Proximal Hamstring Tears and Syndrome Elan J
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Iliopsoas Tendonitis/Bursitis Exercises
ILIOPSOAS TENDONITIS / BURSITIS What is the Iliopsoas and Bursa? The iliopsoas is a muscle that runs from your lower back through the pelvis to attach to a small bump (the lesser trochanter) on the top portion of the thighbone near your groin. This muscle has the important job of helping to bend the hip—it helps you to lift your leg when going up and down stairs or to start getting out of a car. A fluid-filled sac (bursa) helps to protect and allow the tendon to glide during these movements. The iliopsoas tendon can become inflamed or overworked during repetitive activities. The tendon can also become irritated after hip replacement surgery. Signs and Symptoms Iliopsoas issues may feel like “a pulled groin muscle”. The main symptom is usually a catch during certain movements such as when trying to put on socks or rising from a seated position. You may find yourself leading with your other leg when going up the stairs to avoid lifting the painful leg. The pain may extend from the groin to the inside of the thigh area. Snapping or clicking within the front of the hip can also be experienced. Do not worry this is not your hip trying to pop out of socket but it is usually the iliopsoas tendon rubbing over the hip joint or pelvis. Treatment Conservative treatment in the form of stretching and strengthening usually helps with the majority of patients with iliopsoas bursitis. This issue is the result of soft tissue inflammation, therefore rest, ice, anti- inflammatory medications, physical therapy exercises, and/or injections are effective treatment options. -

The Effect of Stretching Hamstring, Gastrocnemius, Iliopsoas
Open Journal of Therapy and Rehabilitation, 2015, 3, 139-145 Published Online November 2015 in SciRes. http://www.scirp.org/journal/ojtr http://dx.doi.org/10.4236/ojtr.2015.34019 The Effect of Stretching Hamstring, Gastrocnemius, Iliopsoas and Back Muscles on Pain and Functional Activities in Patients with Chronic Low Back Pain: A Randomized Clinical Trial Hamada E. Seif1, Aqeel Alenazi2, Sahar Mahmoud Hassan1, Shaji John Kachanathu3, Ashraf R. Hafez1* 1Cairo UniversityHospital, Cairo University, Cairo, Egypt 2Physical Therapy and Rehabilitation Department, College of Applied Medical Sciences, Salman Bin Abdulaziz University, Alkharj, Saudi Arabia 3Collage of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia Received 15 September 2015; accepted 6 November 2015; published 9 November 2015 Copyright © 2015 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract A back pain lasting more than 12 weeks has been defined as a chronic low back pain (LBP) [1]. More than half of people suffer from LBP [1]. The purpose of this study was to examine the effect of gastrocnemius muscle stretching in the treatment of chronic low back pain. Methods: Forty pa- tients with chronic low back pain, ages ranging from 25 to 40 years, were recruited and divided randomly into two groups. The control group followed a physical therapy program that included stretching exercises for back, hamstring and iliopsoas muscles. Strengthening exercises for abdo- minal muscle and postural instructions for activities of daily living were also performed. The ex- perimental group followed the same control-group exercises with the addition of stretching exer- cises for gastrocnemius muscles. -
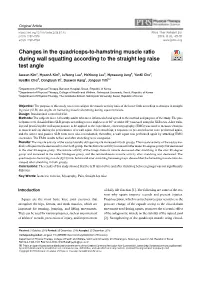
Changes in the Quadriceps-To-Hamstring Muscle
Original Article https://doi.org/10.14474/ptrs.2019.8.1.45 Phys Ther Rehabil Sci pISSN 2287-7576 2019, 8 (1), 45-51 eISSN 2287-7584 www.jptrs.org Changes in the quadriceps-to-hamstring muscle ratio http://crossmark.crossref.org/dialog/?doi=10.14474/ptrs.2019.8.1.45&domain=pdf&date_stamp=2019-3-25 during wall squatting according to the straight leg raise test angle Jaeeun Kima, HyeonA Kimb, JuYeong Leeb, HoYoung Leeb, Hyoseung Jungb, YunKi Chob, HyeMin Choib, Donghyun Yic, Daewon Kangc, Jongeun Yimb,c a Department of Physical Therapy, Barosun Hospital, Seoul, Republic of Korea b Department of Physical Therapy, College of Health and Welfare, Sahmyook University, Seoul, Republic of Korea c Department of Physical Therapy, The Graduate School, Sahmyook University, Seoul, Republic of Korea Objective: The purpose of this study was to investigate the muscle activity ratio of the lower limb according to changes in straight leg raise (SLR) test angles on hamstring muscle shortening during squat exercises. Design: Randomized controlled trial. Methods: The subjects were 14 healthy adults who were informed of and agreed to the method and purpose of the study. The par- ticipants were classified into SLR groups according to two angles (over 80° or under 80°) assessed using the SLR tests. After train- ing and practicing the wall squat posture to be applied to the experiment, electromyography (EMG) was used to measure changes in muscle activity during the performance of a wall squat. After stretching, a sequence of pre-stretch tests were performed again, and the active and passive SLR tests were also reconducted; thereafter, a wall squat was performed again by attaching EMG electrodes. -
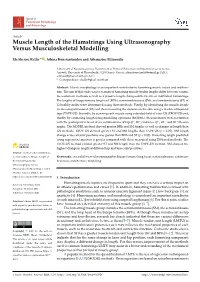
Muscle Length of the Hamstrings Using Ultrasonography Versus Musculoskeletal Modelling
Journal of Functional Morphology and Kinesiology Article Muscle Length of the Hamstrings Using Ultrasonography Versus Musculoskeletal Modelling Eleftherios Kellis * , Athina Konstantinidou and Athanasios Ellinoudis Laboratory of Neuromechanics, Department of Physical Education and Sport Sciences at Serres, Aristotle University of Thessaloniki, 62100 Serres, Greece; [email protected] (A.K.); [email protected] (A.E.) * Correspondence: [email protected] Abstract: Muscle morphology is an important contributor to hamstring muscle injury and malfunc- tion. The aim of this study was to examine if hamstring muscle-tendon lengths differ between various measurement methods as well as if passive length changes differ between individual hamstrings. The lengths of biceps femoris long head (BFlh), semimembranosus (SM), and semitendinosus (ST) of 12 healthy males were determined using three methods: Firstly, by identifying the muscle attach- ments using ultrasound (US) and then measuring the distance on the skin using a flexible ultrasound tape (TAPE-US). Secondly, by scanning each muscle using extended-field-of view US (EFOV-US) and, thirdly, by estimating length using modelling equations (MODEL). Measurements were performed with the participant relaxed at six combinations of hip (0◦, 90◦) and knee (0◦, 45◦, and 90◦) flexion angles. The MODEL method showed greater BFlh and SM lengths as well as changes in length than US methods. EFOV-US showed greater ST and SM lengths than TAPE-US (p < 0.05). SM length change across all joint positions was greater than BFlh and ST (p < 0.05). Hamstring length predicted using regression equations is greater compared with those measured using US-based methods. The EFOV-US method yielded greater ST and SM length than the TAPE-US method. -

Quadriceps and Hamstrings Coactivation in Exercises Used in Prevention And
bioRxiv preprint doi: https://doi.org/10.1101/574210; this version posted March 11, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 Quadriceps and hamstrings coactivation in exercises used in prevention and 2 rehabilitation of hamstring strain injury in young soccer players 3 Gonzalo Torres1¶; David Chorro1¶; Archit Navandar2¶; Javier Rueda1¶; Luís 4 Fernández3¶; Enrique Navarro1*¶ 5 6 1Faculty of Sport Sciences, Universidad Politécnica de Madrid, Madrid, Madrid, Spain. 7 2Faculty of Sport Sciences, Universidad Europea de Madrid, Madrid, Madrid, Spain. 8 3Medical Services of Atlético de Madrid, Club Atlético de Madrid, Madrid, Madrid, 9 Spain. 10 11 12 *Corresponding author 13 E-mail: [email protected] (EN) 14 15 ¶These authors contributed equally to this work. 16 17 18 19 20 21 22 23 24 bioRxiv preprint doi: https://doi.org/10.1101/574210; this version posted March 11, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 25 Abstract 26 This study aimed to study the co-activation of hamstring-quadriceps muscles 27 during submaximal strength exercises without the use of maximum voluntary isometric 28 contraction testing and compare (i) the inter-limb differences in muscle activation, (ii) the 29 intra-muscular group activation pattern, and (iii) the activation during different phases of 30 the exercise. -
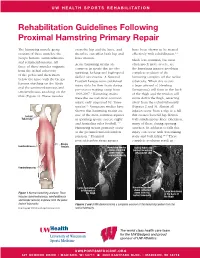
Rehabilitation Guidelines Following Proximal Hamstring Primary Repair
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines Following Proximal Hamstring Primary Repair The hamstring muscle group cross the hip and the knee, and have been shown to be treated consists of three muscles: the therefore can affect both hip and effectively with rehabilitation.1, 8 biceps femoris, semitendinosus knee motion. Much less common, but most and semimembranosus. All Acute hamstring strains are often much more severe, are three of these muscles originate common in sports that involve the hamstring injuries involving from the ischial tuberosity sprinting, kicking and high-speed complete avulsion of the of the pelvis and then insert skilled movements. A National hamstring complex off the ischial below the knee with the biceps Football League team published tuberosity. When this occurs femoris attaching on the fibula injury data for their team during a large amount of bleeding and the semimembranosus and pre-season training camp from (hematoma) will form in the back semitendinosus attaching on the 1998-2007.1 Hamstring strains of the thigh and the tendon will tibia (Figure 1). These muscles were the second most common move down the thigh, retracting injury, only surpassed by “knee away from the ischial tuberosity sprains”.1 Numerous studies have (Figures 2 and 3). Almost all shown that hamstring strains are injuries occur from a slip or a fall Ischial one of the most common injuries that creates forceful hip flexion Tuberosity in sprinting sports, soccer, rugby with simultaneous knee extension, and Australian rules football.1-12 -
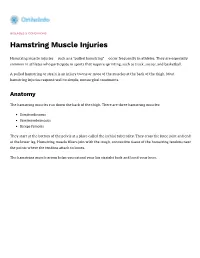
Hamstring Muscle Injuries
DISEASES & CONDITIONS Hamstring Muscle Injuries Hamstring muscle injuries — such as a "pulled hamstring" — occur frequently in athletes. They are especially common in athletes who participate in sports that require sprinting, such as track, soccer, and basketball. A pulled hamstring or strain is an injury to one or more of the muscles at the back of the thigh. Most hamstring injuries respond well to simple, nonsurgical treatments. Anatomy The hamstring muscles run down the back of the thigh. There are three hamstring muscles: Semitendinosus Semimembranosus Biceps femoris They start at the bottom of the pelvis at a place called the ischial tuberosity. They cross the knee joint and end at the lower leg. Hamstring muscle fibers join with the tough, connective tissue of the hamstring tendons near the points where the tendons attach to bones. The hamstring muscle group helps you extend your leg straight back and bend your knee. Normal hamstring anatomy. The three hamstring muscles start at the bottom of the pelvis and end near the top of the lower leg. Description A hamstring strain can be a pull, a partial tear, or a complete tear. Muscle strains are graded according to their severity. A grade 1 strain is mild and usually heals readily; a grade 3 strain is a complete tear of the muscle that may take months to heal. Most hamstring injuries occur in the thick, central part of the muscle or where the muscle fibers join tendon fibers. In the most severe hamstring injuries, the tendon tears completely away from the bone. It may even pull a piece of bone away with it. -

A Thesis Entitled Relationship Between Hamstring Strength And
A Thesis entitled Relationship Between Hamstring Strength and Agonist-Antagonist Co-Activation by Meghan Gregoire Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science Degree in Exercise Science with a Concentration in Athletic Training ___________________________________________ Grant Norte, PhD, AT, ATC, CSCS, Committee Chair ___________________________________________ Neal Glaviano, PhD, AT, ATC, Committee Member ___________________________________________ Amanda Murray, PT, DPT, PhD, Committee Member ___________________________________________ Lucinda Bouillon, PT, DPT, PhD, Committee Member ___________________________________________ Cyndee Gruden, PhD, Dean College of Graduate Studies The University of Toledo May 2019 Copyright 2019, Meghan Gregoire This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of Relationship Between Hamstring Strength and Agonist-Antagonist Co-Activation by Meghan Gregoire Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science Degree in Exercise Science The University of Toledo May 2019 Introduction: Anterior cruciate ligament (ACL) injury is common among females due to several neuromuscular risk factors. Decreased hamstrings to quadriceps (H:Q) ratio is one neuromuscular factor that place females at an increased risk of ACL injury. Increased activation of the hamstrings during functional tasks help assist the static stabilizes of the knee, decrease strain on the ACL and reduce anterior tibial translation. Objectives: The objective of this study was to (1) identify the relationship between H:Q strength and co- activation ratio in the medial and lateral compartments of the knee during the stance phase of walking gait as well as (2) compare H:Q ratio between high and low groups. -
Back of Thigh
Back of thigh Dr Garima Sehgal Associate Professor King George’s Medical University UP, Lucknow DISCLAIMER: • The presentation includes images which have been taken from google images or books. • The author of the presentation claims no personal ownership over these images taken from books or google images. • They are being used in the presentation only for educational purpose. Learning Objectives By the end of this teaching session on back of thigh – I all the MBBS 1st year students must be able to: • Enumerate the contents of posterior compartment of thigh • Describe the cutaneous innervation of skin of back of thigh • Enumerate the hamstring muscles • List the criteria for inclusion of muscles as hamstring muscles • Describe the origin, insertion, nerve supply & actions of hamstring muscles • Describe origin, course and branches of sciatic nerve • Write a short note on posterior cutaneous nerve of thigh • Write a note on arteries and arterial anastomosis at the back of thigh • Discuss applied anatomy of back of thigh Compartments of the thigh Cutaneous innervation of back of thigh 1 4 2 3 Contents of Back of thigh Muscles: Hamstring muscles & short head of biceps femoris Nerves: Sciatic nerve & posterior cutaneous nerve of thigh Arterial Anastomosis: The Posterior Femoral Cutaneous Nerve (n. cutaneus femoralis posterior) Dorsal divisions of – S1, S2 & Ventral divisions of S2, S3 Exits from pelvis through the greater sciatic foramen below the Piriformis. Descends beneath the Gluteus maximus with the inferior gluteal artery Runs down the back of the thigh beneath the fascia lata, to the back of the knee and leg Posterior Femoral Cutaneous Nerve contd…. -

“What Is This Pain in My Butt?”
TRAINING DOCTOR’S ORDERS “What is This Pain in My Butt?” Jordan D. Metzl, M.D. t’s a common problem I see in my office all the time. A triathlete or a runner is training Iintently and over a period of several weeks, develops a pain in the butt. Initially, this starts as a dull ache, and if they don’t come in soon enough, it progresses to a sharp pain. The con- versations usually go something like this: “Doc, this pain in my butt is killing me. I can’t run up hills, I can’t bike with any power, and every time I do anything hard, it grabs me.” Pain in the butt, otherwise known as a prox- imal hamstring strain, is a nagging injury that deserves immediate attention. Like most ath- letes, triathletes will often wait until it’s broken, really broken, before coming to the doctor. The hamstring, however, is one injury that needs to be taken seriously as soon as it starts to hurt. (Incidentally, this “wait until it doesn’t work” approach is more prevalent in men, who gen- erally wait until a body part is falling off before they come to the doctor, but women have been known to do it also.) The hamstring muscles—the biceps ahooMedia.com femoris, semitendinosus and semimembra- nosus—are a group of three muscles that come off of the ischial tueberosity, otherwise known John Segesta / W as the “sit bones,” at the base of the pelvis. Like several muscle groups in the body, the The proximal hamstring, however, the top the injury does not heal, ultrasound or MRI can hamstrings actually cross two joints, the hip of the muscles that comes off ischium, has a ter- be used to look for a partial tear, one of the more and the knee, inserting on the inside and the rible blood supply and heals very slowly. -

Proximal Hamstring Repair – Surgical Technique
Proximal hamstring repair – surgical technique Lasse Lempainen Hospital Mehiläinen NEO, Turku, Finland Correspondence: Lasse Lempainen, MD, PhD Adjunct professor, orthopaedic surgeon Hospital Mehiläinen NEO Joukahaisenkatu 6 FI-20520 Turku, Finland Email: [email protected], [email protected] Abstract Proximal hamstring injuries are common in athletes. Surgical indications are based on to regain the pre-injury activity level of the athlete. The key to achieve athletes back to play is to understand that hamstrings consist of three different muscles which have different functions. The rupture of proximal hamstring tendon can occur to one, two or all of these three tendons (semitendinosus, semimembranosus and biceps femoris) which may result to disabling and chronic pain with unable to fully participate to competitive sports. Surgery with open technique provides good visibility to hamstring tendons, nervous structures and bony insertion landmarks. This chapter gives the reader the indications for proximal hamstring tendon avulsion surgery together with the surgical technique and post-operative rehabilitation. We also discuss possible complications of the operative treatment. Keywords: hamstring injury, tendon avulsion, open surgery, surgical technique, rehabilitation Introduction Hamstring injuries can occur in various sports activities but also among regular people eg while falling down. These injuries can be highly disabling and they can lead to substantial time loss from sports (Harris et al, 2011). Some of the hamstring injuries require surgical treatment for optimal recovery (Lempainen 2015). Various open surgery techniques have been presented in literature (Lempainen 2006, Pombo & Bradley, 2009; Cohen et al, 2012; Sarimo et al, 2008; Birmingham et al, 2011; Carmichael et al, 2009; Moatshe et al, 2017). -

Influence of Hamstring, Glutes and Piriformis Muscle Health on Low Back Pain Sheetal Naik* Received: Department of Physiotherapy, Sikkim Manipal University/Drs
Acta Scientific Orthopaedics (ISSN: 2581-8635) Volume 4 Issue 3 March 2021 Commentary Influence of Hamstring, Glutes and Piriformis Muscle Health on Low Back Pain Sheetal Naik* Received: Department of Physiotherapy, Sikkim Manipal University/Drs. Nicolas and ASP, UAE Published: January 25, 2021 *Corresponding Author: Sheetal Naik. February 16, 2021 Sheetal Naik, Department of Physiotherapy, Sikkim © All rights are reserved by Manipal University/Drs. Nicolas and ASP, UAE. Abstract Flexibility and Strength are key factors to a muscle’s health. They are important for normal biomechanical function. The purpose ofKeywords: this article is to highlight the importance of Hamstring, Glutes and Piriformis health on Low back pain cases. Hamstring Tightness; Piriformis Syndrome; Glutes Tightness; Strengthening; Stretching; Low Back Pain Abbreviations if they exercise, it’s more of yes I go for walks or I am a housewife and so I am always active throughout the day. So how do the above Introductionopd: Outpatient Department; doc: Doctor. mentioned sentences dictate why you are getting this pain? Let us get into the technical aspect of it. Low back pain is a very commonly experienced condition with almost 8 out of 10 people experiencing it at some point of their Starting with Hamstrings, “The hamstrings are a group of four life. It is safe to say, that, as someone who has had the privilege muscles (long head of the biceps femoris, short head of the biceps of treating wide variety of patient cases, low back pain comprises femoris, semitendinosus, and semimembranosus) that originate on nearly 50% of any opd patient load. Lower back pain can often be a the bottom of the pelvis, the sitting bones, and insert over the knee result of soft tissue impairments surrounding and supporting the on the tibia or fibula.