EAHL Newsletter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Official Site, Telegram, Facebook, Instagram, Instamojo
Page 1 Follow us: Official Site, Telegram, Facebook, Instagram, Instamojo All SUPER Current Affairs Product Worth Rs 1200 @ 399/- ( DEAL Of The Year ) Page 2 Follow us: Official Site, Telegram, Facebook, Instagram, Instamojo SUPER Current Affairs MCQ PDF 3rd August 2021 By Dream Big Institution: (SUPER Current Affairs) © Copyright 2021 Q.World Sanskrit Day 2021 was celebrated on ___________. A) 3 August C) 5 August B) 4 August D) 6 August Answer - A Sanskrit Day is celebrated every year on Shraavana Poornima, which is the full moon day in the month of Shraavana in the Hindu calendar. In 2020, Sanskrit Day was celebrated on August 3, while in 2019 it was celebrated on 15 August. Sanskrit language is believed to be originated in India around 3,500 years ago. Q.Nikol Pashinyan has been re-appointed as the Prime Minister of which country? A) Ukraine C) Turkey B) Armenia D) Lebanon Answer - B Nikol Pashinyan has been re-appointed as Armenia’s Prime Minister by President Armen Sarkissian. Pashinyan was first appointed as the prime minister in 2018. About Armenia: Capital: Yerevan Currency: Armenian dram President: Armen Sargsyan Page 3 Follow us: Official Site, Telegram, Facebook, Instagram, Instamojo Q.Min Aung Hlaing has taken charge as the Prime Minister of which country? A) Bangladesh C) Thailand B) Laos D) Myanmar Answer - D The Chief of the Myanmar military, Senior General Min Aung Hlaing has taken over as the interim prime minister of the country on August 01, 2021. About Myanmar Capital: Naypyitaw; Currency: Kyat. NEWLY Elected -

Compassionate and Visionary Leadership. Key Lessons of Social Democratic Governance in Times of Covid-19
PROGRESS IN EUROPE 31 Compassionate and visionary leadership Key lessons of Social Democratic governance in times of Covid-19 Ania Skrzypek The Covid-19 pandemic has triggered an unforeseen reaction from European citizens. People – the same people that until a year ago were very vocal in expressing their mistrust in politics and institutions – instinctively turned to their national government to receive care and cure in a moment of deep crisis. Furthermore, they found a feeling of mutual solidarity, particularly in the fi rst stages of the lockdown, and naturally longed for a more robust welfare state. These are not changes that one can consider permanent or long-term. Yet they have had signifi cant implications for politics and for political parties, and for the Social Democratic ones in particular, which are strongly committed to values such as solidarity, and have traditionally been cham- pions of the European welfare states. The new public mood has allowed for welfare policies to be recognised as essential, that during the 2008 fi nancial crisis were considered simply too costly. What is more, the crisis has offered the opportunity for the Social Democratic parties in government to set the direction rather than merely manage the crisis. Empathy and com- munication focused on safeguarding jobs have become fundamental tools for establishing a connection with the European people. At the end of 2020 social media were fl ooded by memes that would immortalise the passing year as a complete disaster. The depiction varied with some suggesting ‘all down the drain’ and others implicitly offering the hope that from the absolute low in which the world had found itself, there was no other way but upwards. -

European Council 15-16 October 2020
OPTION 2 VARIATION FROM OPTION 1 > Using same grid to identity dierent types of patterns made up with lines BRUSSELS EUROPEAN COUNCIL 15-16 OCTOBER 2020 SWEDEN Stefan Löfven Prime Minister EUROPEAN COUNCIL Charles Michel President European Council EUROPEAN COMMISSION GERMANY Ursula von der Leyen President Angela Merkel Federal Chancellor EUROPEAN EXTERNAL ACTION SERVICE AUSTRIA Josep Borrell Fontelles Sebastian Kurz High Representative of the Union for Federal Chancellor Foreign Affairs and Security Policy GENERAL SECRETARIAT OF THE COUNCIL BELGIUM Jeppe Tranholm-Mikkelsen Alexander De Croo Secretary-General Prime Minister BULGARIA Boyko Borissov GUEST Prime Minister EUROPEAN PARLIAMENT CROATIA David Maria Sassoli Andrej Plenković President Prime Minister CYPRUS EUROPEAN COMMISSION Nicos Anastasiades Michel Barnier President of the Republic Chief Negotiator CZECHIA Andrej Babiš Prime Minister DENMARK Mette Frederiksen Prime Minister 12 october 2020 RS 292 2020 RS 292 2020 Trombino_151020.indd 1 14/10/2020 10:52:42 OPTION 2 VARIATION FROM OPTION 1 > Using same grid to identity dierent types of patterns made up with lines ÉIRE/IRELAND LUXEMBOURG Micheál Martin Xavier Bettel The Taoiseach Prime Minister ESTONIA MALTA Jüri Ratas Robert Abela Prime Minister Prime Minister FINLAND THE NETHERLANDS Sanna Marin Mark Rutte Prime Minister Prime Minister FRANCE POLAND Emmanuel Macron Mateusz Morawiecki President of the Republic Prime Minister GREECE PORTUGAL Kyriakos Mitsotakis António Costa Prime Minister Prime Minister HUNGARY ROMANIA Viktor Orbán Klaus Werner Iohannis Prime Minister President ITALY SLOVAKIA Giuseppe Conte Igor Matovič Prime Minister Prime Minister LATVIA SLOVENIA Krišjānis Kariņš Janez Janša Prime Minister Prime Minister LITHUANIA SPAIN Gitanas Nausėda Pedro Sánchez Pérez-Castejón President of the Republic Prime Minister RS 292 2020 Trombino_151020.indd 2 14/10/2020 10:52:54. -

Statement by H.E. Robert Abela, Prime Minister of Malta at the High
Statement by H.E. Robert Abela, Prime Minister of Malta at the High-level meeting to commemorate the seventy-fifth Anniversary of the United Nations Item 128(a) 21 September 2020 “The future we want, the United Nations we need: reaffirming our collective commitment to multilateralism” Secretary General, President of the General Assembly, Excellencies, Ladies and Gentlemen It is highly significant that at the moment the world is gripped by a global pandemic, we come together through virtual means, to celebrate the 75th Anniversary of the United Nations. In a matter of weeks, the pandemic manifested itself as the largest global challenge in the history of the United Nations. As the Final Declaration, which we endorse today, rightly states, ‘There is no other global organization with the legitimacy, convening power and normative impact as the United Nations. No other global organization gives hope to so many people for a better world and can deliver the future we want. The urgency for all countries to come together, to fulfill the promise of the nations united, has rarely been greater.’ Mr President, Today, the 21st September, Malta celebrates 56 years of Independence, but what is also noteworthy is that Malta became the 114th member of the United Nations Organisation on the 1st December 1964, only a few weeks after gaining Independence. On the raising of the flag the then Maltese Prime Minister, Dr George Borg Olivier, emphasized Malta’s position between East and West, Europe and Africa, and spoke of Malta’s aspirations for peaceful development. Now that Malta had taken her place among the free nations, the Prime Minister pledged Malta’s contribution towards world peace in that, ‘spirit of heroic determination, in defence of traditional concepts of freedom and civilisation’, which have characterized Malta’s long history. -

Executive Database 10 September 2020 Nb
EXECUTIVE DATABASE 10 SEPTEMBER 2020 NB: THIS DATABASE IS BASED ON INFORMATION RECEIVED FROM SA MISSIONS POLITICAL DESKS FOREIGN MISSIONS COUNTRY HEAD OF STATE DATE OF HEAD OF GOVERNMENT DATE OF MINISTER OF FOREIGN CAPITAL CITY INAUGURATION (PRIME MINISTER) APPOINTMENT AFFAIRS African Union HE Mr Matamela Cyril 12/02/2020 HE Mr Moussa Faki 14/03/2017 Addis Ababa (AU) Ramaphosa Mahamat Chairperson Chairperson of the African Union Commission0 Islamic Republic HE Mr Ashraf Ghani 29/09/2014 Chief Executive 29/09/2014 HE Haroon Kabul of Afghanistan Chakhansuri (acting) President Mr Abdullah Abdullah Minister of Foreign Affairs 23/01/2020 Republic of HE Mr Ilir Rexhep Metaj 24/07/2017 HE Mr Edi Rama 15/09/2013 HE Mr Edi Rama Tirana Albania President Prime Minister Prime Minister and Minister of Foreign Affairs 21/01/2019 Gent Cakaj Deputy Minister of Foreign Affairs (with full responsibility as a Minister) 22/01/2019 Democratic HE Mr Abdelmadjid Tebboune 19/12/2019 HE Mr Abdelaziz Djerad 28/12/2019 HE Ms Sabri Boukadoum Algiers People’s President Prime Minister presiding Minister of Foreign Affairs Republic of over the Council of and International Algeria Ministers Cooperation Head of Government 02/04/2019 Principality of HE Bishop Joan Enric VIVES I 16/05/2019 HE Mr Xavier Espot 17/07/2017 HE Mrs Maria Ubach Font Andorra La Andorra SICILIA Zamora Vella Minister of Foreign Affairs (Co-Prince of Andorra) Prime Minister (Letters to each HE Mr Emmanuel Macron Co-Prince) (Co-Prince of Andorra) Republic of HE Mr João Manuel 26/09/2017 HOS is -

Global Leaders'
u Agenda for the Global Leaders’ Day 1 Global Leaders’ Day 08 July 2020 u Event agenda Time Speaker 10.00 ILO DG opens the Global Summit (CEST) Mr Antonio GUTERRES, Secretary-General of the United Nations Dr Tedros Adhanom GHEBREYESUS, Director-General of the World Health Organization S.E. Mme Simonetta SOMMARUGA, Présidente de la Confédération suisse H.E. Mr MOON Jae-in, President of the Republic of Korea H.E. Mr Gotabaya RAJAPAKSA, President of the Democratic Socialist Republic of Sri Lanka Ms Sangita REDDY, President of the Federation of Indian Chambers of Commerce And Industry (FICCI) Mr Rikio KOZU, President, Japanese Trade Union Confederation (JTUC-RENGO) H.E. Mr Josaia Voreqe BAINIMARAMA, Prime Minister of the Republic of Fiji H.E. Sheikh HASINA, Prime Minister of the Government of the People's Republic of Bangladesh H.E. Mr Tuilaepa Lupe Sailele MALIELEGAOI, Prime Minister of the Independent State of Samoa H.E. General Prayut CHAN-O-CHA, Prime Minister of the Kingdom of Thailand H.E. Mr K. P. Sharma OLI, Prime Minister of the Federal Democratic Republic of Nepal H.E. Mr Imran KHAN, Prime Minister of the Islamic Republic of Pakistan H.E. Daw Aung San Suu KYI, State Counsellor of the Republic of the Union of Myanmar Ms Reema NANAVATY, Leader, Self Employed Women’s Association (SEWA), India Ms Kristalina GEORGIEVA, Managing Director of the International Monetary Fund Mr Roberto AZEVÊDO, Director-General of the World Trade Organization H.E. Mr Mohammad Ibrahim SHTAYYEH, Prime Minister of the Palestinian Authority Break for 10 minutes H.E. -

DIGITAL ENGAGEMENT REPORT 2021 European Center for Digital Competitiveness – Digital Engagement Report 2021
DIGITAL ENGAGEMENT REPORT 2021 European Center for Digital Competitiveness – Digital Engagement Report 2021 » Preface The Covid-19 pandemic has highlighted that digitalisation is one of the most critical issues faced by individuals, businesses and countries today. Whilst other nations – notably the United States and China – have capitalised on the crisis and now dominate key digital technologies more than ever before, Europe is increasingly lagging behind in terms of digitalisation and the development of a digital economy. Moreover, many European companies are still struggling not only with infrastructure topics, but also with key digital technologies such as quantum computing and robotics. Against this backdrop, the European Center for Digital Competitiveness by ESCP Business School in Berlin has published the Digital Engagement Report 2021. The report presents the digital engagement of all 27 European heads of state and government for the year 2020, including all interactions around digitalisation, based on publicly accessible government information, press releases and personal accounts on the social media platform Twitter. Heads of state and government play a crucial role in the successful digital transformation of their countries, and similar to CEOs, who are responsible for setting and implementing company strategy, these government leaders set the political agenda of their country and are ultimately responsible for their execution. Furthermore, the involvement of a government leader can signal the importance of an issue to his or her entire country, which in turn can inspire the actions of citizens, start-ups and incumbent businesses. The way that governments manage and navigate the digital revolution will continue to determine significantly how competitive and prosperous their countries will be in the decades ahead. -

Dear Madam President, Dear Ursula, As Heads of States And
20 April 2021 Dear Madam President, Dear Ursula, As Heads of States and Governments we have committed to the Paris Agreement and the climate neutrality of the EU and we are very firm in standing by you when accomplishing the European Green Deal. At the same time, we must insist that all important elements of it remain preserved, namely improving well-being of citizens and pursuing the just transition that leaves no one behind. In this respect, recent developments around the Commission proposals for the EU Taxonomy delegated act raise serious concerns among us. We are particularly worried about our right to decide on our energy mix in conditions where the rules for mobilization of private and public investments would clearly disadvantage some technologies, since the principle of technological neutrality is not respected to the extent that they constitute an indispensable element of the 2030 National Climate Energy Plans and they contribute to a significant decrease of GHG. Investment decisions being strongly affected may even result in substantial slowing down of the process of coal phase-out in some states and make us all much less fit for achieving climate-neutral Europe. The direction the delegated act preparation heads for is not right for our economies and it is not right for the EU's growth either. We firmly believe that the intention to put forward a separate legislative proposal specifically covering how certain economic activities, primarily in the energy sector, contribute to decarbonisation is contrary to the core of the Taxonomy Regulation – the principle of technological neutrality as well as the commitment to ensure that technical screening criteria are based on available scientific evidence. -
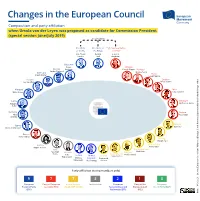
Changes in the European Council
Changes in the European Council Composition and party affiliation when Ursula von der Leyen was proposed as candidate for Commission President (special session June/July 2019) no voting rights President President of High Representative of the EC the EUCO of the EU Jean-Claude Donald Federica Juncker Tusk Mogherini Bulgarien Boyko Slovakia Croatia Borissow Peter Pellegrini Portugal Andrej Plenković António Costa Germany Malta Angela Merkel Joseph Muscat Ireland Sweden Leo Varadkar Stefan Löfven Hungary Spain Viktor Orbán Pedro Sánchez Latvia Denmark Krišjānis Mette Frederiksen Kariņš Romania Finland Sponsored by the Federal Foreign Office Klaus Antti Rinne | Johannis Estonia Cyprus Jüri Ratas Nicos Anastasiades Burak Korkmaz Greece Alexis Tsipras Design: Slovenia Marjan Šarec Austria Czech Republic Andrej Babiš Brigitte Bierlein Italy The Netherlands Giuseppe Lithuania Belgium Mark Rutte Conte Luxembourg Charles Michel Dalia Poland United France Grybauskaitė Xavier Bettel Mateusz Kingdom Emmanuel Morawiecki Theresa May Macron European Council and Wikipedia| Party affiliation (voting members only) | Source: | Source: 9 7 7 3 2 1 0 European Party of European Renew Europe - Independent European Party of the European People's Party Socialists (PES) (ALDE, EDP, LREM) Conservatives and European Left Green Party (EGP) 19/03/2021 (EPP) Reformists (ECR) (PEL) Date: Changes in the European Council Composition and party affiliation March 2021 no voting rights President President of High Representative of the EC the EUCO of the EU Ursula Charles Joseph von -

Country Position Name Email Twitter Andorra Prime Minister Mr
Country Position Name Email Twitter Andorra Prime Minister Mr. Xavier Espot Zamora [email protected] Twitter: GovernAndorra Minister of Foreign Affairs Mrs. Maria Ubach Font [email protected] Twitter:@mubachfont UN Ambassdor in New York H.E. Mrs. Elisenda Vives Balmaña [email protected] Twitter: @ANDORRA_UN UN Ambassdor in Geneva H.E. Mr. Joan Forner Rovira [email protected] Austria President Dr. Alexander Van der Bellen [email protected] Twitter: A. Van der Bellen Federal Chancellor Mr. Sebastian Kurz [email protected] Minister of Foreign Affairs Mr Alexander Schallenberg Twitter: MFA_Austria UN Ambassdor in New York H.E. Mr. Alexander Marchik Twitter: @AustriaUN Disarmament Ambassdor Mr Thomas HAJNOCZI [email protected] Belgium Prime Minister Ms. Sophie Wilmès sophia.wilmè[email protected] Twitter: CharlesMichel Minister of Foreign Affairs Mr. Didier Reynders [email protected] Twitter: dreynders UN Ambassdor in New York H.E. Mr. Philippe Kridelka [email protected] Twitter: @BelgiumUN UN Ambassdor in Geneva H.E. Mr. Geert Muylle [email protected] Denmark Prime Minister Mr. Mette Fredriksen [email protected] larsloekke Minister of Foreign Affairs Mr. Jeppe Kofod [email protected] Twitter: UM_dk UN Ambassdor in New York H.E. Mr. Martin Bille Hermann [email protected] Twitter: Denmark_UN UN Ambassdor in Geneva Mr. Morten Jespersen [email protected] Finland President Mr. Sauli Niinistö [email protected] Twitter: niinisto Prime Minister Mr. Sanna Marin [email protected] Twitter: juhasipila Minister of Foreign Affairs Mr. Peeka Haavisto [email protected] Twitter: Ulkoministeriö UN Ambassdor in New York H.E. Mr. -

Statement of the Steering Committee of the Eastern Partnership Civil
Sebastian Kurz, Federal Chancellor, Republic of Austria Sophie Wilmès, Prime Minister, Kingdom of Belgium Boyko Borissov, Prime Minister, Republic of Bulgaria Andrej Plenković, Prime Minister, Republic of Croatia Nicos Anastasiades, President of the Republic, Republic of Cyprus Andrej Babiš, Prime Minister, Czech Republic Mette Frederiksen, Prime Minister, Kingdom of Denmark Micheál Martin, Taoiseach, Republic of Ireland Jüri Ratas, Prime Minister, Republic of Estonia Sanna Marin, Prime Minister, Republic of Finland Emmanuel Macron, President of the Republic, French Republic Angela Merkel, Federal Chancellor, Federal Republic of Germany Kyriakos Mitsotakis, Prime Minister, Hellenic Republic Viktor Orbán, Prime Minister, Hungary Giuseppe Conte, Prime Minister, Italian Republic Krišjanis̄ Karinş̌ , Prime Minister, Republic of Latvia Gitanas Nauseda,̇ President, Republic of Lithuania Xavier Bettel, Prime Minister, Grand Duchy of Luxembourg Robert Abela, Prime Minister, Republic of Malta Mark Rutte, Prime Minister, Kingdom of the Netherlands Mateusz Morawiecki, Prime Minister, Republic of Poland António Costa, Prime Minister, Republic of Portugal Klaus Werner Iohannis, President, Romania Igor Matovič, Prime Minister, Slovak Republic Janez Janša, Prime Minister, Republic of Slovenia Pedro Sánchez, Prime Minister, Kingdom of Spain Stefan Löfven, Prime Minister, Kingdom of Sweden Ursula von der Leyen, President of the European Commission Charles Michel, President of the European Council David Sassoli, President of the European Parliament Josep -

Prime Minister Dr Robert Abela Office of the Prime Minister Auberge De Castille, Valetta VLT 1061 Malta
Prime Minister Dr Robert Abela Office of the Prime Minister Auberge de Castille, Valetta VLT 1061 Malta Minister Hon. Jose Herrera Ministry for the National Heritage, the Arts and Local Government Old Treasury Street, 30, Valetta VLT 1410 Malta Subject: Request for a comprehensive update on the latest state of affairs in the case of the murder of Daphne Caruana Galizia 25 March 2021 Dear Prime Minister, Dear Minister, On behalf of the Members of the Democracy, Rule of Law, and Fundamental Rights Monitoring Group (DRFMG) of the European Parliament, I am addressing you to express concerns and raise questions relating to the situation in Malta. The recent confession of Mr. Vincent Muscat shed further light on the criminal act of the murder of Daphne Caruana Galizia, while also showing that many questions around other individuals possibly implicated remain unanswered. The revelations make clear that the Maltese government must still consider the fight against organised crime, corruption and the intimidation of journalists as an utmost priority. I am particularly concerned over the possible involvement of public officials in the Daphne Caruana Galizia case. Allegations that former Economy Minister Chris Cardona could have been involved in a plot to kill a journalist and that MP and former parliamentary secretary Rosianne Cutajar could have accepted cash from Yorgen Fenech, the man accused of masterminding the assassination, are alarming. In light of this, bearing in mind DRFMG does not want to interfere with ongoing court proceedings, we would request the Maltese government to give our DRFMG a comprehensive update on the latest state of affairs in the case of the murder of Daphne Caruana Galizia.