19 M/s Yora Tobam Steel Fabrication, T.T. Marg, Itanagar, Papum Pare District Papum Pare 20 M/s Tai Enterprise, Kharsang, Changlang District Changlang 21 M/s Mount Valley Foods (P) Ltd., Bordumsa, Changlang District Changlang 22 M/s Bulo Steel Fabricator, Daporijo, Upper Subansiri District Upper Subansiri 23 M/s Pertin Wire Products, Yingkiong, Upper Siang District Upper Subansiri 24 M/s Siang Fruit Canning Factory, Nigmoi, East Siang District East Siang DISTRICTWISE UNITS ENJOYED BENEFITS UNDER THE SCHEME BUT CEASED TO AVAIL THE CENTRAL TRANSPORT SUBSIDY SL. -
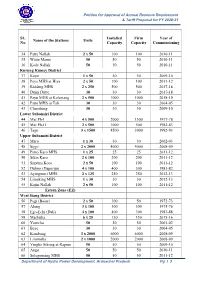
SL. No. Name of the Stations Units Installed Capacity Firm Capacity
Petition for Approval of Annual Revenue Requirement & Tariff Proposal for FY 2020-21 SL. Installed Firm Year of Name of the Stations Units No. Capacity Capacity Commissioning 34 Patta Nallah 2 x 50 100 100 2010-11 35 Watte Mame 50 50 50 2010-11 36 Kade Nallah 50 50 50 2010-11 Kurung Kumey District 37 Koye 1 x 50 50 50 2009-10 38 Paya MHS at Hiya 2 x 50 100 100 2011-12 39 Kidding MHS 2 x 250 500 500 2017-18 40 Dumi Dutte 30 30 30 2017-18 41 Payu MHS at Koloriang 2 x 500 1000 1000 2018-19 42 Patte MHS at Tali 30 30 30 2004-05 43 Chambang 30 30 30 2009-10 Lower Subansiri District 44 Mai Ph-I 4 x 500 2000 1500 1977-78 45 Mai Ph-II 2 x 500 1000 500 1982-83 46 Tago 3 x 1500 4500 3000 1992-93 Upper Subansiri District 47 Maro 1 x 30 30 30 2002-03 48 Sippi 2 x 2000 4000 4000 2008-09 49 Pinto Karo MHS 1 x 25 25 25 2011-12 50 Sikin Karo 2 x 100 200 200 2011-12 51 Sinyum Koro 2 x 50 100 100 2011-12 52 Dulom (Daporijo) 4 x 100 400 300 1981-82 53 Ayingmuri MHS 2 x 125 250 250 2012-13 54 Limeking MHS 1 x 30 30 30 2012-13 55 Kojin Nallah 2 x 50 100 100 2011-12 Estern Zone (EZ) West Siang District 56 Pagi (Basar) 2 x 50 100 50 1972-73 57 Along 3 x 100 300 300 1975-76 58 Ego-Echi (Dali) 4 x 100 400 300 1987-88 59 Mechuka 6 x 25 150 150 2015-16 60 Yomcha 50 50 50 2001-02 61 Beye 30 30 30 2004-05 62 Kambang 3 x 2000 6000 6000 2008-09 63 Liromoba 2 x 1000 2000 2000 2008-09 64 Yingko Sikong at Rapum 50 50 50 2009-10 65 Angu 50 50 50 2010-11 66 Solegomang MHS 50 50 50 2011-12 Department of Hydro Power Development, Arunachal Pradesh Pg l 3 Petition for Approval of Annual Revenue Requirement & Tariff Proposal for FY 2020-21 SL. -
The Arunachal Pradesh Gazette EXTRAORDINARY PUBLISHED by AUTHORITY No
The Arunachal Pradesh Gazette EXTRAORDINARY PUBLISHED BY AUTHORITY No. 80 Vol. XXVI, Naharlagun, Thursday, February 21, 2019, Phalguna 2, 1940 (Saka) OFFICE OF THE CHIEF ELECTORAL OFFICER ARUNACHAL PRADESH ITANAGAR The 19th February, 2019 No. EN/LEG/43/2019. —The following Notification issued by Election Commission of India, Nirvachan Sadan, Ashoka Road, New Delhi, and published in the Gazette of India Part-II, Section 3 Sub-Section (iii) dated 13th February, 2019, is reproduced below for general information. ELECTION COMMISSION OF INDIA Nlrvachan Sadan, Ashoka Road, New Delhl - 110001 13th February, 2019 Dated : 24 Magha, 1940 (Saka). NOTIFICATION No.434/ARUN-LA/2019(1) : - In exercise of the powers conferred by Sub-Section (1) of Section 22 of the Representation of the People Act,1951 (43 of 1951) and in supersession of its notification No.434/ARUN-LA/2014(1) dated 13th March, 2014, the Election Commission hereby appoints each of the officer of the Govemment of Arunachal Pradesh, as specified in column 2 of the Table below as the Assistant Returning Officer to assist the Returning Officer of the Assembly Constituency in the State of Arunachal Pradesh as specified in column 1 of the said table against such officer of the Government in the performance of the functions of such Returning Officer:- TABLE No. and Name of Assembly Assistant Returning Officers Constituency. 1 2 1-Lumla (ST) 1. Circle Officer, Lumla 2. Circle Officer, Dudunghar 3. Circle Officer, Zemithang 2-Tawang (ST) 1. Extra Assistant Commissioner, Tawang 2. Circle Officer, Kitpi 3-Mukto (ST) 1. Circle Officer, Jang 2. -
Working Paper-6 Final
Working Paper No. CDS/06/2020 Challenges of Development in the Border Areas: An Empirical Study Amitava Mitra June 2020 Centre for Development Studies Department of Economics Rajiv Gandhi University Rono Hills, Arunachal Pradesh Working Paper No. CDS/06/2020 Challenges of Development in the Border Areas: An Empirical Study Amitava Mitra June 2020 Centre for Development Studies Department of Economics, Rajiv Gandhi University Rono Hills, Arunachal Pradesh PREFACE The Centre for Development Studies (CDS) was set up as a research adjunct at the Department of Economics, Rajiv Gandhi University (RGU), Itanagar, Arunachal Pradesh, with a generous grant from the Ministry of Finance (Department of Economic Affairs), Government of India. The objectives of the Centre include the creation of high-quality research infrastructure for students, researchers and faculty members, in addition to sponsoring and coordinating research on various developmental issues having policy implications at the regional and national level. Publishing working/policy papers on the research outcome of the Centre, monographs and edited volumes are the key activities of the Centre. The present working paper by Prof. Amitava Mitra, titled, ‘Challenges of Development in the Border Areas of Arunachal Pradesh: An Empirical Study’, is an output of a research project. It is sixth in the series of working paper published by the Centre for Development Studies. The working paper has explored the wide ranging inter-district disparities in the state of Arunachal Pradesh, in terms of availability of infrastructural facilities that are crucial for improving the economic condition of people in the state. The districts of the northern and eastern international border areas, with high mountains are less well serviced than the districts in the foothills of Arunachal Pradesh. -

Shri Dorjee Khandu Hon’Ble Chief Minister Arunachal Pradesh
SPEECH OF SHRI DORJEE KHANDU HON’BLE CHIEF MINISTER ARUNACHAL PRADESH AT THE 54TH NDC MEETING AT VIGYAN BHAVAN New Delhi December 19, 2007 54TH NDC MEETING SPEECH OF SHRI DORJEE KHANDU HON’BLE CHIEF MINISTER ARUNACHAL PRADESH 2 Hon’ble Prime Minister and the Chairman of NDC, Hon’ble Deputy Chairman, Planning Commission, Hon’ble Union Ministers, My colleague Chief Ministers, Distinguished members of the Planning Commission, Senior Officers, Ladies and Gentlemen. It is indeed a proud privilege and honour for me to participate in this 54th NDC meeting. This meeting has been convened essentially to consider and approve the Draft 11th Five Year Plan (2007-2012). The visionary and comprehensive Eleventh Five Year Plan envisions to steer the process of development through rapid reduction of poverty and creation of employment opportunities, access to essential services like health and education specially for the poor, equality of opportunity, empowerment through education and skill development to meet the objectives of inclusiveness and sustainability . However, I would like to share our views on some of the important issues and recommendations highlighted in the agenda. 2) Let me start with reiterating what our Hon’ble Prime Minister has stated in his Independence Day address on 15th August 2005. “ in this new phase of development, we are acutely aware that all regions of the country should develop at the same pace. It is unacceptable for us to see any region of the country left behind other regions in this quest for development. In every scheme of the Government, we will be making all efforts to ensure that backward regions are adequately taken care of. -

Download Full Report
P�R�E�F�A�C�E� 1.� This�Report�has�been�prepared�for�submission�to�the� Governor under Article 151 of the Constitution.� 2.� Chapters�I�and�II�of�this�Report�respectively�contain�Audit� observations�on�matters�arising�from�examination�of� Finance�Accounts�and�Appropriation�Accounts�of�the�State� Government for the year ended 31 March 2010.� 3.� Chapter�III�on�‘Financial�Reporting’�provides�an�overview� and�status�of�the�State�Government’s�compliance�with� various�financial�rules,�procedures�and�directives�during� the current year.� 4.� Audit�observations�on�matter�arising�from�performance� audit�and�audit�of�transactions�in�various�departments� including�the�Public�Works�department,�audit�of�stores�and� stock,�audit�of�autonomous�bodies,�Statutory�Corporations,� Boards�and�Government�Companies�and�audit�of�revenue� receipts for the year ended 31 March 2010 are included in a� separate Report.� 5.� The�audit�has�been�conducted�in�conformity�with�the� Auditing�Standards�issued�by�the�Comptroller�and�Auditor� General of India. CHAPTER I Finances of the State Government Pr o f i l e of th e St a t e Area-wise, AR U N A C H A L PR A D E S H , which became a full-fledged state on February 20, 1987, is the largest state in the north-eastern region. Till 1972, it was known as the North- East Frontier Agency (NEFA). It gained the Union Territory status on January 20, 1972 and was renamed as Arunachal Pradesh. The State, being one of the Special Category State, is dependent on central assistance for plan investment because of poor resource base. -
Work Wise Details (RIDF State Share)
GOVERNMENT OF ARUNACHAL PRADESH PUBLIC WORKS DEPARTMENT SPECIAL ASSISTANCE PACKAGE (SAP) ANNUAL OPERATING PLAN 2007-2008 VOLUME – E COMMUNICATION SECTOR R.I.D.F. (NABARD) STATE SHARE I N D E X RURAL INFRASTRUCTURE DEVELOPMENT FUND (RIDF) Page No. Sl. No. Name of Division From To 12 34 FORMATS CSS-I (PART-I) 1 3 CSS-II (PART-I) 1 5 1. Tawang 1 2. Bomdila 2 3. Bameng 3 4. Seppa 4 5. Ziro 5 6 6. Sangram 7 9 7. Basar 10 8. Mariyang 11 9. Yingkiong 12 10. Roing 13 11. Jairampur 14 12. Khonsa 15 13. Longding 16 Page 1 FORMAT : CSS-I SPECIAL ASSISTANCE PACKAGE (SAP) ANNUAL OPERATING PLAN : 2007-2008 RURAL INFRASTRUCTURE DEVELOPMENT FUND (NABARD) (Rs. in lakh) Sl. Name of the Scheme Pattern of sharing Estimated Cost (State Share)Cummulative Expenditure Balance Proposed Outlay Remarks No. Expenditure during 9th & 10th Plan Estimated Cost 2007-2008 between Centre and period till March,2007 State Original Revised Total State State Share State Share 1 2 3 5 14 17 19 1 Ring Road at Zemithung (10.80 Km) in Centre - 80% 205.41 205.41 205.41 85.40 S/Culvert-20 Nos & Tawang District State - 20% R&B Wall-300 mtr Non-Divertable 2 Dirang-Tawang BRO Road to Sangti Centre - 80% 169.34 169.34 121.50 47.84 47.85 B/Topping-2.72 Km & Khali Bok via Khaso (14.50 km). State - 20% Steel Bridge-100% Non-Divertable 3 Road from Seppa-Chayangtajo to Centre - 80% 50.89 50.89 50.89 50.90 F/Cutting-3.50 Km Bameng (15.00 Km) in East Kameng State - 20% Non-Divertable District 4 Road from PWD IB to Bali in Seijosa Centre - 80% 252.47 252.47 252.47 100.45 F/Cutting-4.60 Km & (14.60 Km) in East Kameng District State - 20% S/Culvert-10 Nos Non-Divertable 5 Yazali-Mangio Road, (65.00 Km) Centre - 90% 281.99 142.60 424.59 242.36 182.23 82.25 S/Culvert-20 Nos & SH: F/C, Culverts, R&B Wall, State - 10% SBC-85.00 Km Sol, WBM, B/Topping i/c Bridges.