Folliculitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
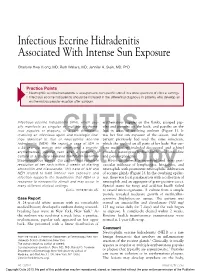
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Abscess Prevention
ABSCESS PREVENTION ▪ Chest pains may occur if infection How do you soak/use Avoiding abscesses goes to heart or lungs compresses? • Wash your hands and the injection site. What should I do if I get ▪ Use warm/hot water (that doesn’t burn your skin) • Use alcohol pads and wipe an abscess? ▪ Soak in tub of plain hot water or hot back & forth (rub hard) over ▪ Treat at home with warm soaks water with Epsom salts injection site to remove dirt. only if: ▪ Use hot, wet, clean washcloth and - No red streaks hold on abscess, if abscess cannot • Then use another new alcohol - Skin not hot and puffy be soaked in tub pad for the final cleaning. ▪ Soak abscess 3 to 4 times a day for ▪ Go to a clinic if abscess: 10-15 minutes each time, if possible What is a skin abscess? - Not improving, especially ▪ Cover with a clean dry bandage after after 5-7 days soaking ▪ Pocket of pus - Gets bigger and/or very ▪ soaking/using compresses ▪ Often found at injection sites, but STOP painful when abscess starts draining can be found elsewhere - Is hot and puffy ▪ More likely with Red streaks start spreading skin-popping from the abscess-go ASAP! muscling What about missing a vein ▪ Go to emergency room if: ▪ May occur even after you stop Chest pain antibiotics? injecting High fever, chills ▪ Take all antibiotics, if Infection looks like it is How do you know it’s an spreading fast prescribed, even if you feel better abscess? ▪ Take antibiotics after you fix (if ▪ using heroin) ▪ Pink or reddish lump on skin ▪ Do not take antibiotics with ▪ Tender or painful Warning -

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA). -

Abscesses Are a Serious Problem for People Who Shoot Drugs
Where to Get Your Abscess Seen Abscesses are a serious problem for people who shoot drugs. But what the hell are they and where can you go for care? What are abscesses? Abscesses are pockets of bacteria and pus underneath you skin and occasionally in your muscle. Your body creates a wall around the bacteria in order to keep the bacteria from infecting your whole body. Another name for an abscess is a “soft tissues infection”. What are bacteria? Bacteria are microscopic organisms. Bacteria are everywhere in our environment and a few kinds cause infections and disease. The main bacteria that cause abscesses are: staphylococcus (staff-lo-coc-us) aureus (or-e-us). How can you tell when you have an abscess? Because they are pockets of infection abscesses cause swollen lumps under the skin which are often red (or in darker skinned people darker than the surrounding skin) warm to the touch and painful (often VERY painful). What is the worst thing that can happen? The worst thing that can happen with abscesses is that they can burst under your skin and cause a general infection of your whole body or blood. An all over bacterial infection can kill you. Another super bad thing that can happen is a endocarditis, which is an infection of the lining of your heart, and “septic embolism”, which means that a lump of the contaminates in your abscess get loose in your body and lodge in your lungs or brain. Why do abscesses happen? Abscesses are caused when bad bacteria come in to contact with healthy flesh. -

Intra-Abdominal Ventriculoperitoneal Shunt Abscess from Streptococcus Pyogenes After Pharyngitis with Scarlet Fever
NEURO ISSN 2377-1607 http://dx.doi.org/10.17140/NOJ-1-107 Open Journal Case Report Intra-Abdominal Ventriculoperitoneal Shunt *Corresponding author Abscess from Streptococcus Pyogenes Edward A. Monaco 3rd, MD, PhD Assistant Professor after Pharyngitis with Scarlet Fever: Case Department of Neurological Surgery University of Pittsburgh Medical Center, Suite F158, 200 Lothrop Report and Review of the Literature Street, Pittsburgh, PA 15213, USA Tel. 412-647-6777 Stephanie H. Chen and Edward A. Monaco 3rd* Fax: 412-647-6483 E-mail: [email protected] Department of Neurological Surgery, University of Pittsburgh Medical Center, Suite F158, 200 Lothrop Street, Pittsburgh, PA 15213, USA Volume 1 : Issue 1 Article Ref. #: 1000NOJ1107 ABSTRACT Article History Received: November 13th, 2014 Objective: Infection is one of the most frequent complications of ventriculoperitoneal shunts. th Accepted: December 15 , 2014 However, Streptococcus pyogenes (Group A Streptococcus, GAS) as a causative agent appears th Published: December 16 , 2014 to be extremely rare. We present an unusual case of a peritoneal shunt infection due to GAS that occurred after pharyngitis with scarlet fever. Case Description: A 31 year-old woman with congenital shunt-dependent hydrocephalus pre- Citation sented with fever, vomiting, and acute abdominal symptoms several weeks after being treated Chen SH, Monaco EA 3rd. Intra-ab- dominal ventriculoperitoneal shunt for pharyngitis and scarlet fever. She was found to have a large intra-abdominal peritoneal abscess from Streptococcus pyo- catheter-associated abscess that grew out GAS. genes after pharyngitis with scarlet Results: The patient’s shunt was externalized at the clavicle and the cerebrospinal fluid (CSF) fever: Case report and review of the was sterile. -

Strep Throat and Scarlet Fever N
n Strep Throat and Scarlet Fever n After a few days, the rash begins to fade. The skin usually Strep throat is caused by infection with the bac- begins to peel, as it often does after a sunburn. teria Streptococcus. In addition to sore throat, swollen glands, and other symptoms, some chil- What are some possible dren develop a rash. When this rash is present, the infection is called scarlet fever. If your child complications of scarlet fever? has a strep infection, he or she will need antibio- Strep infection has some potentially serious complica- tics to treat it and to prevent rheumatic fever, tions. With proper treatment, most of these can be pre- which can be serious. vented. Complications include: Strep infection may cause an abscess (localized area of pus) in the throat. What are strep throat and scarlet Rheumatic fever. This disease develops a few weeks after fever? the original strep infection. It is felt to be caused by our immune system. It can be serious and can cause fever, heart Most sore throats are caused by virus, but strep throat is inflammation, arthritis, and other symptoms. Your child caused by the bacteria Group A Strepococcus. Treatment can be left with heart problems called rheumatic disease. of this infection with antibiotics may help your child feel Rheumatic fever is uncommon now and can be prevented better and prevent rheumatic fever. by treating the strep infection properly with antibiotics. Some children with strep throat or strep infections else- where may develop a rash. When that occurs, the infection Acute glomerulonephritis. -

Pseudomonas Skin Infection Clinical Features, Epidemiology, and Management
Am J Clin Dermatol 2011; 12 (3): 157-169 THERAPY IN PRACTICE 1175-0561/11/0003-0157/$49.95/0 ª 2011 Adis Data Information BV. All rights reserved. Pseudomonas Skin Infection Clinical Features, Epidemiology, and Management Douglas C. Wu,1 Wilson W. Chan,2 Andrei I. Metelitsa,1 Loretta Fiorillo1 and Andrew N. Lin1 1 Division of Dermatology, University of Alberta, Edmonton, Alberta, Canada 2 Department of Laboratory Medicine, Medical Microbiology, University of Alberta, Edmonton, Alberta, Canada Contents Abstract........................................................................................................... 158 1. Introduction . 158 1.1 Microbiology . 158 1.2 Pathogenesis . 158 1.3 Epidemiology: The Rise of Pseudomonas aeruginosa ............................................................. 158 2. Cutaneous Manifestations of P. aeruginosa Infection. 159 2.1 Primary P. aeruginosa Infections of the Skin . 159 2.1.1 Green Nail Syndrome. 159 2.1.2 Interdigital Infections . 159 2.1.3 Folliculitis . 159 2.1.4 Infections of the Ear . 160 2.2 P. aeruginosa Bacteremia . 160 2.2.1 Subcutaneous Nodules as a Sign of P. aeruginosa Bacteremia . 161 2.2.2 Ecthyma Gangrenosum . 161 2.2.3 Severe Skin and Soft Tissue Infection (SSTI): Gangrenous Cellulitis and Necrotizing Fasciitis. 161 2.2.4 Burn Wounds . 162 2.2.5 AIDS................................................................................................. 162 2.3 Other Cutaneous Manifestations . 162 3. Antimicrobial Therapy: General Principles . 163 3.1 The Development of Antibacterial Resistance . 163 3.2 Anti-Pseudomonal Agents . 163 3.3 Monotherapy versus Combination Therapy . 164 4. Antimicrobial Therapy: Specific Syndromes . 164 4.1 Primary P. aeruginosa Infections of the Skin . 164 4.1.1 Green Nail Syndrome. 164 4.1.2 Interdigital Infections . 165 4.1.3 Folliculitis . -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Skin Disease and Disorders
Sports Dermatology Robert Kiningham, MD, FACSM Department of Family Medicine University of Michigan Health System Disclosures/Conflicts of Interest ◼ None Goals and Objectives ◼ Review skin infections common in athletes ◼ Establish a logical treatment approach to skin infections ◼ Discuss ways to decrease the risk of athlete’s acquiring and spreading skin infections ◼ Discuss disqualification and return-to-play criteria for athletes with skin infections ◼ Recognize and treat non-infectious skin conditions in athletes Skin Infections in Athletes ◼ Bacterial ◼ Herpetic ◼ Fungal Skin Infections in Athletes ◼ Very common – most common cause of practice-loss time in wrestlers ◼ Athletes are susceptible because: – Prone to skin breakdown (abrasions, cuts) – Warm, moist environment – Close contacts Cases 1 -3 ◼ 21 year old male football player with 4 day h/o left axillary pain and tenderness. Two days ago he noticed a tender “bump” that is getting bigger and more tender. ◼ 16 year old football player with 3 day h/o mildly tender lesions on chin. Started as a single lesion, but now has “spread”. Over the past day the lesions have developed a dark yellowish crust. ◼ 19 year old wrestler with a 3 day h/o lesions on right side of face. Noticed “tingling” 4 days ago, small fluid filled lesions then appeared that have now started to crust over. Skin Infections Bacterial Skin Infections ◼ Cellulitis ◼ Erysipelas ◼ Impetigo ◼ Furunculosis ◼ Folliculitis ◼ Paronychea Cellulitis Cellulitis ◼ Diffuse infection of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin – Triad of erythema, edema, and warmth in the absence of underlying foci ◼ S. aureus or S. pyogenes Erysipelas Erysipelas ◼ Superficial infection of the dermis ◼ Distinguished from cellulitis by the intracutaneous edema that produces palpable margins of the skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F.