(RS) Is Characterized by Inflammation of Nasal and Paranasal Sinuses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nasal Polyposis, Eosinophil Dominated Inflammation, and Allergy
Thorax 2000;55 (Suppl 2):S79–S83 S79 Nasal polyposis, eosinophil dominated Thorax: first published as 10.1136/thorax.55.suppl_2.S79 on 1 October 2000. Downloaded from inflammation, and allergy Niels Mygind, Ronald Dahl, Claus Bachert A polyp is an oedematous mucous membrane computed tomographic (CT) scanning). The which forms a pedunculating process with a overall prevalence rate is probably about slim or broad stalk or base. Nasal polyps origi- 2–4%5–7 which increases with age of the study nate in the upper part of the nose around the population. Nasal polyposis occurs with a high openings to the ethmoidal sinuses. The polyps frequency in groups of patients with specified extend into the nasal cavity from the middle airway diseases (table 1). meatus, resulting in nasal blockage and re- Although symptomatic nasal polyposis is stricted airflow to the olfactory region. The rare in the general population, much higher polyp stroma is highly oedematous with a vary- figures for the occurrence of isolated nasal ing density of inflammatory cells. Nasal polyps have been obtained from necropsy polyposis, consisting of recurrent, multiple studies. A thorough endoscopic examination of polyps, is part of an inflammatory reaction removed nasoethmoidal blocks and endoscopic involving the mucous membrane of the nose, examination of unselected necropsy specimens paranasal sinuses, and often the lower airways. have shown polyps in as many as 25–40% of The polyps are easily accessible for immuno- specimens.89 logical and histological studies and an increas- Allergic rhinitis has a high prevalence rate of ing number of publications have appeared in about 15–20%.10 Most cases in the western recent years, including two monographs.12 world are caused by pollen allergy, having a Nasal polyps have long been associated with seasonal occurrence. -

(CD-P-PH/PHO) Report Classification/Justifica
COMMITTEE OF EXPERTS ON THE CLASSIFICATION OF MEDICINES AS REGARDS THEIR SUPPLY (CD-P-PH/PHO) Report classification/justification of medicines belonging to the ATC group R01 (Nasal preparations) Table of Contents Page INTRODUCTION 5 DISCLAIMER 7 GLOSSARY OF TERMS USED IN THIS DOCUMENT 8 ACTIVE SUBSTANCES Cyclopentamine (ATC: R01AA02) 10 Ephedrine (ATC: R01AA03) 11 Phenylephrine (ATC: R01AA04) 14 Oxymetazoline (ATC: R01AA05) 16 Tetryzoline (ATC: R01AA06) 19 Xylometazoline (ATC: R01AA07) 20 Naphazoline (ATC: R01AA08) 23 Tramazoline (ATC: R01AA09) 26 Metizoline (ATC: R01AA10) 29 Tuaminoheptane (ATC: R01AA11) 30 Fenoxazoline (ATC: R01AA12) 31 Tymazoline (ATC: R01AA13) 32 Epinephrine (ATC: R01AA14) 33 Indanazoline (ATC: R01AA15) 34 Phenylephrine (ATC: R01AB01) 35 Naphazoline (ATC: R01AB02) 37 Tetryzoline (ATC: R01AB03) 39 Ephedrine (ATC: R01AB05) 40 Xylometazoline (ATC: R01AB06) 41 Oxymetazoline (ATC: R01AB07) 45 Tuaminoheptane (ATC: R01AB08) 46 Cromoglicic Acid (ATC: R01AC01) 49 2 Levocabastine (ATC: R01AC02) 51 Azelastine (ATC: R01AC03) 53 Antazoline (ATC: R01AC04) 56 Spaglumic Acid (ATC: R01AC05) 57 Thonzylamine (ATC: R01AC06) 58 Nedocromil (ATC: R01AC07) 59 Olopatadine (ATC: R01AC08) 60 Cromoglicic Acid, Combinations (ATC: R01AC51) 61 Beclometasone (ATC: R01AD01) 62 Prednisolone (ATC: R01AD02) 66 Dexamethasone (ATC: R01AD03) 67 Flunisolide (ATC: R01AD04) 68 Budesonide (ATC: R01AD05) 69 Betamethasone (ATC: R01AD06) 72 Tixocortol (ATC: R01AD07) 73 Fluticasone (ATC: R01AD08) 74 Mometasone (ATC: R01AD09) 78 Triamcinolone (ATC: R01AD11) 82 -

Epinephrine Versus Tramazoline to Reduce Nasal Bleeding During Nasotracheal Intubation. a Double- Blind Randomized Trial
Epinephrine versus tramazoline to reduce nasal bleeding during nasotracheal intubation. A double- blind randomized trial Aiji Sato(Boku) ( [email protected] ) Aichi Gakuin University Yoshiki Sento Nagoya City University Yuji Kamimura Nagoya City University Eisuke Kako Nagoya City University Masahiro Okuda Aichi Gakuin University Naoko Tachi Aichi Gakuin University Yoko Okumura Aichi Gakuin University Mayumi Hashimoto Aichi Gakuin University Hiroshi Hoshijima Tohoku University Fumihito Suzuki Akita National Hospital Kazuya Sobue Nagoya City University Research Article Keywords: Nasotracheal intubation, Epinephrine, Tramazoline, Nasal bleeding Posted Date: February 10th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-148779/v1 Page 1/14 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 2/14 Abstract BACKGROUND Nasal bleeding is the most common complication during nasotracheal intubation (NTI). To reduce nasal bleeding, the nasal cavity is treated with vasoconstrictors (epinephrine [E] or tramazoline [T]) prior to NTI. This study aimed to determine whether E or T is more effective and safe for reducing nasal bleeding during NTI. METHODS This study was preregistered on UMIN-CTR after being approved by the IRB of the School of Dentistry at Aichi Gakuin University. Written consent was received from all the patients. Total 206 patients aged 20–70 years and classied as 1–2 on American Society of Anesthesiologists-physical status were scheduled to undergo general anesthesia with NTI. Patients with a narrowed nasal cavity observed during preoperative CT test (n = 3), patients with hypertension (n = 3), patients undergoing antithrombotic therapy, and patients who did not give consent (n = 3) were excluded from the study. -

List of Union Reference Dates A
Active substance name (INN) EU DLP BfArM / BAH DLP yearly PSUR 6-month-PSUR yearly PSUR bis DLP (List of Union PSUR Submission Reference Dates and Frequency (List of Union Frequency of Reference Dates and submission of Periodic Frequency of submission of Safety Update Reports, Periodic Safety Update 30 Nov. 2012) Reports, 30 Nov. -

Nasal Polyposis: a Review
Global Journal of Otolaryngology ISSN 2474-7556 Review Article Glob J Otolaryngol - Volume 8 Issue 2 May 2017 Copyright © All rights are reserved by Sushna Maharjan DOI: 10.19080/GJO.2017.0 Nasal Polyposis: A Review Sushna Maharjan1*, Puja Neopane2, Mamata Tiwari1 and Ramesh Parajuli3 1Department of Pathology, Chitwan Medical College Teaching Hospital, Nepal 2Department of Oral Medicine and Pathology, Health Sciences University of Hokkaido, Japan 3Department of Department of Otorhinolaryngology, Chitwan Medical College Teaching Hospital, Nepal Submission: May 07, 2017; Published: May 30, 2017 *Corresponding author: Sushna Maharjan, Department of Pathology, Chitwan Medical College Teaching Hospital (CMC-TH), P.O. Box 42, Bharatpur, Chitwan, Nepal, Email: Abstract Nasal polyp is a benign lesion that arises from the mucosa of the nasal sinuses or from the mucosa of the nasal cavity as a macroscopic usuallyedematous present mass. with The nasalexact obstruction,etiology is still rhinorrhea unknown and and postnasalcontroversial, drip. but Magnetic it is assumed resonance that imagingmain causes is suggested, are inflammatory particularly conditions to rule andout allergy. It is more common in allergic patients with asthma. Interleukin-5 has found to be significantly raised in nasal polyps. The patients seriousKeywords: conditions Allergy; such Interleukin-5; as neoplasia. Nasal Histopathological polyp; Neoplasia examination is also suggested to rule out malignancy and for definite diagnosis. Abbreviations: M:F- Male: Female; IgE: Immunoglobulin E; IL: Interleukin; CRS: Chronic Rhinosinusitis; HLA: Human Leucocyte Antigen; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging Introduction the nose and nasal sinuses characterized by stromal edema and Nasal polyps are characterized by benign lesions that arise from the mucosa of the nasal sinuses, most often from the cause may be different. -

Surgical Management of Nasal Airway Obstruction
Surgical Management of Nasal Airway Obstruction John F. Teichgraeber, MDa, Ronald P. Gruber, MDb, Neil Tanna, MD, MBAc,* KEYWORDS Nasal obstruction Nasal breathing Septal deviation Nasal valve narrowing Turbinate hypertrophy KEY POINTS The management and diagnosis of nasal airway obstruction requires an understanding of the form and function of the nose. Nasal airway obstruction can be structural, physiologic, or a combination of both. Anatomic causes of airway obstruction include septal deviation, internal nasal valve narrowing, external nasal valve collapse, and inferior turbinate hypertrophy. Thus, the management of nasal air obstruction must be selective and carefully considered. The goal of surgery is to address the deformity and not just enlarge the nasal cavity. INTRODUCTION vomer, and maxillary crest. The narrowest portion of the nose is the internal nasal valve (10–15), The management and diagnosis of nasal airway which is formed by the septum, the inferior turbi- obstruction requires an understanding of the nate, and the upper lateral cartilage. Short nasal form and function of the nose. Nasal airway bones, a narrow midnasal fold, and malposition obstruction can be structural, physiologic, or a of the alar cartilages all predispose patients to in- combination of both. Thus, the management of ternal valve incompetence. nasal airway obstruction must be selective and The lateral wall of the nose contains 3 to 4 turbi- often involves medical management. The goal of nates (inferior, middle, superior, supreme) and the surgery is to address the deformity and not just corresponding meatuses that drain the paranasal enlarge the nasal cavity. This article reviews airway sinuses. The nasolacrimal duct drains through obstruction and its treatment. -

New Medical Treatments for Nasal Polyps
New Medical Treatments for Nasal Polyps February 7, 2020 Brian Modena, MD, MSc 1 Disclosures Research support: NHLBI‐Supported Researcher Self Care Catalysts: architect of Health StorylinesTM app Personal Fees: AstraZeneca, GSK, Regeneron, Sanofi 42nd Annual Pulmonary and Allergy Update Objectives 1. Discuss the epidemiology, biology, pathophysiology, and symptoms of CRS with nasal polyposis (CRSwNP). 2. Review treatment guidelines and recommendations for CRSwNP. 3. Review the many scoring systems used to evaluate CRSwNP. 4. Discuss in detail the Phase II and Phase III clinical trials using biologics for treatment of CRSwNP. Nasal Polyposis Epidemiology Prevalence = ~4%1; (CRS = ~11‐12%)2 Costs: Genetic inheritance = ~14% 2 Increases with age; peak ~50 years CRS = ~$8 billion/year Caucasians = Th2‐driven inflammation. Per patient per year: $13,000; Male to female = 2:1 $26,000 if surgery performed. Asians = Th1‐driven inflammation. Association with allergic rhinitis is weak. Surgeries/year = ~500,000 Disease Prevalence estimates 1. Hastan, Fokkens, et al, 2011 Allergic rhinitis Adult: 0.1%; Children 1.5%1 2. Lange, Holst, et al., Clin Otolaryngol 2013. 3. Mygind. JACI. 1990 Dec;86(6 Pt 1):827‐9. Asthma 5‐22% 4. Schleimer RP. Annu Rev Pathol. 2017;12:331‐57. 5. Hunter TD, DeConde AS, Manes RP. J Med Econ. 2018;21(6):610‐5. CRS 20‐25%1‐4 6. Palmer JN, Messina JC, Biletch R, et al. Allergy Asthma Proc. 2018;39:1‐9. NSAID intolerance 36‐72% 7. Pearlman AN, Chandra RK, Chang D, et al. Am J Rhinol Allergy. 2009;23(2):145‐8. NSAID intolerance and asthma 80% 8. -

Surgical Management of Polyps in the Treatment of Nasal Airway
Surgical Management of Polyps in the TreatmentofNasal Airway Obstruction Samuel S. Becker, MD KEYWORDS FESS Nasal polyps Sinonasal polyps Polyp treatment Nasal obstruction In addition to their role in chronic rhinosinusitis and nasal congestion, sinonasal polyps are associated with significant nasal obstruction. Via a purely mechanical effect (ie, obstruction at its simplest level), polyps alter and otherwise block the normal flow of air through the nose. Similarly, by blocking the drainage pathways of the paranasal sinuses, sinus inflammation and its associated symptom of congestion occur. Because the pathway that leads to the formation of sinonasal polyps has not been completely elucidated, effective long-term treatments remain difficult to pinpoint. Management of these polyps, therefore, is a difficult challenge for the contemporary otolaryngologist. Some of the more common medical treatment options include: topical and oral steroids; macrolide antibiotics; diuretic nasal washes; and intrapolyp steroid injection. Surgical options include polypectomy and functional endoscopic sinus surgery (FESS). In addition, novel treatments for polyps are introduced with some frequency. This article presents an overview of management options for sino- nasal polyps, focusing on the indications, efficacy, and complications of the more common interventions. DIAGNOSIS AND PREVALENCE OF SINONASAL POLYPS Diagnosis of sinonasal polyps relies primarily on nasal endoscopy, with computed tomography (CT) to evaluate the extent of disease. Although unilateral -

Anatomy, Physiology, and General Concepts in Nasal Reconstruction
Anatomy, Physiology, and General Concepts in Nasal Reconstruction Jason D. Bloom, MDa, Marcelo B. Antunes, MDb, Daniel G. Becker, MDb,* KEYWORDS Nasal reconstruction Nasal anatomy Skin physiology Wound healing Facial lines ANATOMY, PHYSIOLOGY, AND GENERAL originally determined the nasal subunits when CONCEPTS IN NASAL RECONSTRUCTION described by Gonzalez-Ulloa and colleagues.2 The thickest area is the caudal portion of the nose, Nasal reconstruction has made great strides in the on the nasal tip and ala, with its skin rich in seba- last 50 years. Nasal reconstructive surgeons have ceous glands. This nasal skin progressively gets gotten away from the idea of “filling the hole” and thinner until it reaches the rhinion, where it is the now have multiple options, which enable them to thinnest,3 and again as it transitions from the tip to achieve an aesthetically pleasing nose and good the columella and the alar rim.4,5 functional results.1 As the central and often the most noticeable feature of the face, the nose is Soft-tissue envelope also one of the most difficult to reconstruct. Nasal The soft-tissue envelope is composed of 4 layers: reconstruction requires a thorough understanding the superficial fatty layer, the fibromuscular of this complex, 3-dimensional structural and layer, the deep fatty layer, and the perichondrial/ topographic anatomy. Also, key to this type of periosteal layer.4 The superficial fatty layer is inti- surgery is the relationship of the nose to the mately connected to the dermis. Immediately surrounding tissues of the face and how these deep to this layer is the fibromuscular layer. -

Statistical Analysis Plan
Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version V1.4 Date 14 July 2017 Decline In lung-function Among Patients with chronic obstructive Lung disease On maintenance therapy (DIAPLO) An observational study evaluating the benefits of early intervention with maintenance therapies to prevent or slow down rapid lung function decline in patients who are at high risk at the time of COPD diagnosis in the combined Optimum Patient Care Research Database and Clinical Practice Research Datalink databases TITLE PAGE Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version 14 July 2017 Date 14 July 2017 TABLE OF CONTENTS PAGE TITLE PAGE ........................................................................................................... 1 TABLE OF CONTENTS ......................................................................................... 2 LIST OF ABBREVIATIONS .................................................................................. 5 RESPONSIBLE PARTIES ...................................................................................... 6 PROTOCOL SYNOPSIS DIAPLO STUDY ........................................................... 7 AMENDMENT HISTORY ................................................................................... 12 MILESTONES ....................................................................................................... 13 1. BACKGROUND AND RATIONALE .................................................................. 14 1.1 Background ........................................................................................................... -
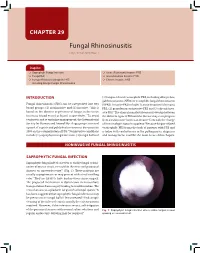
Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer
CHAPTER 29 Fungal Rhinosinusitis Eng Cern Gan, Amin R Javer Snapshot Saprophytic Fungal Infection Acute (Fulminant) Invasive FRS Fungal Ball Granulomatous Invasive FRS Fungus-Related Eosinophilic FRS Chronic Invasive FRS Including Allergic Fungal Rhinosinusitis INTRODUCTION (3) fungus-related eosinophilic FRS, including allergic fun- gal rhinosinusitis (AFRS) or eosinphilic fungal rhinosinusitis Fungal rhinosinusitis (FRS) can be categorized into two (EFRS). Invasive FRS include (1) acute invasive (fulminant) 1 broad groups: (1) noninvasive and (2) invasive. This is FRS, (2) granulomatous invasive FRS and (3) chronic inva- based on the absence or presence of fungus in the tissue sive FRS.3 The clinical manifestations may overlap between (mucosa, blood vessel or bone) respectively.2 To avoid the different types of FRS and the disease may even progress confusion and to optimize management, the International from a noninvasive form to an invasive form with the change Society for Human and Animal Mycology group convened of immunologic status in a patient.4 Because fungus-related a panel of experts and published a consensus document in eosinophilic FRS forms the bulk of patients with FRS and 2009 on the categorization of FRS.3 Noninvasive conditions is laden with controversies in the pathogenesis, diagnosis include (1) saprophytic fungal infection, (2) fungal ball and and management, it will be the main focus of this chapter. NONINVASIVE FUNGAL RHINOSINUSITIS SAPROPHYTIC FUNGAL INFECTION Saprophytic fungal infection refers to visible fungal coloni- zation of mucus crusts seen within the nose and paranasal sinuses on nasoendoscopy3,4 (Fig. 1). These patients are usually asymptomatic or may present with a foul smelling odor.2 They are likely to have had previous sinus surgery. -
Surgical Interventions for Inferior Turbinate Hypertrophy: a Comprehensive Review of Current Techniques and Technologies
International Journal of Environmental Research and Public Health Review Surgical Interventions for Inferior Turbinate Hypertrophy: A Comprehensive Review of Current Techniques and Technologies Baharudin Abdullah * and Sharanjeet Singh Department of Otorhinolaryngology-Head & Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian 16150, Kelantan, Malaysia; [email protected] * Correspondence: [email protected] Abstract: Surgical treatment of the inferior turbinates is required for hypertrophic inferior turbinates refractory to medical treatments. The main goal of surgical reduction of the inferior turbinate is to relieve the obstruction while preserving the function of the turbinate. There have been a variety of surgical techniques described and performed over the years. Irrespective of the techniques and technologies employed, the surgical techniques are classified into two types, the mucosal-sparing and non-mucosal-sparing, based on the preservation of the medial mucosa of the inferior turbinates. Although effective in relieving nasal block, the non-mucosal-sparing techniques have been associated with postoperative complications such as excessive bleeding, crusting, pain, and prolonged recovery period. These complications are avoided in the mucosal-sparing approach, rendering it the preferred option. Although widely performed, there is significant confusion and detachment between current practices and their basic objectives. This conflict may be explained by misperception over the myriad Citation: Abdullah, B.; Singh, S. Surgical Interventions for Inferior of available surgical techniques and misconception of the rationale in performing the turbinate Turbinate Hypertrophy: A reduction. A comprehensive review of each surgical intervention is crucial to better define each Comprehensive Review of Current procedure and improve understanding of the principle and mechanism involved.