Asymmetry of the Humerus: the Influence of Handedness on the Deltoid Tuberosity and Possible Implications for Osteometric Sorting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

By the Authors. These Guidelines Will Be Usefulas an Aid in Diagnosing
Kroeber Anthropological Society Papers, Nos. 71-72, 1990 Humeral Morphology of Achondroplasia Rina Malonzo and Jeannine Ross Unique humeral morphologicalfeatures oftwo prehistoric achondroplastic adult individuals are des- cribed. Thesefeatures are compared to the humerus ofa prehistoric non-achondroplastic dwarfand to the humeri ofa normal humanpopulation sample. A set ofunique, derived achondroplastic characteris- tics ispresented. The non-achondroplastic individual is diagnosed as such based on guidelines created by the authors. These guidelines will be useful as an aid in diagnosing achondroplastic individualsfrom the archaeological record. INTRODUCTION and 1915-2-463) (Merbs 1980). The following paper describes a set of humeral morphological For several decades dwarfism has been a characteristics which can be used as a guide to prominent topic within the study of paleopathol- identifying achondroplastic individuals from the ogy. It has been represented directly by skeletal archaeological record. evidence and indirectly by artistic representation in the archaeological record (Hoffman and Brunker 1976). Several prehistoric Egyptian and MATERIALS AND METHODS Native American dwarfed skeletons have been recorded, indicating that this pathology is not A comparative population sample, housed by linked solely with modem society (Brothwell and the Lowie Museum of Anthropology (LMA) at Sandison 1967; Hoffman and Brunker 1976; the University of California at Berkeley, was Niswander et al. 1975; Snow 1943). Artifacts derived from a random sample forming a total of such as paintings, tomb illustrations and statues sixty adult individuals (thirty males and thirty of dwarfed individuals have been discovered in females) from six different prehistoric ar- various parts of the world. However, interpreta- chaeological sites within California. Two tions of such artifacts are speculative, for it is achondroplastic adult individuals from similar necessary to allow artistic license for individualis- contexts, specimen number 6670 (spc. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -
Bones of the Upper and Lower Limb Musculoskeletal Block - Lecture 1
Bones of the Upper and Lower limb Musculoskeletal Block - Lecture 1 Objective: Classify the bones of the three regions of the lower limb (Thigh, leg and foot). Memorize the main features of the – Bones of the thigh (femur & patella) – Bones of the leg (tibia & Fibula) – Bones of the foot (tarsals, metatarsals and phalanges) Recognize the side of the bone. Color index: Important In male’s slides only In female’s slides only Extra information, explanation Editing file Click here for Contact us: useful videos [email protected] Please make sure that you’re familiar with these terms Terms Meaning Example Ridge The long and narrow upper edge, angle, or crest of something The supracondylar ridges (in the distal part of the humerus) Notch An indentation, (incision) on an edge or surface The trochlear notch (in the proximal part of the ulna) Tubercles A nodule or a small rounded projection on the bone (Dorsal tubercle in the distal part of the radius) Fossa A hollow place (The Notch is not complete but the fossa is Subscapular fossa (in the concave part of complete and both of them act as the lock of the joint the scapula) Tuberosity A large prominence on a bone usually serving for Deltoid tuberosity (in the humorous) and it the attachment of muscles or ligaments ( is a bigger projection connects the deltoid muscle than the Tubercle ) Processes A V-shaped indentation (act as the key of the joint) Coracoid process ( in the scapula ) Groove A channel, a long narrow depression sure Spiral (Radial) groove (in the posterior aspect of (the humerus -

Biceps Anatomical Aberration in a Cadaveric Study
CaseReport32 Indian Journalof Anatomy Volume 7Number 3, May -June 2018 DOI: http://dx.doi.org/10.21088/ija.2320.0022.7318.24 BicepsAnatomicalAberrationinaCadavericStudy ViayAnanth K. Abstract InaroutinecadavericdissectionsinacadavertheshortheadofBicepsBrachiitendon(SBT)showedbifurcated inattachmentwiththebellyofthePronatorTeresmuscleseenalongwithitsusualcourseofattachmentwiththe radialtuberosity. Thiswas seenbilaterally on boththe upperlimbs inthesame bodyduringthe anatomical dissection.erethebicepsbrachiiwasoriginatingfromthelongheadfromthesupraglenoidtuberclefromthe capusularjointandtheshortheadfromthecoracoidprocessofscapula. KeywordsBicepsBrachiiandPronatorTeresMuscleExtrarticularInsertionCadaver. Introduction Intheupperextremitytheanteriorcompartment formstheflexorgroupmusclesofwhichalongwith thecoracobrachialistheBicepsBrachiiplaysamajor roleinflexingthearmsandtheelbowjoint.It compensatestheactionwiththeTricepsBrachiithe posteriorcompartmentmuscleofthebrachiumwhich formstheextensors. Itisalargefusiformmuscleofthatcompartment 3,8andaprimarysupinatoroftheforearm.Biceptal aponeurosis,atriangularbandformedfromthedeep fasciaoriginatesfromthebicepstendon.This aponeurosisgivesprotectiontothecubitalfossa.A thirdhead is also reportedseen posterior to the brachialartery8. Itoriginatesfromlongandshortheadsfrom supraglenoidtubercleandcoracoidsprocessof scapularespectively. Andboththeheadsconvergewiththetwobelles andgetsinsertedintotheposteriorpartofthe tuberosityofradiusbone9. Fi.Rt.SideArm Authors AffiliationLecturer,DepartmentofAnatomy, igure1showsBicepsBrachiiinthefrontof -

Options of Bipolar Muscle Transfers to Restore Deltoid Function: an Anatomical Study
Surgical and Radiologic Anatomy (2019) 41:911–919 https://doi.org/10.1007/s00276-018-2159-1 ORIGINAL ARTICLE Options of bipolar muscle transfers to restore deltoid function: an anatomical study Malo Le Hanneur1,2 · Julia Lee1,3 · Eric R. Wagner1,4 · Bassem T. Elhassan1 Received: 2 June 2018 / Accepted: 8 December 2018 / Published online: 12 December 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract Purpose To outline the technical details and determine the ranges of two pedicled functioning flaps that are the upper pec- toralis major (UPM) and latissimus dorsi (LD) to elucidate their respective indications with regards to deltoid impairment. Methods The UPM and LD bipolar transfers were performed in 14 paired cadaveric shoulders, one on each side. The UPM was flipped 180° laterally over its pedicle to be placed onto the anterior deltoid. The LD flap was elevated on its pedicle to be rotated and positioned onto the deltoid mid-axis. Their respective spans were defined according to the deltoid muscle origin and insertion. Results The UPM outreached the lateral edge of the anterior deltoid origin with a mean distance of 7.3 cm (range 4–9.1 cm) off the lateral edge of the clavicle. Distally, the flap consistently overcame the proximal end of the deltoid tuberosity for a mean distance of 2.1 cm (range 0.9–3.2 cm). The LD flap mdi-axis could be consistently placed onto the deltoid mid-axis; spans of the anterior and posterior borders of the LD flap averaged 1 cm (range − 1 to 2.3 cm) and 0.2 cm (range −1.8 to 1.9 cm), respectively. -

The Anatomy of the Bicipital Tuberosity and Distal Biceps Tendon
The anatomy of the bicipital tuberosity and distal biceps tendon Augustus D. Mazzocca, MD,a Mark Cohen, MD,b Eric Berkson, MD,b Gregory Nicholson, MD,b Bradley C. Carofino, MD,a Robert Arciero, MD,a and Anthony A. Romeo, MDb Farmington, CT, and Chicago, IL The anatomy of the distal biceps tendon and bicipi- and the mean BT-radial styloid angle is 123° Ϯ 10°. tal tuberosity (BT) is important in the pathophysiol- None of the measurements correlated with patient ogy of tendon rupture, as well as surgical repair. age, sex, or race. We concluded that the morphology Understanding the dimensions of the BT and its an- of the BT ridge is variable. The insertion footprint of gular relationship to the radial head and radial the distal biceps tendon is on the ulnar aspect of the styloid will facilitate surgical procedures such as re- BT ridge. The dimensions of the radius and BT are ap- construction of the distal biceps tendon, radial head plicable to several surgical procedures about the el- prosthesis implantation, and reconstruction of proxi- bow. (J Shoulder Elbow Surg 2007;16:122-127.) mal radius trauma. We examined 178 dried cadav- eric radii, and the following measurements were col- The recognition and treatment of distal biceps ten- lected: radial length, length and width of the BT, don ruptures have increased over time. Previously, diameter of the radius just distal to the BT, distance this injury was considered rare; only 65 cases were from the radial head to the BT, radial head diame- reported before 1941.2,4 However, a more recent ter, width of the radius at the BT, radial neck-shaft retrospective study identified the incidence to be 1.2 10 angle, and styloid angle. -
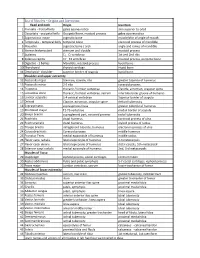
List of Muscles – Origins and Insertions
List of Muscles – Origins and Insertions: Head and neck Origin Insertion 1 Frontalis - frontal belly galea aponeurotica skin superior to orbit 2 Occipitalis - occipetal belly Occipetal bone, mastoid process galea aponeurotica 3 Zygomaticus major zygmatic bone muscle/skin of angle of mouth 4 Temporalis - temporal belly temporal bone coronoid process of mandible 5 Masseter zygmatic bone / arch angle and ramus of mandible 6 Sternocleidomastoid sternum and clavicle mastoid process 7 Scalenes C3 - C7 vertebrae 1st and 2nd ribs 8 Splenius capitis C7 - T4 vertebrae mastoid process, occipetal bone 9 Digastric - 2 bellies Mandible, mastoid process hyoid bone 10 Thyrohyoid thyroid cartilage Hyoid bone 11 Omohyoid - shoulder superior border of scapula hyoid bone Shoulder and upper extremity 12 Pectoralis major Sternum, clavicle, ribs greater tubercle of humerus 13 Pectoralis minor 2-5 ribs coracoid process 14 Trapezius thoracic / lumbar vertebrae Clavicle, acromion, scapular spine 15 Latissimus dorsi thoracic / lumbar vertebrae, sacrum intertubercular groove of humerus 16 Levator scapulae 1-4 cervical vertebrae Superior border of scapula 17 Deltoid Clavicle, acromion, scapular spine deltoid tuberosity 18 Supraspinatus supraspinous fossa greater tubercle of humerus 19 Rhomboid major T2-T5 vertebrae medial border of scapula 20 Biceps brachii supraglenoid part, coracoid process radial tuberosity 21 Brachialis distal humerus coronoid process of ulna 22 Brachioradialis distal humerus styloid process of radius 23 Triceps brachii infraglenoid tubercle, -

Muscles of the Upper Limb.Pdf
11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles of the Upper Limb Pectoralis minor ORIGIN: INNERVATION: anterior surface of pectoral nerves ribs 3 – 5 ACTION: INSERTION: protracts / depresses scapula coracoid process (scapula) (Anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Serratus anterior Subclavius ORIGIN: INNERVATION: ORIGIN: INNERVATION: ribs 1 - 8 long thoracic nerve rib 1 ---------------- INSERTION: ACTION: INSERTION: ACTION: medial border of scapula rotates scapula laterally inferior surface of scapula stabilizes / depresses pectoral girdle (Lateral view) (anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Trapezius Levator scapulae ORIGIN: INNERVATION: ORIGIN: INNERVATION: occipital bone / spinous accessory nerve transverse processes of C1 – C4 dorsal scapular nerve processes of C7 – T12 ACTION: INSERTION: ACTION: INSERTION: stabilizes / elevates / retracts / upper medial border of scapula elevates / adducts scapula acromion / spine of scapula; rotates scapula lateral third of clavicle (Posterior view) (Posterior view) 1 11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles Moving Arm Rhomboids Pectoralis major (major / minor) ORIGIN: INNERVATION: ORIGIN: INNERVATION: spinous processes of C7 – T5 dorsal scapular nerve sternum / clavicle / ribs 1 – 6 dorsal scapular nerve INSERTION: ACTION: INSERTION: ACTION: medial border of scapula adducts / rotates scapula intertubucular sulcus / greater tubercle flexes / medially rotates / (humerus) adducts -

RADIOULNAR JOINTS the Radius and Ulna Articulate by –
RADIOULNAR JOINTS The radius and ulna articulate by – • Synovial 1. Superior radioulnar joint 2. Inferior radioulnar joint • Non synovial Middle radioulnar union Superior Radioulnar Joint This articulation is a trochoid or pivot-joint between • the circumference of the head of the radius • ring formed by the radial notch of the ulna and the annular ligament. The Annular Ligament (orbicular ligament) This ligament is a strong band of fibers, which encircles the head of the radius, and retains it in contact with the radial notch of the ulna. It forms about four-fifths of the osseo- fibrous ring, and is attached to the anterior and posterior margins of the radial notch a few of its lower fibers are continued around below the cavity and form at this level a complete fibrous ring. Its upper border blends with the capsule of elbow joint while from its lower border a thin loose synovial membrane passes to be attached to the neck of the radius The superficial surface of the annular ligament is strengthened by the radial collateral ligament of the elbow, and affords origin to part of the Supinator. Its deep surface is smooth, and lined by synovial membrane, which is continuous with that of the elbow-joint. Quadrate ligament A thickened band which extends from the inferior border of the annular ligament below the radial notch to the neck of the radius is known as the quadrate ligament. Movements The movements allowed in this articulation are limited to rotatory movements of the head of the radius within the ring formed by the annular ligament and the radial notch of the ulna • rotation forward being called pronation • rotation backward, supination Middle Radioulnar Union The shafts of the radius and ulna are connected by Oblique Cord and Interosseous Membrane The Oblique Cord (oblique ligament) The oblique cord is a small, flattened band, extending downward and laterally, from the lateral side of the ulnar tuberosity to the radius a little below the radial tuberosity. -

Functional Anatomy of the Shoulder Glenn C
Journal ofAthletic Training 2000;35(3):248-255 C) by the National Athletic Trainers' Association, Inc www.journalofathletictraining.org Functional Anatomy of the Shoulder Glenn C. Terry, MD; Thomas M. Chopp, MD The Hughston Clinic, Columbus, GA Objective: Movements of the human shoulder represent the nents. Bony anatomy, including the humerus, scapula, and result of a complex dynamic interplay of structural bony anat- clavicle, is described, along with the associated articulations, omy and biomechanics, static ligamentous and tendinous providing the clinician with the structural foundation for under- restraints, and dynamic muscle forces. Injury to 1 or more of standing how the static ligamentous and dynamic muscle these components through overuse or acute trauma disrupts forces exert their effects. Commonly encountered athletic inju- this complex interrelationship and places the shoulder at in- ries are discussed from an anatomical standpoint. creased risk. A thorough understanding of the functional anat- Conclusions/Recommendations: Shoulder injuries repre- omy of the shoulder provides the clinician with a foundation for sent a significant proportion of athletic injuries seen by the caring for athletes with shoulder injuries. medical provider. A functional understanding of the dynamic Data Sources: We searched MEDLINE for the years 1980 to interplay of biomechanical forces around the shoulder girdle is 1999, using the key words "shoulder," "anatomy," "glenohu- necessary and allows for a more structured approach to the meral joint," "acromioclavicular joint," "sternoclavicular joint," treatment of an athlete with a shoulder injury. "scapulothoracic joint," and "rotator cuff." Key Words: anatomy, static, dynamic, stability, articulation Data Synthesis: We examine human shoulder movement by breaking it down into its structural static and dynamic compo- M ovements of the human shoulder represent a complex BONY ANATOMY dynamic relationship of many muscle forces, liga- ment constraints, and bony articulations. -

Shoulder Anatomy
ShoulderShoulder AnatomyAnatomy www.fisiokinesiterapia.biz ShoulderShoulder ComplexComplex BoneBone AnatomyAnatomy ClavicleClavicle – Sternal end – Acromion end ScapulaScapula Acromion – Surfaces end Sternal Costal end Dorsal – Borders – Angles ShoulderShoulder ComplexComplex BoneBone AnatomyAnatomy Scapula 1. spine 2. acromion 3. superior border 4. supraspinous fossa 5. infraspinous fossa 6. medial (vertebral) border 7. lateral (axillary) border 8. inferior angle 9. superior angle 10. glenoid fossa (lateral angle) 11. coracoid process 12. superior scapular notch 13 subscapular fossa 14. supraglenoid tubercle 15. infraglenoid tubercle ShoulderShoulder ComplexComplex BoneBone AnatomyAnatomy HumerousHumerous – head – anatomical neck – greater tubercle – lesser tubercle – greater tubercle – lesser tubercle – intertubercular sulcus (AKA bicipital groove) – deltoid tuberosity ShoulderShoulder ComplexComplex BoneBone AnatomyAnatomy HumerousHumerous – Surgical Neck – Angle of Inclination 130-150 degrees – Angle of Torsion 30 degrees posteriorly ShoulderShoulder ComplexComplex ArticulationsArticulations SternoclavicularSternoclavicular JointJoint – Sternal end of clavicle with manubrium/ 1st costal cartilage – 3 degree of freedom – Articular Disk – Ligaments Capsule Anterior/Posterior Sternoclavicular Ligament Interclavicular Ligament Costoclavicular Ligament ShoulderShoulder ComplexComplex ArticulationsArticulations AcromioclavicularAcromioclavicular JointJoint – 3 degrees of freedom – Articular Disk – Ligaments Superior/Inferior