Scapular Winging Is a Rare Disorder Often Caused by Neuromuscular Imbalance in the Scapulothoracic Stabilizer Muscles
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Chapter 30 When It Is Not Cervical Radiculopathy: Thoracic Outlet Syndrome—A Prospective Study on Diagnosis and Treatment
Chapter 30 When it is Not Cervical Radiculopathy: Thoracic Outlet Syndrome—A Prospective Study on Diagnosis and Treatment J. Paul Muizelaar, M.D., Ph.D., and Marike Zwienenberg-Lee, M.D. Many neurosurgeons see a large number of patients with some type of discomfort in the head, neck, shoulder, arm, or hand, most of which are (presumably) cervical disc problems. When there is good agreement between the history, physical findings, and imaging (MRI in particular), the diagnosis of cervical disc disease is easily made. When this agreement is less than ideal, we usually get an electromyography (EMG), which in many cases is sufficient to confirm cervical radiculopathy or establish another diagnosis. However, when an EMG does not provide too many clues as to the cause of the discomfort, serious consideration must be given to other painful syndromes such as thoracic outlet syndrome (TOS) and some of its variants, occipital or C2 neuralgia, tumors of or affecting the brachial plexus, and orthopedic problems of the shoulder (Table 30.1). Of these, TOS is the most controversial and difficult to diagnose. Although the neurosurgeons Adson (1–3) and Naffziger (10,11) are well represented as pioneers in the literature on TOS, this condition has received only limited attention in neurosurgical circles. In fact, no original publication in NEUROSURGERY or the Journal of Neurosurgery has addressed the issue of TOS, except for an overview article in NEUROSURGERY (12). At the time of writing of this paper, two additional articles have appeared in Neurosurgery: one general review article and another strictly surgical series comprising 33 patients with a Gilliatt-Sumner hand (7). -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
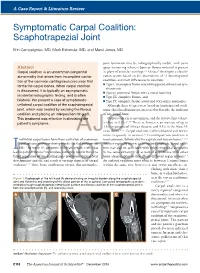
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -

Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies
Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies Zachary Simmons, MD* KEYWORDS Brachial plexus Brachial plexopathy Axillary nerve Musculocutaneous nerve Suprascapular nerve Nerve conduction studies Electromyography KEY POINTS The brachial plexus provides all motor and sensory innervation of the upper extremity. The plexus is usually derived from the C5 through T1 anterior primary rami, which divide in various ways to form the upper, middle, and lower trunks; the lateral, posterior, and medial cords; and multiple terminal branches. Traction is the most common cause of brachial plexopathy, although compression, lacer- ations, ischemia, neoplasms, radiation, thoracic outlet syndrome, and neuralgic amyotro- phy may all produce brachial plexus lesions. Upper extremity mononeuropathies affecting the musculocutaneous, axillary, and supra- scapular motor nerves and the medial and lateral antebrachial cutaneous sensory nerves often occur in the context of more widespread brachial plexus damage, often from trauma or neuralgic amyotrophy but may occur in isolation. Extensive electrodiagnostic testing often is needed to properly localize lesions of the brachial plexus, frequently requiring testing of sensory nerves, which are not commonly used in the assessment of other types of lesions. INTRODUCTION Few anatomic structures are as daunting to medical students, residents, and prac- ticing physicians as the brachial plexus. Yet, detailed understanding of brachial plexus anatomy is central to electrodiagnosis because of the plexus’ role in supplying all motor and sensory innervation of the upper extremity and shoulder girdle. There also are several proximal upper extremity nerves, derived from the brachial plexus, Conflicts of Interest: None. Neuromuscular Program and ALS Center, Penn State Hershey Medical Center, Penn State College of Medicine, PA, USA * Department of Neurology, Penn State Hershey Medical Center, EC 037 30 Hope Drive, PO Box 859, Hershey, PA 17033. -

Neuroanatomy for Nerve Conduction Studies
Neuroanatomy for Nerve Conduction Studies Kimberley Butler, R.NCS.T, CNIM, R. EP T. Jerry Morris, BS, MS, R.NCS.T. Kevin R. Scott, MD, MA Zach Simmons, MD AANEM 57th Annual Meeting Québec City, Québec, Canada Copyright © October 2010 American Association of Neuromuscular & Electrodiagnostic Medicine 2621 Superior Drive NW Rochester, MN 55901 Printed by Johnson Printing Company, Inc. AANEM Course Neuroanatomy for Nerve Conduction Studies iii Neuroanatomy for Nerve Conduction Studies Contents CME Information iv Faculty v The Spinal Accessory Nerve and the Less Commonly Studied Nerves of the Limbs 1 Zachary Simmons, MD Ulnar and Radial Nerves 13 Kevin R. Scott, MD The Tibial and the Common Peroneal Nerves 21 Kimberley B. Butler, R.NCS.T., R. EP T., CNIM Median Nerves and Nerves of the Face 27 Jerry Morris, MS, R.NCS.T. iv Course Description This course is designed to provide an introduction to anatomy of the major nerves used for nerve conduction studies, with emphasis on the surface land- marks used for the performance of such studies. Location and pathophysiology of common lesions of these nerves are reviewed, and electrodiagnostic methods for localization are discussed. This course is designed to be useful for technologists, but also useful and informative for physicians who perform their own nerve conduction studies, or who supervise technologists in the performance of such studies and who perform needle EMG examinations.. Intended Audience This course is intended for Neurologists, Physiatrists, and others who practice neuromuscular, musculoskeletal, and electrodiagnostic medicine with the intent to improve the quality of medical care to patients with muscle and nerve disorders. -

Scapular Winging Secondary to Apparent Long Thoracic Nerve Palsy in a Young Female Swimmer
THIEME Case Report e57 Scapular Winging Secondary to Apparent Long Thoracic Nerve Palsy in a Young Female Swimmer Shiro Nawa1 1 Department of Judo Seifuku and Health Sciences, Faculty of Health Address for correspondence Shiro Nawa, MS, Department of Judo Promotional Sciences, Tokoha University, Hamamatsu City, Seifuku and Health Sciences, Faculty of Health Promotional Sciences, Shizuoka-ken, Japan Tokoha University, 1230 Miyakoda-cho, Kita-ku, Hamamatsu City, Shizuoka-ken, 431-2102, Japan J Brachial Plex Peripher Nerve Inj 2015;10:e57–e61. (e-mail: [email protected]). Abstract Background In neurological diseases, winging of the scapula occurs because of serratus anterior muscle dysfunction due to long thoracic nerve palsy, or trapezius muscle dysfunction due to accessory nerve palsy. Several sports can cause long thoracic nerve palsy, including archery and tennis. To our knowledge, this is the first report of long thoracic nerve palsy in an aquatic sport. Objective The present study is a rare case of winging of the scapula that occurred during synchronized swimming practice. Methods The patient’s history with the present illness, examination findings, rehabili- tation progress, and related medical literature are presented. Keywords Results A 14-year-old female synchronized swimmer had chief complaints of muscle ► winging of the weakness, pain, and paresthesia in the right scapula. Upon examination, marked scapula winging of the scapula appeared during anterior arm elevation, as did floating of the ► accessory nerve palsy superior angle. After 1 year of therapy, right shoulder girdle pain and paresthesia had ► long thoracic nerve disappeared; however, winging of the scapula remained. palsy Conclusions Based on this observation and the severe pain in the vicinity of the second ► synchronized dorsal rib, we believe the cause was damage to the nerve proximal to the branch arising swimming from the upper nerve trunk that innervates the serratus anterior. -

Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon)
Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon) Mark A. Vitale, MD, MPHa, Fraser Taylor, MB, BS, FRACSb,c, Mark Ross, MB, BS, FRACSb,c,d, Steven L. Moran, MDe,* KEYWORDS Thumb Trapezial-metacarpal (TM) joint Silicone Artelon Pyrocarbon Total joint arthroplasty KEY POINTS Trapezium prosthetic arthroplasty has been used to treat basal joint arthritis for nearly 5 decades. Implant arthroplasty seeks to preserve joint biomechanics, avoid metacarpal subsidence, and provide immediate stability. There has been rapid development of trapezial prosthetic implants, including synthetic interposition materials, metal total joint arthroplasties and pyrocarbon trapezial arthroplasties. While many recently available implants have been shown to have short-term success, determining the medium- to long-term outcomes require further study. INTRODUCTION method has specific advantages and disadvan- tages for the surgeon to consider. The basal joint of the thumb is the second most 1 In contrast to ablative resection and joint fusion commonly affected joint by arthritis. Degenerative procedures, which sacrifice function of the basal disease of this joint can result in significant pain, joint in an effort to provide pain relief, prosthetic ar- stiffness, weakness, and disability. Conservative throplasty offers the theoretic advantages of pres- measures, such as nonsteroidal anti-inflammatory ervation of normal anatomy and biomechanics. drugs, splinting, and intra-articular corticosteroid This could be accomplished without subsidence injections, can provide relief for some patients; for of the thumb metacarpal, with preservation of those with severe disease in whom nonoperative normal motion at the trapezialmetacarpal (TM) measures fail, many surgical methods are available, joint, prevention of metacarpophalangeal joint with successful outcomes reported in the literature. -

Trapeziectomy
Trapeziectomy What is arthritis of the Trapeziometacarpal symptoms are. You can avoid certain activities joint? that cause you pain or take painkillers. Your The Trapezium is a small wrist bone that lies at hand therapist can provide or make splints for the base of your thumb. It is commonly affected you to rest your thumb in. Your doctor may also by wear and tear, otherwise known as arthritis. inject the joint with steroid (cortisone). This can be done under ultrasound or X-ray guidance Your surgeon has recommended an operation usually on a different day from the outpatient called trapeziectomy. It is the removal of this appointment. The injection only provides bone. However, it is your decision to go ahead temporary relief of symptoms (3-6 months) with the operation or not. or may not be successful at all. Repeated This leaflet gives you information about the injections often last a shorter duration each benefits and risks to help you to make an time. They do not cure the condition. informed decision. If you have any questions Surgical options: this leaflet does not answer, please ask your surgeon or the healthcare team. 1. Trapieziectomy – This is where the bone is removed completely. The gap fills with scar There is more than one way this surgery is tissue on which your thumb will sit to reduce carried out and if you research the internet you the pain of the bone on bone rubbing. will find a lot of information about it, some of 85% of patients have a significant pain which may not be relevant to you. -

Arthritis of the Base of the Thumb
Arthritis of the Base of the Thumb What is it? How is the diagnosis made? In a normal joint, cartilage covers the end of the bones and serves as a The diagnosis is made by history and physical evaluation. Pressure and shock absorber to allow smooth, pain-free movement. In osteoarthritis (OA, movement such as twisting will produce pain at the joint. A grinding or “degenerative arthritis”) the cartilage layer wears out, resulting in direct sensation may also be present at the joint (see Figure 3). X-rays are contact between the bones and producing pain and deformity. One of the used to confirm the diagnosis, although symptom severity often does not most common joints to develop OA in the hand is the base of the thumb. correlate with x-ray findings. The thumb basal joint, also called the carpometacarpal (CMC) joint, is a specialized saddle-shaped joint that is formed by a small bone of the wrist What are the treatment options? (trapezium) and the first bone of the thumb (metacarpal). The saddle shaped Less severe thumb arthritis will usually respond to non-surgical care. joint allows the thumb to have a wide range of motions, including up, down, Arthritis medication, splinting and limited cortisone injections may help across the palm, and the ability to pinch (see Figure 1). alleviate pain. A hand therapist might provide a variety of rigid and non-rigid splints which can be used while sleeping or during activities. Figure 1: Thumb Basal Joint Patients with advanced disease or who fail non-surgical treatment may be candidates for surgical reconstruction. -

Upper Limb 3 the Wrist
Upper Limb 3 The Wrist Donald Sammut Hand Surgeon Kings Upper Limb Anatomy plus lecture notes • Unlike'many'other'joints,'the'wrist'surface'anatomy'gives'away'little'of' the'bony'structures'beneath'the'surface.' • Still'less'does'it'suggest'the'complex'ligament'structures' Carpus' Radius' Ulna' • The'wrist'is'surrounded'by'vital'structures,'tendons,'nerves,'arteries.'' • Pathology'in'these'structures'can'give'symptoms'mistaken'for'problems' with'the'wrist'joint' • 8'wrist'bones'form'the'carpus.' • Proximally'these'articulate'with'the'radius' • Distally'they'articulate'with'the'metacarpals.' • The'carpal'bones'articulate'with'each'other'in'a'particular'configuration'of' bony'shapes'and'ligaments'which'dictate'the'complex'function.' Trapezoid' Capitate' Trapezium' Hamate' Scaphoid' Pisiform' Lunate' Triquetral' • Proximally'the'carpus'articulates'with'the'distal'radius'and'with'the' triangular'fibrocartilage.' • The'TFC'separates'the'carpus'from'the'ulna' • The'distal'ulna'does'not'participate'in'the'articulation'with'the'carpus' • View'of'the'distal'radius.'Proximal'aspect'of'the'RadioKcarpal'joint' • Note'' 'the'Scaphoid'fossa' 'the'Lunate'fossa' 'the'triangular'fibrocartilage' PROXIMAL)ARTICULAR)SURFACE)OF)THE)WRIST:)RADIUS'AND'TRIANGULAR'CARTILAGE' ' THE'ULNA'IS'EXCLUDED.' • Distal'aspect'of'the'RadioKcarpal'joint' The'radius'and'triangular'fibrocartilage'articulate'with'the'scaphoid,'lunate' and'triquetral' DISTAL)ARTICULAR)SURFACE)OF)THE)WRIST:)SCAPHOID,'LUNATE','TRIQUETRAL' ' • The'bony'shapes'of'the'radiocarpal'joint'make'for'an'unstable'arrangement'