Revitalization and Social Change: Contributions from Psychiatric Epidemiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Divaricating Plants in New Zealand in Relation to Moa Browsing
GREENWOOD AND ATKINSON: DIYARICATING PLANTS AND MOA BROWSING 21 EVOLUTION OF DIVARICATING PLANTS IN NEW ZEALAND IN RELATION TO MOA BROWSING R. M. GREENWOOD' and I. A. E. ATKINSON' SUMMAR Y: New Zealand appears to be the only country where spineless, small-leaved divaricating plants make up nearly 10% of the woody flora. Climatic explanations have been advanced to &ccount for the origin of these divaricating plants. We suggest that the divergent and interl~ced branching, the woody exterior and the tough stems of these plants are adaptations evolved in response to browsing by moas. Together with a few species of much smaHer birds, moas were the only browsing vertebrates in New Zealand prior to the arrival of man. Thq divaricate habit is probably only one of several strategies evolved by plants in response to moa browsing. However, because fioas fed in a different way from mammals there is little to support the idea that introduced browsing mammals have merely replaced moas as aQ ecological factor in New Zealand. MORPHOLOGICAL FEATURES OF NEW ZEALAND difficult. The most helpful keys are those of Bulmer DIY ARICATING fLANTS (1958) and Taylor (1961), which deal specifioolly The term Hdivaricating", indicating branching at with these plants. New Zealand species found in this a wide angle, is used in New Zealand to describe the investigation to be capable of divaricating are listed many species of small-leaved woody shrubs that in Table 1. In cases where there was difficulty in have closely interlaced bra,nches. Some are the deciding whether a species should be included in juvenile stages of trees that lose the divaricate habit the table the criteria used for inclusion were (i) as they grow taUer. -

Ecological and Genetic Analysis of Plant-Animal Interactions in Mediterranean Environments
UNIVERSIDAD DE MURCIA ESCUELA INTERNACIONAL DE DOCTORADO Ecological and Genetic Analysis of Plant-Animal Interactions in Mediterranean Environments Análisis Ecológico y Genético de Interacciones Planta-Animal en Ambientes Mediterráneos D. Vicente Martínez López 2018 Ecological and genetic analysis of plant-animal interactions in Mediterranean environments Análisis ecológico y genético de interacciones planta-animal en ambientes mediterráneos Tesis Doctoral Vicente Martínez López 2018 Escuela Internacional de Doctorado de la Universidad de Murcia (EIDUM) Universidad de Murcia Directores: Dra. Mª Pilar De la Rúa Tarín Dr. Francisco Robledano Aymerich Con el apoyo de (support): Esta tesis ha sido realizada en los Departamentos de Zoología y Antropología Física y Ecología e Hidrología de la Universidad de Murcia bajo de dirección de los doctores Mª Pilar De la Rúa Tarín y Francisco Robledano Aymerich. El autor ha sido beneficiario de un Contrato Predoctoral para la Formación del Profesorado Universitario (FPU) del Ministerio de Educación, Cultura y Deporte (referencia FPU 13/05115). Además ha realizado dos estancias predoctorales de tres meses de duración cada una financiada también por el Ministerio de Educación, Cultura y Deporte en régimen de concurrencia competitiva en la Universidad de Marburg (Alemania), supervisado por la Dra. Nina Farwig, y en CIBIO/InBIO (Universidad de Oporto, Portugal), supervisado por la Dra. Cristina García. Las investigaciones realizadas en el presente trabajo han recibido financiación de los proyectos de la -

Morristown Street Tree Resource Booklet
Morristown Street Tree Resource Booklet June 2020 I. Large Shade Trees for Areas Larger than 4’ x 6’ 3 Black Tupelo (Nyssa sylcatica) 4 Dawn Redwood (Metasequoia glyptostroboides) 5 Elm (Ulmus spp.) 6 Gingko (Gingko biloba) 7 Hardy Rubber Tree (Eucommia ulmoides) 8 Honey Locust (Gleditsia triacanthos inermis) 9 Katsura Tree (Cercidphyllum japonicum) 10 Kentucky Coffee Tree (Gymnocladus dioicus) 11 Linden (Tilia spp) 12 Little Leaf Linden (Tilia cordata) 13 Silver Linden (Tilia tomentosa) 14 Crimean Linden (Tilia x euchlora) 15 London Plane Tree (Platanus x acerfolia) 16 Maple, Red (Acer rubrum) 17 Maple, Sugar ( Acer saccharum) 18 Oak, Pin (Quercus palustris) 19 Oak, Red (Quercus rubra) 20 Oak, Shingle (Quercus imbricaria) 21 Oak, White (Quercus alba) 22 Oak, Willow (Quercus phellos) 23 Pagoda Tree (Styphnolobium japanicum) 24 Sweetgum (Liquidambur styraciflua) 25 Japanese Zelkova (Zelkova serrata) 26 II. Understory Small and Medium Trees for Areas Larger than 2’ x 6’ 27 American Yellowwood (Cladrastis kentukea) 28 Amur Maackia (Maackia amurensis) 29 Cherry (Prunus spp) 30 Crabapple (Malus spp) 31 Dogwood (Cornus spp) 32 Eastern Rudbud (Cercis canadensis) 33 Golden Raintree (Koelreuteria paniculata) 34 Hackberry (Celtis occidentalis) 35 Hawthorne (Crataegus spp) 36 Hop Hornbeam (Ostrya virginiana) 37 Japanese Snowball (Styrax japonicas) 38 Maple Amur (Acer ginnala ‘Flame’) 39 Maple, Hedge (Acer campestre) 40 Purpleleaf Plum (Prunus cerasifera) 41 Callery Pear (Pyrus calleryanan’) 42 I. Large Shade Trees for Areas Larger than 4’ x 6’ Black Tupelo (Nyssa sylcatica) Form: Pyramidal in youth with horizontal branches forming, and rounded or irregular crown. Mature Height: 30’ to 50’ Mature Spread: 20’ to 30’ Use: Acceptable street tree. -

Plant Structural Defences Against Browsing Birds: a Legacy of New Zealand’S Extinct Moas
OIKOS 104: 500Á/508, 2004 Plant structural defences against browsing birds: a legacy of New Zealand’s extinct moas William J. Bond, William G. Lee and Joseph M. Craine Bond, W. J., Lee, W. G. and Craine, J. M. 2004. Plant structural defences against browsing birds: a legacy of New Zealand’s extinct moas. Á/ Oikos 104: 500Á/508. Browsing by large vertebrates has been a major force in the evolution of terrestrial plants but Holocene extinctions of the browsers have left a legacy of broken biotic partnerships. Ratite birds were the largest herbivores in several regions, such as the moas of New Zealand. Many woody plants there have a distinct form of branching, described as ‘‘divaricate’’, with thin, wide angled, branches intertwining to form a tangled canopy. Divaricate branching has been interpreted as a form of protection against climate extremes or as an anachronistic defense against the extinct moas. Here we report the first experimental evidence that many of these plants are defended against extant ratite browsers. In feeding experiments on two tree species with different (heteroblastic) juvenile and adult branch morphology, emus and ostriches obtained adequate feeding rates from adult shoots but sub-maintenance feeding rates from juvenile shoots with the ratite-resistant traits. Divaricate juvenile shoots suffered 30Á/ 70% less biomass removal to the birds than adult shoots. Ratites browse by a distinctive clamping and tugging action. Structural defence traits that exploit the limitations of this feeding mode include narrow, strong, elastic branches that resist being torn off, wide branching angle (‘‘divaricate’’) that makes shoots difficult to swallow, and small, widely spaced leaves. -

HORIZONS Evolution of the Arctic Calanus Complex
JOURNAL OFJPR PLANKTON Advance RESEARCH Accessj VOLUME published0 j NUMBER January0 j PAGES 3, 12012–5 j 2012 HORIZONS Evolution of the Arctic Calanus complex: an Arctic marine avocado? Downloaded from JØRGEN BERGE 1,2*, TOVE M. GABRIELSEN 1, MARK MOLINE 1,3 AND PAUL E. RENAUD 1,4 1 2 UNIVERSITY CENTRE ON SVALBARD, PB 156, N-9171 LONGYEARBYEN, NORWAY, FACULTY OF BIOSCIENCES, FISHERIES AND ECONOMICS, UNIVERSITY OF 3 TROMSØ, N-9037 TROMSØ, NORWAY, CENTER FOR COASTAL MARINE SCIENCES, BIOLOGICAL SCIENCES DEPARTMENT, CALIFORNIA POLYTECHNIC STATE 4 UNIVERSITY, SAN LUIS OBISPO, CA 93407, USA AND AKVAPLAN-NIVA. FRAM CENTRE FOR CLIMATE AND THE ENVIRONMENT, N-9296 TROMSØ, NORWAY *CORRESPONDING AUTHOR: [email protected] http://plankt.oxfordjournals.org/ Received August 5, 2011; accepted in principle November 23, 2011; accepted for publication December 5, 2011 Corresponding editor: Mark J. Gibbons Before man hunted the large baleen whales to near extinction by the end of the nineteenth century, Arctic ecosystems were strongly influenced by these large pre- dators. Their main prey were zooplankton, among which the calanoid copepod at University Library of Tromsø on March 11, 2013 species of the genus Calanus, long considered key elements of polar marine ecosys- tems, are particularly abundant. These herbivorous zooplankters display a range of adaptations to the highly seasonal environments of the polar oceans, most notably extensive energy reserves and seasonal migrations to deep waters where the non-feeding season is spent in diapause. Classical work in marine ecology has suggested that slow growth, long lifespan and large body size in zooplankton are specific adaptations to life in cold waters with short and unpredictable feeding seasons. -

The Significance of Bernarr Macfadden's
1 UNFIT FOR AMERICA: THE SIGNIFICANCE OF BERNARR MACFADDEN’S “WEAK CHILD” CLAIM IN AMERICAN PHYSICAL CULTURE Hubbard M. Uhlhorn TC 660H Plan II Honors Program The University of Texas at Austin May 10, 2017 ________________________________________ Kimberly A. Beckwith, Ph.D. Department of Kinesiology and Health Education Supervising Professor _________________________________________ Tolga Ozyurcu Department of Kinesiology and Health Education Second Reader 2 Acknowledgements I would like to thank the entire staff of the H.J Lutcher Stark Center at the University of Texas Austin for allowing me the opportunity to preform archival research at such an expansive facility. I would like to thank Cindy Slater, the Associate Director for Library Services at the Stark Center for every pound of box she hauled out of the archives and her extensive knowledge of the collections which made my work so much easier. I would also like to thank Dr. Jan Todd, Co-Director of the Stark Center, for pointing me in the direction of writing a thesis dealing with this subject matter early last semester. A special thanks to my second reader, Dr. Tolga Ozyurtcu, for signing every single paper I gave to him, sometimes on blind faith. You provided some insight from your own personal experience writing these types of things and it helped me stay focused while writing it. A very special thanks to my Thesis Supervisor Dr. Kimberly Beckwith, who took substantial amounts of time out of her own busy schedule to discuss my paper and help me improve it. I’ve never seen someone edit as thoroughly as Kim does. -

Evolutionary Perspectives on Religion: an Overview and Synthesis
UNDERGRADUATE CONTRIBUTION EvoS Journal: The Journal of the Evolutionary Studies Consortium Evolutionary Perspectives on Religion: An Overview and Synthesis Zachary Smith* Holly Arrow Department of Psychology, University of Oregon ABSTRACT Religion is a cultural universal that has puzzled evolutionists since Darwin. The moral, social, emotional, and explanatory components that make up complex religious systems offer both evolutionary benefits and costs. Evolutionists who propose functional accounts of religion argue that it offers adaptive benefits that outweigh the costs. Theorists who propose nonfunctional accounts view religion as a byproduct of interactions among nonreligious cognitive adaptations and environments. Others argue that religion evolved via memetic transmission, which allows maladaptive features to persist. These maladaptive features may be anachronisms that were functional in the past but are detrimental to fitness in modern contexts. A thorough review reveals that work guided by these different perspectives is driven by divergent research questions that ultimately complement one another to offer a more comprehensive evolutionary account of the complexity, variety, and durability of religious belief and behavior. KEYWORDS Psychology of religion; evolution of religion; cultural evolution; cognitive adaptation; cognitive byproduct; meme theory; multi-level selection; exaptation INTRODUCTION In the 1740s a small Protestant group known as the Shakers formed in Manchester, England. The Shaker creed emphasized equality between men and women in religious practices, the need for communal living, a literalist view of the Bible, and a strict moral code. Following their eventual migration to New England, the Shakers attracted nearly 20,000 converts throughout the nineteenth century AUTHOR NOTE: Please direct correspondence to Zachary Smith, Small Groups Lab, Department of Psychology, 1227 University of Oregon, Eugene, OR 97403-1227. -

Avocado - Wikipedia, the Free Encyclopedia
Avocado - Wikipedia, the free encyclopedia Create account Log in Article Talk Read Edit View history Avocado From Wikipedia, the free encyclopedia Main page For the place in California, see Avocado, California. For the Pearl Jam album, see Pearl Jam Contents (album). Featured content The ( ) is a tree native to Current events avocado Persea americana [1] Avocado Random article Central Mexico, classified in the flowering plant family Donate to Wikipedia Lauraceae along with cinnamon, camphor and bay laurel. Wikimedia Shop Avocado or alligator pear also refers to the fruit (botanically a large berry that contains a single seed[2]) of Interaction the tree. Help Avocados are commercially valuable and are cultivated in About Wikipedia tropical and Mediterranean climates throughout the world. Community portal They have a green-skinned, fleshy body that may be pear- Recent changes shaped, egg-shaped, or spherical. Commercially, it ripens Contact Wikipedia after harvesting. Trees are partially self-pollinating and Toolbox often are propagated through grafting to maintain a predictable quality and quantity of the fruit. Print/export [hide] Languages Contents 1 History 1.1 Etymology Avocado fruit and foliage, Réunion island 2 Cultivation Az rbaycanca 2.1 Harvest and postharvest Bân-lâm-gú 2.2 Breeding Basa Banyumasan 2.3 Propagation and rootstocks Беларуская 2.4 Growing indoors Беларуская 2.5 Diseases (тарашкевіца) Ripe avocado fruit and cross-section 2.6 Cultivation in California Bislama 2.7 A cultivars Scientific classification Български 2.8 B cultivars Kingdom: Plantae Català 2.9 Other cultivars Cebuano Phylum: Angiosperms 3 Avocado-related international trade issues Česky Class: Magnoliids 4 Culinary uses Chamoru Order: Laurales 5 Nutritional value ChiTumbuka 6 As a houseplant Family: Lauraceae Dansk 7 Allergies Genus: Persea Deutsch 8 Toxicity to animals Diné bizaad Species: P. -

An Integrative Approach to Discern the Seed Dispersal Role of Frugivorous Guilds in a Mediterranean Semiarid Priority Habitat
An integrative approach to discern the seed dispersal role of frugivorous guilds in a Mediterranean semiarid priority habitat Diana Carolina Acosta-Rojas1,2, María Victoria Jiménez-Franco3,4, Víctor Manuel Zapata-Pérez5, Pilar De la Rúa1 and Vicente Martínez-López1,5 1 Department of Zoology and Physical Anthropology, Faculty of Veterinary, University of Murcia, Murcia, Spain 2 Senckenberg Biodiversity and Climate Research Centre (BiK-F), Frankfurt am Main, Germany 3 Ecology Area, Department of Applied Biology, Faculty of Experimental Sciences, University Miguel Hernández, Elche, Spain 4 Department of Ecological Modeling, UFZ–Helmholtz Centre for Environmental Research, Leipzig, Germany 5 Department of Ecology and Hydrology, Faculty of Biology, University of Murcia, Murcia, Spain ABSTRACT Seed dispersal is an essential process to maintain the viability of plant populations, and understanding this ecological process allows management strategies to be developed to conserve ecosystems. European Union priority habitat 5220Ã is defined as “Mediterranean arborescent shrubland with Ziziphus lotus” and it represents a favorable microclimate within the severe climatic conditions typical of the semiarid south-eastern region of the Iberian Peninsula. Therefore, the study of seed dispersal in this priority habitat by different frugivorous guilds, is a challenge for its conservation. In this study, we have characterized a mutualistic network of seed dispersal that is mediated by vertebrates (mammals and birds) in the protected habitat 5220Ã. The aims of this study were to: (i) identify the seed disperser community; (ii) analyze the relative role of key species in the dispersal process; and (iii) compare the functional ecology of the seed dispersal process between mammals Submitted 18 February 2019 and birds. -
OUT on a LIMB a Few Thoughts About Tree Health” Article by Tom SUMMER 2019, VOLUME 39, ISSUE 2 & Vickie Wiens on Page 6
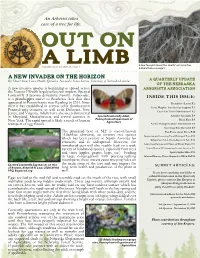
An Arborist takes care of a tree for life. OUT ON A LIMB A Few Thoughts About Tree Health” article by Tom SUMMER 2019, VOLUME 39, ISSUE 2 & Vickie Wiens on page 6. A NEW INVADER ON THE HORIZON A Quarterly Update By: Dave Olson, Forest Health Specialist, Nebraska Forest Service, University of Nebraska-Lincoln of the Nebraska A new invasive species is beginning to spread across Arborists Association the Eastern US with largely unknown impacts. Spotted Lanternfly (Lycorma delicatula) Family: Fulgoridae, is a planthopper native to Southeast Asia that first INSIDE THIS ISSUE: appeared in Pennsylvania near Reading in 2014. Since President’s Letter P.2 then it has established in several other Southeastern Terry Hughes Tree Service Support P.3 Pennsylvania counties, as well as in Delaware, New Jersey, and Virginia. Adults have also been discovered Can I Eat These Mushrooms? P.3 in Maryland, Massachusetts, and several counties in Spotted Lanternfly Adult, Arborist Spotlight P.4 Pennsylvania Department of Black Knot P.5 New York. The rapid spread is likely a result of human Agriculture transport of egg masses. A Few Thoughts about Tree Health P.6 Common Tree Removal P.9 The preferred host of SLF is tree-of-heaven Fun Facts about Trees P.10 (Ailanthus altissima), an invasive tree species Inspecting and Assessing Flood-Damaged Trees P.12 which has been present in North America for centuries and is widespread. However, the What Can NAA Do in Western NE P.12 introduced pest will also readily feed on a wide Lawn Care Detrimental Effects on Woody Plants P.13 variety of hardwood species, especially fruit trees Newest Western NE Community Forestry Specialist P.13 and vines (apples, grapes, hops, etc.) Feeding Spruce Spider Mites P.13 in large congregations with piercing-sucking Infected Nursery Plants Shipped to NE & IA P.14 mouthparts, these insects cause weeping holes on the main stem of the tree and may impact the Spotted Lanternfly Egg masses on tree- SUBMIT ARTICLES: of-heaven, Kenneth R. -

50Awesomefacts.Pdf
THE PLACE FOR LIFE. In 2017, as part of its Centennial Legacy Program, the Rotary Club of Windsor (1918) donated $225,000 to help build the Rotary (1918) Centennial Hub, linking the Chrysler Canada Greenway with the Herb Gray Parkway trails, and trails in the Towns of LaSalle and Tecumseh. In so doing, the Rotary Club effectively helped fill in a gap in the greenway system, and with the creation of the trail, the Greenway system links every community in Windsor Essex. Not to be outdone, in 2018 the Rotary Club of Windsor (1918) committed an additional $20,000 over four years to create the Rotary Forest - a shared project of all Rotary Clubs and all Rotarians in Windsor Essex. These projects not only contribute to the Rotary Club of Windsor (1918)’s legacy in Windsor Essex; they also contribute to an incredible legacy for the region - projects that connect communities, restore landscapes and habitats, and ultimately help create a place where people want to live in, play in, and invest in. The Rotary Club of Windsor (1918), more than most, recognizes the important connections between healthy economies, healthy people, and healthy landscapes. As part of the Club’s ongoing commitment to raising awareness and celebrating all the Windsor-Essex region has to offer, the Club, President Jules Hawkins introduced the “50 Awesome Environmental Fact about Windsor Essex’ as a way of increasing awareness of our regional environment. This is a compilation of those 50 Awesome Environmental Facts - an encouragement for Rotarians to get out and explore, enjoy, and celebrate what makes this region the #Place for LIfe. -

Reproductive Immunosuppression and Diet F 21
Current Anthropology Volume 43, Number 1, February 2002 ᭧ 2002 by The Wenner-Gren Foundation for Anthropological Research. All rights reserved 0011-3204/2002/4301-0002$3.50 Around the world, people recognize that pregnancy is Reproductive associated with nausea, vomiting, and marked changes in dietary preferences, a pattern termed pregnancy sick- ness (Flaxman and Sherman 2000).2 Nausea and vomiting Immunosuppression generally serve to protect the individual from the harm- ful effects of ingested toxins and toxin-producing path- and Diet ogens; vomiting expels the offensive substance, while nausea, a highly aversive experience, anchors remarkable one-trial learning, motivating future avoidance of the substance (Bernstein 1999). The complex and coordi- An Evolutionary Perspective on nated nature of these features, the specificity of their eliciting conditions, and the obvious benefits that they Pregnancy Sickness and Meat provide all suggest that normal nausea and vomiting are Consumption1 part of an adaptation, a trait that has evolved through natural selection because of the advantages that it fur- nishes to its possessors. However, in contrast to the usual circumstances associated with nausea and vomiting, by Daniel M. T. Fessler many pregnant women experience these symptoms after ingesting foods which others around them eat without ill effect—indeed, it seems that pregnant women often become nauseated before ingestion has occurred and, Pregnancy sickness, a suite of “symptoms” that frequently co-oc- most notably, experience nausea and vomiting at far cur during pregnancy, may be an adaptation providing behavioral higher frequencies than do other members of their com- prophylaxis against infection. Maternal immunosuppression, nec- munities. The striking differences between the circum- essary for tolerance of the fetus, results in gestational vulnerabil- ity to pathogens.