2021 SMM #3 Dental Change Effective 5.1.2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
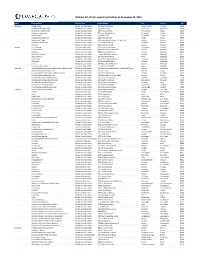
Facilities List for Website.Xlsx
Address list of Core operating facilities at December 31, 2019 State Facility Name Facility Type Street Address City County Zip Alabama Avalon Place Skilled Nursing Facility 200 Alabama Avenue Muscle Shoals Colbert 35661 Brookshire (fka Westside) Skilled Nursing Facility 4320 Judith Lane Huntsville Madison 35805 Canterbury Health Center Skilled Nursing Facility 1720 Knowles Road Phoenix City Russell 36867 Cottage of the Shoals Skilled Nursing Facility 500 John Aldridge Drive Tuscumbia Colbert 35674 Keller Landing Skilled Nursing Facility 813 Keller Lane Tuscumbia Colbert 35674 Lynwood Nursing Home Skilled Nursing Facility 4164 Halls Mill Road Mobile Mobile 36693 Merrywood Lodge Skilled Nursing Facility 280 Mount Hebron Road, P.O. Box 130 Elmore Elmore 36025 Northside Health Care Skilled Nursing Facility 700 Hutchins Avenue Gadsden Etowah 35901 River City Skilled Nursing Facility 1350 14th Avenue SE Decatur Morgan 35601 Arizona Austin House Assisted Living Facility 195 South Willard Street Cottonwood Yavapai 86326 Encanto Palms Assisted Living Facility 3901 West Encanto Boulevard Phoenix Maricopa 85009 L'Estancia Skilled Nursing Facility 15810 South 42nd Street Phoenix Maricopa 85048 Maryland Gardens Skilled Nursing Facility 31 West Maryland Avenue Phoenix Maricopa 85013 Mesa Christian Skilled Nursing Facility 255 West Brown Road Mesa Maricopa 85201 Palm Valley Skilled Nursing Facility 13575 West McDowell Road Goodyear Maricopa 85338 Ridgecrest Skilled Nursing Facility 16640 North 38th Street Phoenix Maricopa 85032 Sun City Skilled Nursing -

1. After Opening the File, Click the "Bookmark" Icon on the Left Side of the Screen
Volunteer Site Locations to File Your Taxes Yourself for Free Instructions for Creating Bookmarked State Pages: 1. After opening the file, click the "Bookmark" icon on the left side of the screen. 2. You will then see the list of state abbreviations on the left-side column; click on the page(s) that correspond to your state to find the listings for your state. 3. You can also click the Search Box above the list to look for specific information (city, zip code, etc.). Last Updated 3/2/2012 1 Volunteer Site Locations to File Your Taxes Yourself for Free Provider State County Phone Dates Languages Appointment United Bank - 137 N Main St 1/17/2012 - Atmore, AL 36502 AL Escambia (251) 446-6000 4/14/2012 English Required BancorpSouth-Roving Site- 4680 Highway 280 East 1/17/2012 - Birmingham, AL 35242 AL Shelby (205) 437-2712 4/16/2012 English Required UWCA - Main-- 3600 8TH AVE South 1/17/2012 - Birmingham, AL 35232 AL Jefferson (888) 421-1288 4/17/2012 English Required UWCA Virginia College 488 Palisades Blvd 1/23/2012 - Birmingham, AL 35209 AL Jefferson (888) 421-1266 4/17/2012 English Required Clinton L Johnson Center - 1655 Eagle Dr 1/16/2012 - Mobile, AL 36605 AL Mobile (251) 470-0372 4/17/2012 English Required Goodwill Easter Seals - Cottage Hill - 5013 Cottage Hill Road 1/17/2012 - Mobile, AL 36609 AL Mobile (251) 300-6270 4/17/2012 English Required Mobile Senior Community Center - 3201 Hillcrest Rd 2/6/2012 - Mobile, AL 36695 AL Mobile (251) 574-7787 4/16/2012 English Required CAA of Monroe County 11 Hines Street 1/16/2012 - Monroeville, -

Lower Manhattan
WASHINGTON STREET IS 131/ CANAL STREETCanal Street M1 bus Chinatown M103 bus M YMCA M NQRW (weekday extension) HESTER STREET M20 bus Canal St Canal to W 147 St via to E 125 St via 103 20 Post Office 3 & Lexington Avs VESTRY STREET to W 63 St/Bway via Street 5 & Madison Avs 7 & 8 Avs VARICK STREET B= YORK ST AVENUE OF THE AMERICAS 6 only6 Canal Street Firehouse ACE LISPENARD STREET Canal Street D= LAIGHT STREET HOLLAND AT&T Building Chinatown JMZ CANAL STREET TUNNEL Most Precious EXIT Health Clinic Blood Church COLLISTER STREET CANAL STREET WEST STREET Beach NY Chinese B BEACH STStreet Baptist Church 51 Park WALKER STREET St Barbara Eldridge St Manhattan Express Bus Service Chinese Greek Orthodox Synagogue HUDSON STREET ®0= Merchants’ Fifth Police Church Precinct FORSYTH STREET 94 Association MOTT STREET First N œ0= to Lower Manhattan ERICSSON PolicePL Chinese BOWERY Confucius M Precinct ∑0= 140 Community Plaza Center 22 WHITE ST M HUBERT STREET M9 bus to M PIKE STREET X Grand Central Terminal to Chinatown84 Eastern States CHURCH STREET Buddhist Temple Union Square 9 15 BEACH STREET Franklin Civic of America 25 Furnace Center NY Chinatown M15 bus NORTH MOORE STREET WEST BROADWAY World Financial Center Synagogue BAXTER STREET Transfiguration Franklin Archive BROADWAY NY City Senior Center Kindergarten to E 126 St FINN Civil & BAYARD STREET Asian Arts School FRANKLIN PL Municipal via 1 & 2 Avs SQUARE STREET CENTRE Center X Street Courthouse Upper East Side to FRANKLIN STREET CORTLANDT ALLEY 1 Buddhist Temple PS 124 90 Criminal Kuan Yin World -

Rockaway (Metro New York), New Jersey Rockaway the Heart of New Jersey
BUSINESS CARD DIE AREA 225 West Washington Street Indianapolis, IN 46204 (317) 636-1600 simon.com Information as of 5/1/16 Simon is a global leader in retail real estate ownership, management and development and an S&P 100 company (Simon Property Group, NYSE:SPG). ROCKAWAY (METRO NEW YORK), NEW JERSEY ROCKAWAY THE HEART OF NEW JERSEY Rockaway Townsquare serves local shoppers in Morris County, home to 496,000 people. — Morris County is the 10th most affluent county in the country, with an average annual household income of $133,000. — The center also serves Warren and Sussex Counties in New Jersey and Northeastern Pennsylvania. — The mall is within close proximity to the headquarters of Avis, Honeywell International, and Quest Diagnostics. SOMETHING FOR EVERYONE Morris County’s only super-regional mall, Rockaway Townsquare is the area’s shopping destination of choice with a diverse retail mix. — A multimillion-dollar renovation was recently completed, providing numerous upgrades and amenities as well as a completely remodeled food court. BY THE NUMBERS Anchored by Four Department Stores Lord & Taylor, Macy’s, JCPenney, Sears Square Footage Rockaway Townsquare spans 1,246,000 square feet. Two Levels Boasting more than 180 specialty stores and eateries. IN GOOD COMPANY Distinctive. Classic. Chic. Many fine brands have chosen Rockaway Townsquare as their preferred location in the Rockaway market. — Abercrombie & Fitch — Aéropostale — Build-A-Bear Workshop — Francesca’s — Hollister Co. — Modell’s Sporting Goods — Swarovski — White House I Black Market POSITIONED TO SUCCEED Rockaway Townsquare is in affluent Morris County in New Jersey, 30 miles west of Manhattan. -

Public/Private Partnership Council – Blue
DOWNLOAD THE ULI EVENTS APP – FALL MEETING Optimize your experience at ULI meetings and conferences with the free ULI Events app · Plan your schedule · Connect with other leaders at the Fall meeting · Find nearby restaurants Available for Apple and Android devices www.uli.org/mobile Public/Private Partnership Council – Blue Chair: Patricia Gage Phone: 303.383.1294 Email: [email protected] Assistant Chair: Jenna Hornstock Phone: 213.992.7437 Email: [email protected] Membership Vice Chair: Steve Elrod Phone: 312.578.6565 Email: [email protected] Vice Chair: Mark Tompkins Phone: 303. 606.4827 Email: [email protected] Vice Chair: Tom Smithgall Phone: 717.293.4403 Email: [email protected] Council Reception – October 21 st 2014 Council Reception Location: The Standard Hotel Address: 848 Washington Street at West 13 th , New York, NY 10014 Time: 6:15PM – 9:15PM Transportation: on your own RSVP contact and cost: John Basile [email protected] 301-634-8679. $150 NOTE: MEMBERS SHOULD PICK UP THEIR SUBWAY PASS FOR COUNCIL DAY AT DINNER! Council Day Agenda – October 22 nd 2014 7:30-8:00 Networking Breakfast- Corbin Building (at the Fulton Street Transit Center), 13 John Street, 3 rd floor New York, NY 10038 Directions: From 242 W42nd Street, walk one half block west on 42nd Street to 8 th Avenue. Take the A or C train downtown to Fulton Street. Exit at the rear of the train. Note that the C train has fewer cars, so you will need to continue walking to the end of the platform. At the top of the stairs, bear left up another flight of stairs to exit on Broadway near Fulton Street. -

In the United States Bankruptcy Court for the Eastern District of Virginia Richmond Division
Case 20-33332-KLP Doc 857 Filed 01/28/21 Entered 01/28/21 13:49:59 Desc Main Document Page 1 of 29 Steven N. Serajeddini, P.C. (admitted pro hac vice) Michael A. Condyles (VA 27807) KIRKLAND & ELLIS LLP Peter J. Barrett (VA 46179) KIRKLAND & ELLIS INTERNATIONAL LLP Jeremy S. Williams (VA 77469) 601 Lexington Avenue Brian H. Richardson (VA 92477) New York, New York 10022 KUTAK ROCK LLP Telephone: (212) 446-4800 901 East Byrd Street, Suite 1000 Facsimile: (212) 446-4900 Richmond, Virginia 23219-4071 Telephone: (804) 644-1700 -and- Facsimile: (804) 783-6192 David L. Eaton (admitted pro hac vice) Jaimie Fedell (admitted pro hac vice) KIRKLAND & ELLIS LLP KIRKLAND & ELLIS INTERNATIONAL LLP 300 North La Salle Street Chicago, Illinois 60654 Telephone: (312) 862-2000 Facsimile: (312) 862-2200 Co-Counsel to the Debtors and Debtors in Possession IN THE UNITED STATES BANKRUPTCY COURT FOR THE EASTERN DISTRICT OF VIRGINIA RICHMOND DIVISION ) In re: ) Chapter 11 ) LE TOTE, INC., et al.,1 ) Case No. 20-33332 (KLP) ) Debtors. ) (Jointly Administered) ) NOTICE OF FILING OF REVISED PROPOSED ORDER APPROVING THE ASSUMPTION AND ASSIGNMENT OF CERTAIN UNEXPIRED LEASE PLEASE TAKE NOTICE that on December 11, 2020, the above-captioned debtors and debtors in possession (collectively, the “Debtors”) filed the Notice of Assumption and Assignment of Unexpired Lease [Docket No. 662] (the “Notice”) with the United States Bankruptcy Court for the Eastern District of Virginia (the “Court”), which Notice includes a proposed form of order. PLEASE TAKE FURTHER NOTICE that the Debtors are hereby filing a revised proposed Order Approving the Assumption and Assignment of Certain Unexpired Lease (the “Revised Proposed Order”), which is attached hereto as Exhibit A. -

Optiplus New York State Provider List 11
Sheet1 ALBANY BRONX KINGS Albany Bronx Brooklyn Sterling Optical Sterling Optical Cohen's Fashion Optical Crossgates Mall 2168 White Plains Road 189 Montague Street 120 Washington Avenue Ext. (718) 931-0500 (718) 855-2333 (518) 456-4151 BERGEN BRONX KINGS Paramus Bronx Brooklyn Lens Lab Express of Paramus Vision Quest Optical Lens Lab Express 193 Route 17 South 880 White Plains Road 482 86th St (201) 368 -1916 (718) 239-9389 (718) 921-5488 BERGEN BRONX KINGS Bergenfield Bronx Brooklyn New Jersey Eye Center Cohen's Fashion Optical Lens Lab Express of Flatbush 1 North Washington Ave. 3416 Jerome Avenue 972 Flatbush Avenue (201) 384-7333 (718) 325-3160 (718) 826-0005 BRONX BRONX KINGS Bronx Bronx Brooklyn General Vision of Lincoln Optic Zone Lens Lab Express of Graham Avenue Hospital 2882 Third Avenue 28 Graham Ave 234 East 149th Street (718) 402-8300 (718) 486-0117 Room 2-A3 (718) 665-0611 BRONX BRONX KINGS Bronx Bronx Brooklyn Bronx Eyecare Bronx Eye Care Family Vision Center 2374 Grand Concourse 5571 Broadway 1023 Church Avenue (718) 365-6300 (718) 543-2020 (718) 826-1234 BRONX KINGS KINGS Bronx Brooklyn Brooklyn Bronx Eyecare General Vision of Flatbush Vogue Optical 2075 Bartow Avenue 2504 Flatbush Ave 3723 Nostrand Ave (718) 671-5666 (718) 253-7700 (718) 646-6200 BRONX KINGS KINGS Bronx Brooklyn Brooklyn Bronx Eyecare General Vision of Court Street Fulton Vision Center 940 Southern Boulevard 66 Court Street 519 Fulton Street (718) 328-7137 (718) 625-0025 (718) 852-7906 KINGS CAMDEN ESSEX Brooklyn Haddon Heights Irvington Mega Vision Center Dr. -

Leisure Pass Group
Explorer Guidebook Empire State Building Attraction status as of Sep 18, 2020: Open Advanced reservations are required. You will not be able to enter the Observatory without a timed reservation. Please visit the Empire State Building's website to book a date and time. You will need to have your pass number to hand when making your reservation. Getting in: please arrive with both your Reservation Confirmation and your pass. To gain access to the building, you will be asked to present your Empire State Building reservation confirmation. Your reservation confirmation is not your admission ticket. To gain entry to the Observatory after entering the building, you will need to present your pass for scanning. Please note: In light of COVID-19, we recommend you read the Empire State Building's safety guidelines ahead of your visit. Good to knows: Free high-speed Wi-Fi Eight in-building dining options Signage available in nine languages - English, Spanish, French, German, Italian, Portuguese, Japanese, Korean, and Mandarin Hours of Operation From August: Daily - 11AM-11PM Closings & Holidays Open 365 days a year. Getting There Address 20 West 34th Street (between 5th & 6th Avenue) New York, NY 10118 US Closest Subway Stop 6 train to 33rd Street; R, N, Q, B, D, M, F trains to 34th Street/Herald Square; 1, 2, or 3 trains to 34th Street/Penn Station. The Empire State Building is walking distance from Penn Station, Herald Square, Grand Central Station, and Times Square, less than one block from 34th St subway stop. Top of the Rock Observatory Attraction status as of Sep 18, 2020: Open Getting In: Use the Rockefeller Plaza entrance on 50th Street (between 5th and 6th Avenues). -
2019 Property Portfolio Simon Malls®
The Shops at Clearfork Denver Premium Outlets® The Colonnade Outlets at Sawgrass Mills® 2019 PROPERTY PORTFOLIO SIMON MALLS® LOCATION GLA IN SQ. FT. MAJOR RETAILERS CONTACTS PROPERTY NAME 2 THE SIMON EXPERIENCE WHERE BRANDS & COMMUNITIES COME TOGETHER SIMON MALLS® LOCATION GLA IN SQ. FT. MAJOR RETAILERS CONTACTS PROPERTY NAME 2 ABOUT SIMON Simon® is a global leader in retail real estate ownership, management, and development and an S&P 100 company (Simon Property Group, NYSE:SPG). Our industry-leading retail properties and investments across North America, Europe, and Asia provide shopping experiences for millions of consumers every day and generate billions in annual sales. For more information, visit simon.com. · Information as of 12/16/2019 3 SIMON MALLS® LOCATION GLA IN SQ. FT. MAJOR RETAILERS CONTACTS PROPERTY NAME More than real estate, we are a company of experiences. For our guests, we provide distinctive shopping, dining, and entertainment. For our retailers, we offer the unique opportunity to thrive in the best retail real estate in the best markets. From new projects and redevelopments to acquisitions and mergers, we are continuously evaluating our portfolio to enhance the Simon experience—places where people choose to shop and retailers want to be. 4 LOCATION GLA IN SQ. FT. MAJOR RETAILERS CONTACTS PROPERTY NAME WE DELIVER: SCALE A global leader in the ownership of premier shopping, dining, entertainment, and mixed-use destinations, including Simon Malls®, Simon Premium Outlets®, and The Mills® QUALITY Iconic, irreplaceable properties in great locations INVESTMENT Active portfolio management increases productivity and returns GROWTH Core business and strategic acquisitions drive performance EXPERIENCE Decades of expertise in development, ownership, and management That’s the advantage of leasing with Simon. -

Directory of Dental Care Providers
Table Of Contents REGION 1 ................................................. 5 Nassau County, NY .......................................... 5 Suffolk County, NY .......................................... 13 REGION 2 ................................................ 22 Bronx County, NY ........................................... 22 Kings County, NY ........................................... 26 New york County, NY ........................................ 33 Queens County, NY ......................................... 38 Richmond County, NY ........................................ 47 REGION 3 ................................................ 49 Dutchess County, NY ........................................ 49 Orange County, NY .......................................... 50 Putnam County, NY ......................................... 52 Rockland County, NY ........................................ 52 Sullivan County, NY ......................................... 55 Ulster County, NY ........................................... 55 Westchester County, NY ...................................... 55 REGION 4 ................................................ 60 Albany County, NY .......................................... 60 Clinton County, NY .......................................... 61 Columbia County, NY ........................................ 62 Essex County, NY .......................................... 62 Fulton County, NY .......................................... 62 Greene County, NY .......................................... 62 Montgomery County, -

BEEKMAN STREET !45’ WIDE" Seaport Subdistrict (ZR 91-661)
SOUTH STREET SEAPORT MUSEUM 250 WATER STREET HISTORIC DISTRICT REET SEAPORT HISTORIC D SOUTH ST ISTRICT JOHN STREET LOT 250 WATER STREET ©2020 SKIDMORE, OWINGS & MERRILL HOWARD HUGHES CORP. SOUTH STREET SEAPORT / 2 EXISTING SITE CONDITIONS THE JOHN STREET LOT 250 WATER STREET ©2020 SKIDMORE, OWINGS & MERRILL SOUTH STREET SEAPORT / 3 HOWARD HUGHES CORP. UNIQUE CONDITIONS UNIQUE OPPORTUNITY The South Street Seaport Museum • Active role to save the Historic District • Preservation of buildings and ships • Interpreter of the Historic District • Campus de!nes Historic District ©2020 SKIDMORE, OWINGS & MERRILL SOUTH STREET SEAPORT / 4 HOWARD HUGHES CORP. UNIQUE CONDITIONS UNIQUE OPPORTUNITY The South Street Seaport Museum • Active role to save the Historic District • Preservation of buildings and ships • Interpreter of the Historic District • Campus de!nes Historic District The Historic District • Rise of NYC’s shipping and !nance • 20th century planning saves the District via construction of tall buildings • Many failed attempts to support the Museum ©2020 SKIDMORE, OWINGS & MERRILL SOUTH STREET SEAPORT / 5 HOWARD HUGHES CORP. UNIQUE CONDITIONS UNIQUE OPPORTUNITY The South Street Seaport Museum • Active role to save the Historic District • Preservation of buildings and ships • Interpreter of the Historic District • Campus de!nes Historic District The Historic District 250 Water Street • Rise of NYC’s shipping and !nance • 20th century planning saves Edge location in Historic District the District via construction of • tall buildings • Vacant -

Fulton Street Transit Center Project: 3D/4D Model Application Report
CIFECENTER FOR INTEGRATED FACILITY ENGINEERING Fulton Street Transit Center Project: 3D/4D Model Application Report By Timo Hartmann, William E. Goodrich, Martin Fischer, & Doug Eberhard CIFE Technical Report #TR170 MAY 2007 STANFORD UNIVERSITY COPYRIGHT © 2007 BY Center for Integrated Facility Engineering If you would like to contact the authors, please write to: c/o CIFE, Civil and Environmental Engineering Dept., Stanford University Terman Engineering Center Mail Code: 4020 Stanford, CA 94305-4020 Fulton Street Transit Center Project: 3D/4D Model Application Report Timo Hartmann Ph.D. Student, CIFE Stanford University William E. Goodrich, P.E. Senior Project Manager, Parsons Brinckerhoff Fulton Street Project Martin Fischer Associate Professor Stanford University Doug Eberhard Chief Technology Officer Parsons Brinckerhoff 1 Executive Summary Within this report we describe the 3D/4D model implementation and application on the Fulton Street Transit Center (FSTC) project during July 2004 to July 2005. The Fulton Street Transit Center is one of the major subway reconstruction projects in New York City. With a budgeted project value of $750 Million the New York City Transit Authority (TA) plans to refurbish the seven subway lines around Fulton Street [Figure 1]. Furthermore, the TA plans to build a new above ground Transit Terminal. On this project a joint venture between Parsons Brinckerhoff and Bovis Lendlease formed the consultant construction management team to support the TA with the tasks of constructability review, bid packaging and site supervision. Figure 1: Subway Lines around Fulton Street in Lower Manhattan Early on in the project the CCM team decided to build a 3D/4D model of the project to visually support the necessary engineering decision making.