Orbit, Eyelids, and Cranial Nerves III, IV, & VI
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Lacrimal Obstruction
Yung_edit_final_Layout 1 01/09/2009 15:19 Page 81 Lacrimal Obstruction Proximal Lacrimal Obstruction – A Review Carl Philpott1 and Matthew W Yung2 1. Rhinology and Anterior Skull Base Fellow, St Paul’s Sinus Centre, St Paul’s Hospital, Vancouver; 2. Department of Otolaryngology, Ipswich Hospital NHS Trust Abstract While less common than distal lacrimal obstruction, proximal obstruction causes many cases of epiphora. This article examines the aetiology of proximal lacrimal obstruction and considers current management strategies with reference to recent literature. The Lester Jones tube is the favoured method of dealing with most cases of severe proximal obstruction; other methods have been tried with less success. Keywords Proximal lacrimal obstruction, epiphora, canalicular blockage, Lester Jones tube Disclosure: The authors have no conflicts of interest to declare. Received: 31 March 2009 Accepted: 14 April 2009 DOI: 10.17925/EOR.2009.03.01.81 Correspondence: Matthew W Yung, The Ipswich Hospital, Heath Road, Ipswich, Suffolk, IP4 5PD, UK. E: [email protected] Obstruction of the lacrimal apparatus commonly causes sufferers to dominant fashion.3 Where absence of the punctum and papilla present with symptoms of epiphora, for which they are commonly (congenital punctal agenesis) occurs, it is likely that more distal parts referred to ophthalmology departments. In those units where of the lacrimal apparatus are obliterated. collaboration with otorhinolaryngology occurs, the distal site of obstruction is usually dealt with. -

Evaluation of the Eyebrow Position After External Müller's Muscle
Journal of Plastic, Reconstructive & Aesthetic Surgery (2019) 72, 662–668 Evaluation of the eyebrow position after external Müller’s muscle tucking: A new technique for ptosis repair a , ∗ b c Kenichi Kokubo , Nobutada Katori , Kengo Hayashi , d e f a Jun Sugawara , Seiko Kou , Akiko Fujii , Shoko Haga , f Jiro Maegawa a Department of Plastic Surgery, Fujisawa Shounandai Hospital. 2345 Takakura, Fujisawa-shi, Kanagawa 251-0802, Japan b Department of Ocular Plastic & Orbital Surgery, Seirei Hamamatsu General Hospital. 2-12-12 Sumiyoshi, Naka-ku, Hamamatsu-shi, Shizuoka 430-8558, Japan c Yokohama Sakuragicho Eye Clinic. 1-200 Hinodecho, Naka-ku Yokohama-shi, Kanagawa 231-0006, Japan d JUN CLINIC, 1402-5 Kitaishidocho, Nagano-shi, Nagano 380-0826, Japan e KO CLINIC for Antiaging. 4-54 Onoecho, Naka-ku Yokohama-shi, Kanagawa 231-0015, Japan f Department of Plastic and Reconstructive Surgery, Yokohama City University Hospital. 3-9 Fukuura, Kanazawa-ku, Yokohama-shi, Kanagawa 236-0004, Japan Received 27 August 2018; accepted 6 January 2019 KEYWORDS Summary Eyebrow descent commonly occurs after ptosis repair or blepharoplasty surgery. Müller’s muscle; The procedures used to correct acquired blepharoptosis are primarily classified into four Eyebrow position; groups. These procedures target the levator aponeurosis, Müller’s muscle, both the aponeu- Blepharoptosis; rosis and Müller’s muscle, or the frontalis muscle. In this study, we used a new technique called MRD; external Müller’s muscle tucking (EMMT) on 51 patients (94 eyelids), which targets the Müller’s Ptosis repair muscle for involutional blepharoptosis. The patients were assessed by comparative analysis us- ing pre- and post-operative digital photographs. -

Treatment of Congenital Ptosis
13 Review Article Page 1 of 13 Treatment of congenital ptosis Vladimir Kratky1,2^ 1Department of Ophthalmology, Queen’s University, Kingston, Canada; 21st Medical Faculty, Charles University, Prague, Czech Republic Correspondence to: Vladimir Kratky, BSc, MD, FRCSC, DABO. Associate Professor of Ophthalmology, Director of Ophthalmic Plastic and Orbital Surgery, Oculoplastics Fellowship Director, Queen’s University, Kingston, Canada; 1st Medical Faculty, Charles University, Prague, Czech Republic. Email: [email protected]. Abstract: Congenital ptosis is an abnormally low position of the upper eyelid, with respect to the visual axis in the primary gaze. It can be present at birth or manifest itself during the first year of life and can be bilateral or unilateral. Additionally, it may be an isolated finding or part of a constellation of signs of a specific syndrome or systemic associations. Depending on how much it interferes with the visual axis, it may be considered as a functional or a cosmetic condition. In childhood, functional ptosis can lead to deprivation amblyopia and astigmatism and needs to be treated. However, even mild ptosis with normal vision can lead to psychosocial problems and correction is also advised, albeit on a less urgent basis. Although, patching and glasses can be prescribed to treat the amblyopia, the mainstay of management is surgical. There are several types of surgical procedure available depending on the severity and etiology of the droopy eyelid. The first part of this paper will review the different categories of congenital ptosis, including more common associated syndromes. The latter part will briefly cover the different surgical approaches, with emphasis on how to choose the correct condition. -

Conjunctival Flora of Normal Human Eye Which Vary with Age, Sex, Geographical Distribution, Right and Left Eye
Central JSM Ophthalmology Research Article *Corresponding author Purnima Rajkarnikar Sthapit, Department of Ophthalmology, Dhulikhel Hospital, Kathmandu Conjunctival Flora of Normal University Hospital, Dhulikhel, Kavre, Nepal, Tel: 009779813254962; Fax: 0097711490707; Email: Human Eye Submitted: 23 February 2014 Purnima Rajkarnikar Sthapit1* and Nhuchhe Ratna Tuladhar2 Accepted: 03 March 2014 1Department of Ophthalmology, Kathmandu University School of Medical Sciences, Nepal Published: 07 March 2014 2Department of Microbiology, Kathmandu University School of Medical Sciences, Nepal ISSN: 2333-6447 Copyright Abstract © 2014 Sthapit et al. Background: The normal flora of the eye plays an important role in maintaining OPEN ACCESS ocular homeostasis by various mechanisms. They comprise of mainly bacteria which do not cause infection in normal conditions but can be a main source of infection after Keywords ocular surgery, trauma or in immune compromised. The ranges of these microorganisms • Coagulase positive Staphylococcus vary with age, sex and geographical distribution. Therefore it is very important for the • Normal flora ophthalmologist to know the ocular normal flora before giving prophylactic antibiotics • Ocular infection and treating infections. • Ocular trauma Objectives: To describe the conjunctival flora of normal human eye which vary with age, sex, geographical distribution, right and left eye. Methodology: A total of 200 conjunctival swabs from 100 patients with healthy eyes were sent for microbiological evaluation to describe the various microorganisms isolated as normal flora of conjunctiva. Result: The growth of bacteria was seen in 78.5% of patients, the commonest flora isolated was Coagulase negative Staphylocccus in 51%. Greater number of male patients had sterile conjunctiva than females and conjunctiva of old people were found to be increasingly more colonised than young. -
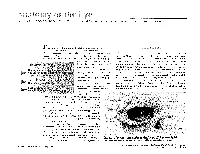
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

Volume 1: the Upper Extremity
Volume 1: The Upper Extremity 1.1 The Shoulder 01.00 - 38.20 (37.20) 1.1.1 Introduction to shoulder section 0.01.00 0.01.28 0.28 1.1.2 Bones, joints, and ligaments 1 Clavicle, scapula 0.01.29 0.05.40 4.11 1.1.3 Bones, joints, and ligaments 2 Movements of scapula 0.05.41 0.06.37 0.56 1.1.4 Bones, joints, and ligaments 3 Proximal humerus 0.06.38 0.08.19 1.41 Shoulder joint (glenohumeral joint) Movements of shoulder joint 1.1.5 Review of bones, joints, and ligaments 0.08.20 0.09.41 1.21 1.1.6 Introduction to muscles 0.09.42 0.10.03 0.21 1.1.7 Muscles 1 Long tendons of biceps, triceps 0.10.04 0.13.52 3.48 Rotator cuff muscles Subscapularis Supraspinatus Infraspinatus Teres minor Teres major Coracobrachialis 1.1.8 Muscles 2 Serratus anterior 0.13.53 0.17.49 3.56 Levator scapulae Rhomboid minor and major Trapezius Pectoralis minor Subclavius, omohyoid 1.1.9 Muscles 3 Pectoralis major 0.17.50 0.20.35 2.45 Latissimus dorsi Deltoid 1.1.10 Review of muscles 0.20.36 0.21.51 1.15 1.1.11 Vessels and nerves: key structures First rib 0.22.09 0.24.38 2.29 Cervical vertebrae Scalene muscles 1.1.12 Blood vessels 1 Veins of the shoulder region 0.24.39 0.27.47 3.08 1.1.13 Blood vessels 2 Arteries of the shoulder region 0.27.48 0.30.22 2.34 1.1.14 Nerves The brachial plexus and its branches 0.30.23 0.35.55 5.32 1.1.15 Review of vessels and nerves 0.35.56 0.38.20 2.24 1.2. -

Endoscopic Supraorbital Eyebrow Approach for the Surgical Treatment of Extraaxial and Intraaxial Tumors
See the corresponding editorial in this issue (E21). Neurosurg Focus 37 (4):E20, 2014 ©AANS, 2014 Endoscopic supraorbital eyebrow approach for the surgical treatment of extraaxial and intraaxial tumors ROBERTO GAZZERI, M.D.,1,2 YUYA NISHIYAMA, M.D., PH.D.,1,3 And CHARLES TEO, M.D.1 1Centre for Minimally Invasive Neurosurgery, Prince of Wales Private Hospital, Sydney, Australia; 2Department of Neurosurgery, San Giovanni Addolorata Hospital, Rome, Italy; and 3Department of Neurosurgery, Fujita Health University School of Medicine, Toyoake, Japan Object. The supraorbital eyebrow approach is a minimally invasive technique that offers wide access to the anterior skull base region and parasellar area through a subfrontal corridor. The use of neuroendoscopy allows one to extend the approach further to the pituitary fossa, the anterior third ventricle, the interpeduncular cistern, the an- terior and medial temporal lobe, and the middle fossa. The supraorbital approach involves a limited skin incision, with minimal soft-tissue dissection and a small craniotomy, thus carrying relatively low approach-related morbidity. Methods. All consecutive patients who underwent the endoscopic supraorbital eyebrow approach were retro- spectively analyzed for lesion location, pathology, length of stay, complications, and cosmetic results. Results. During a 56-month period, 97 patients (mean age 58.5 years) underwent an endoscopic eyebrow ap- proach to resect extra- and intraaxial brain lesions. The most common pathologies treated were meningiomas (n = 41); craniopharyngiomas (n = 22); dermoid tumors (n = 7); metastases (n = 4); gliomas (n = 3); and other miscel- laneous frontal, parasellar, and midbrain (n = 23) lesions. The median length of postoperative hospital stay was 2.7 days (range 1–8 days). -

Orbital Imaging in Thyroid-Related Orbitopathy
Orbital imaging in thyroid-related orbitopathy Christopher Lo, MD, Shoaib Ugradar, MD, and Daniel Rootman, MD, MS SUMMARY A broad understanding of the different imaging modalities used to assess the physiologic changes seen in Graves’ orbitopathy complement clinical examination. Subtle applications of radiographic imaging techniques allow for a better understanding of the overall physiology of the orbit, quantify progression of disease, and differentiate it from orbital diseases with overlapping features. A nuanced approach to interpreting imaging features may allow us to delineate inactive from active thyroid eye disease, and advances within this field may arm clinicians with the ability to better predict and prevent dysthyroid optic neuropathy. ( J AAPOS 2018;22:256.e1-256.e9) rbital imaging plays a central role in the diag- mean inferior rectus width, 4.8 mm; medial rectus width, nosis and management of thyroid-related orbit- 4.2 mm; superior rectus width, 4.6 mm; and lateral rectus O opathy (TRO). Diagnostically, it is used to width, 3.3 mm.8,9 These numbers can be used as a guide; compliment a careful ophthalmic examination, laboratory however, they represent population averages, each with values, and ancillary studies to confirm the presence of significant variation. Overlap in populations exist, and TRO and/or dysthyroid optic neuropathy (DON). It can both diseased and nondiseased muscles can have widths also be helpful in surgical planning and understanding close to these values. In the end, there are no strict rules. the progression of thyroid myopathy. Computed tomogra- In terms of muscle involvement, clinical myopathy is phy (CT), magnetic resonance imaging (MRI), ultrasound, thought to most often involve the inferior rectus muscle, and nuclear medicine all have applications in the field. -

New Theory on Facial Beauty: Ideal Dimensions in the Face and Its Application to Your Practice by Dr
New Theory on Facial Beauty: Ideal Dimensions in the Face And its application to your practice By Dr. Philip Young Aesthetic Facial Plastic Surgery 2015 Bellevue, Washington American Brazilian Aesthetic Meeting • Hello my presentation is on studying some further elements of a new theory on facial beauty called the Circles of Prominence. • Specifically we are going to be studying some key dimensions in the face that I think could possibly help your practice. • I’m from Bellevue Washington Home of Bill Gates, Microsoft and Starbucks. Beauty In my opinion Beauty is the most important trait that we have and it is the one trait that can have the most dramatic impact in our lives. Obviously finding the answer for Beauty is essential in our industry. The answers have alluded us: the magic number of Phi, cephalometrics, the neo classical canons by Leonardo Da Vinci, the averageness theory, etc. have all come short in finding what makes a face beautiful. • The Circles of Prominence is a theory that I discovered in 2003-2005 and was published in the Archives of Facial Plastic Surgery in 2006 and Received the Sir Harold Delf Gillies Award from the American Academy of Facial Plastic Surgery. The Circles of Prominence • Original published Archives FPS 2006 • Based on the idea that there is an ideal • Everything on the face has an ideal as well • Because we spend so much time looking at the iris • All dimensions of the face are related to the width of the iris • Obviously with a better definition of beauty our results in plastic surgery can be improved • The circles of prominence is based on the belief that there is an ideal.