Regular Meeting of the Qi/Um Committee
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2017 Main Residency Match®
Results and Data 2017 Main Residency Match® April 2017 www.nrmp.org Requests for permission to use these data as well as questions about the content of this publication or National Resident Matching Program data may be directed to Mei Liang, Director of Research, NRMP, at [email protected]. Questions about the NRMP should be directed to Mona M. Signer, President and CEO, NRMP, at [email protected]. Suggested Citation National Resident Matching Program, Results and Data: 2017 Main Residency Match®. National Resident Matching Program, Washington, DC. 2017. Copyright © 2017 National Resident Matching Program, 2121 K Street, NW, Suite 1000, Washington, DC 20037 USA. All rights reserved. Permission to use, copy and/or distribute any documentation and/or related images from this publication shall be expressly obtained from the NRMP. NRMP Board of Directors NATIONAL RESIDENT MATCHING PROGRAM 2121 K Street, NW Suite 1000 Washington, DC 20037 The NRMP is governed by a 19-member Board of Directors, including: • Chair, Chair-Elect, and Secretary/Treasurer • Two graduate medical education program directors • Three medical students • Three resident physicians, one of whom is an international medical graduate • One public member Officers • Chair: Maria C. Savoia, M.D., Dean for Medical Education, University of California, San Diego • Chair Elect: Susan Guralnick, M.D., Associate Dean for Graduate Medical Education and Student Affairs, Winthrop University Hospital • Secretary/Treasurer: C. Bruce Alexander, M.D., Professor of Pathology, University of Alabama at Birmingham • President and Chief Executive Officer: Mona M. Signer, M.P.H., National Resident Matching Program Board Members, 2016-2017 • Maya A. Babu, M.D., MBA, Neurological Surgery Resident, Mayo Clinic • Jennifer Bai, M.D. -

Hospital Assessment - Amount Paid SFY 2020 (July 2019- June 2020)
Hospital Assessment - Amount Paid SFY 2020 (July 2019- June 2020) Hospital Name Provider Type Hospital System SFY 2020 Paid Assessment Amount ABRAZO ARROWHEAD CAMPUS Urban Acute Hospitals Abrazo Health Care$ 8,277,304 ABRAZO CENTRAL CAMPUS Urban Acute Hospitals Abrazo Health Care$ 5,988,200 ABRAZO SCOTTSDALE CAMPUS Urban Acute Hospitals Abrazo Health Care$ 3,705,416 ABRAZO WEST CAMPUS Urban Acute Hospitals Abrazo Health Care$ 6,919,768 ARIZONA GENERAL HOSPITAL Urban Acute Hospitals Dignity$ 233,840 AURORA BEHAVIORAL HEALTH Large Psychiatric Hospitals Aurora Behavioral Health System$ 648,432 AURORA BEHAVIORAL HEALTH - TEMPE Large Psychiatric Hospitals Aurora Behavioral Health System$ 472,420 BANNER - UNIVERSITY MEDICAL CENTER PHOENIX Urban Acute Hospitals Banner Health$ 15,279,028 BANNER - UNIVERSITY MEDICAL CENTER SOUTH Urban Acute Hospitals Banner Health$ 4,454,810 BANNER - UNIVERSITY MEDICAL CENTER TUCSON Pediatric-Intensive General Acute Hospitals Banner Health$ 11,791,293 BANNER BAYWOOD MEDICAL CENTER Urban Acute Hospitals Banner Health$ 10,143,600 BANNER BEHAVORIAL HEALTH MEDICAL CENTER Large Psychiatric Hospitals Banner Health$ 472,736 BANNER BOSWELL MEDICAL CENTER Urban Acute Hospitals Banner Health$ 8,121,200 BANNER CASA GRANDE MEDICAL CENTER Non-CAH Rural Acute Hospitals Banner Health$ 3,354,024 BANNER DEL E WEBB MEDICAL CENTER Urban Acute Hospitals Banner Health$ 9,183,908 BANNER DESERT MEDICAL CENTER Pediatric-Intensive General Acute Hospitals Banner Health$ 12,579,857 BANNER ESTRELLA MEDICAL CENTER Urban Acute Hospitals Banner -

AUC's 2018 Residency Report
2018 RESIDENCY MATCH The AUC alumni network grows each year as our graduates join postgraduate medical education programs throughout the United States. In 2018, more than 290 AUC graduates attained residency positions through the National Resident Matching Program® (NRMP). At AUC we remain committed to enrolling talented and committed students and providing them with the quality instruction, support, and experiences they need to reach their full potential. 217 matches throu2gh t3he programs 291 NRMP Matcsh pecialties student matches GEOGRAPHIC DISTRIBUTION PRIMARY CARE MATCHES AUC graduates earned positions in 38 U.S. states and AUC continues to contribute a significant number of the District of Columbia and will head to large university- primary care physicians to the US physician workforce affiliated academic medical centers, rural-based programs, busy urban hospitals, and major regional healthcare systems 9 6 87 2 3 Internal Family Pediatrics The most grads are headed to Medicine Medicine 60 39 33 17 13 HIGHLY COMPETITIVE SPECIALTIES* New York Michigan Florida Louisiana California and will also enter states like Mississippi, Wyoming, Nevada, Arkansas and Oklahoma where there is a great need for physicians1 Child Dermatology Emergency Neurology Medicine General Interventional Orthopedic STATES Surgery Radiology Surgery + DC 38 AUC NRMP Student Match Growth 1 9 4 2 7 7 2 6 4 0 2 2 2 2 2 1 2017 State Physician Workforce Data Book. Association of American Medical Colleges. 2018 2017 2016 2015 2014 *Highly competitive specialties are defined by the number of positions offered and the position fill rate. Data presented here reflect the official results provided by the NRMP and may not reflect residency positions attained outside the NRMP Match. -

Tenet Healthcare Annual Report 2021
Tenet Healthcare Annual Report 2021 Form 10-K (NYSE:THC) Published: February 19th, 2021 PDF generated by stocklight.com UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, DC 20549 Form 10-K ☒ Annual report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the fiscal year endedD ecember 31, 2020 OR ☐ Transition report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the transition period from to Commission File Number 1-7293 ________________________________________ TENET HEALTHCARE CORPORATION (Exact name of Registrant as specified in its charter) Nevada 95-2557091 (State of Incorporation) (IRS Employer Identification No.) 14201 Dallas Parkway Dallas, TX 75254 (Address of principal executive offices, including zip code) (469) 893-2200 (Registrant’s telephone number, including area code) ________________________________________________________ Securities registered pursuant to Section 12(b) of the Act: Title of each class Trading symbol Name of each exchange on which registered Common stock, $0.05 par value THC New York Stock Exchange 6.875% Senior Notes due 2031 THC31 New York Stock Exchange Securities registered pursuant to Section 12(g) of the Act: None ________________________________________________________ Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨ Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No x Indicate by check mark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days. -

Hospital Facilities
Cigna uses hospitalist(s) at the following hospital facilities. For information on Cigna’s participating hospitalists, please call the Member Services number on the back of your Cigna ID card. ABRAZO ARROWHEAD CAMPUS MAYO CLINIC ARIZONA ABRAZO CENTRAL CAMPUS MAYO CLINIC HOSPITAL ABRAZO SCOTTSDALE CAMPUS MERCY GILBERT MEDICAL CENTER ABRAZO WEST CAMPUS MOUNT GRAHAM REGIONAL MEDICAL CENTER BANNER BAYWOOD MEDICAL CENTER MOUNTAIN VISTA MEDICAL CENTER BANNER BAYWOOD RHODES REHAB NORTHERN COCHISE COMMUNITY HOSPITAL BANNER BOSWELL MEDICAL CENTER NORTHWEST MEDICAL CENTER BANNER CASA GRANDE MEDICAL CENTER NORTHWEST MEDICAL CENTER SAHUARITA BANNER CHILDRENS AT DESERT OASIS HOSPITAL BANNER DEL WEBB MEDICAL CENTER PAGE HOSPITAL BANNER DESERT MEDICAL CENTER PHOENIX CHILDRENS HOSPITAL BANNER ESTRELLA MEDICAL CENTER SAN JUAN REGIONAL MEDICAL CENTER BANNER GATEWAY MEDICAL CENTER SCOTTSDALE HEALTHCARE OSBORN BANNER GOLDFIELD MEDICAL CENTER SCOTTSDALE HEALTHCARE SHEA MEDICAL CENTER BANNER HEART HOSPITAL SCOTTSDALE HEALTHCARE THOMPSON PEAK BANNER IRONWOOD MEDICAL CENTER SELECT SPECIALTY HOSPITAL BANNER OCOTILLO MEDICAL CENTER ST JOSEPHS HOSPITAL & MEDICAL CENTER BANNER THUNDERBIRD MEDICAL CENTER ST LUKES MEDICAL CENTER BANNER UNIVERSITY MEDICAL CENTER PHOENIX CAMPUS SUMMIT HEALTHCARE BANNER UNIVERSITY MEDICAL CENTER SOUTH CAMPUS TEMPE ST LUKES HOSPITAL BANNER UNIVERSITY MEDICAL CENTER TUCSON CAMPUS TUCSON MEDICAL CENTER CANCER TREATMENT CENTERS OF AMERICA VALLEYWISE HEALTH CANYON VISTA MEDICAL CENTER VERDE VALLEY MEDICAL CENTER CARONDELET HOLY CROSS HOSPITAL -
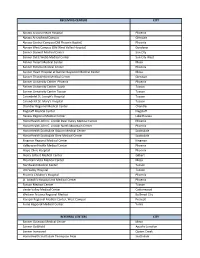
2019 List of Crcs.Xlsx
RECEIVING CENTERS CITY Abrazo Arizona Heart Hospital Phoenix Abrazo Arrowhead Campus Glendale Abrazo Central Campus (Old Phoenix Baptist) Phoenix Abrazo West Campus (Old West Valley Hospital) Goodyear Banner Boswell Medical Center Sun City Banner Del E Webb Medical Center Sun City West Banner Desert Medical Center Mesa Banner Estrella Medical Center Phoenix Banner Heart Hospital at Banner Baywood Medical Center Mesa Banner Thunderbird Medical Center Glendale Banner University Center Phoenix Phoenix Banner University Center South Tucson Banner University Center Tucson Tucson Carondelet St. Joseph's Hospital Tucson Carondelet St. Mary's Hospital Tucson Chandler Regional Medical Center Chandler Flagstaff Medical Center Flagstaff Havasu Regional Medical Center Lake Havasu HonorHealth John C. Lincoln Deer Valley Medical Center Phoenix HonorHealth John C. Lincoln North Mountain Center Phoenix HonorHealth Scottsdale Osborn Medical Center Scottsdale HonorHealth Scottsdale Shea Medical Center Scottsdale Kingman Regional Medical Center Kingman Valleywise Health Medical Center Phoenix Mayo Clinic Hospital Phoenix Mercy Gilbert Medical Center Gilbert Mountain Vista Medical Center Mesa Northwest Medical Center Tucson Oro Valley Hospital Tucson Phoenix Children's Hospital Phoenix St. Joseph's Hospital and Medical Center Phoenix Tucson Medical Center Tucson Verde Valley Medical Center Cottonwood Western Arizona Regional Medical Bullhead City Yavapai Regional Medical Center, West Campus Prescott Yuma Regional Medical Center Yuma REFERRAL CENTERS CITY Banner Gateway Medical Center Mesa Banner Goldfield Apache Junction Banner Ironwood Queen Creek HonorHealth Scottsdale Thompson Peak Scottsdale Tempe St. Lukes Hospital Tempe. -

ARIZONA FAH MEMBER FACILITIES Federation of American Hospitals Represents America’S Tax-Paying Community Hospitals and SENATE Health Systems
ARIZONA FAH MEMBER FACILITIES Federation of American Hospitals represents America’s tax-paying community hospitals and SENATE health systems. Sen. Mark Kelly (D) Sen. Kyrsten Sinema (D) HOUSE (Click name to view the district) Rep. Tom O’Halleran (D) / Arizona 1st Rep. Ann Kirkpatrick (D) / Arizona 2nd Rep. Raúl Grijalva (D) / Arizona 3rd Rep. Paul Gosar (R) / Arizona 4th Rep. Andy Biggs (R) / Arizona 5th Rep. David Schweikert (R) / Arizona 6th TOTAL Rep. Ruben Gallego (D) / Arizona 7th FACILITIES Rep. Debbie Lesko (R) / Arizona 8th Rep. Greg Stanton (D) / Arizona 9th 25 TOTAL HOSPITAL BEDS 3,482 TOTAL EMPLOYEES 13,145 FEDERATION OF AMERICAN HOSPITALS® 750 9th Street, N.W. Suite 600, Washington, DC 20001 fah.org ARIZONA FAH MEMBER FACILITIES Beds Employees REP. TOM O'HALLERAN (D) / ARIZONA 1ST 1 HOSPITAL Oro Valley Hospital Oro Valley Community Health Systems 144 612 REP. ANN KIRKPATRICK (D) / ARIZONA 2ND 6 HOSPITALS Canyon Vista Medical Center Sierra Vista LifePoint Health 100 779 Carondelet St. Joseph’s Hospital Tucson Tenet Healthcare Corporation 486 1,451 Encompass Health Rehabilitation Hospital of Northwest Tucson Encompass Health 60 171 Tucson Encompass Health Rehabilitation Institute of Tucson Tucson Encompass Health 80 241 Northwest Medical Center Tucson Community Health Systems 300 1,696 Palo Verde Hospital Tucson Universal Health Services, Inc. 84 200 REP. RAÚL GRIJALVA (D) / ARIZONA 3RD 3 HOSPITALS Carondelet Holy Cross Hospital Nogales Tenet Healthcare Corporation 25 174 Carondelet St. Mary’s Hospital Tucson Tenet Healthcare Corporation 400 1,407 Yuma Rehabilitation Hospital, a Partnership of Encompass Yuma Encompass Health 51 163 Health & YRMC REP. -

Arizona COVID-19 Cases
Arizona COVID-19 cases The Arizona Department of Health Services has reported 105,094 positive COVID-19 cases and 67,543 cases in Maricopa County as of July 7, 2020. Out of the 811,870 COVID-19 tests completed to date in Arizona, 11.3% have tested positive for the virus. Percent positive is the number of people with a positive test result, out of all the people COVID-19 tested completed in Arizona. In Maricopa County, 2,868 patients (4%) have been admitted to a hospital and 628 (1%) admitted to an ICU since the county began collecting data on Jan. 22. People aged 65 or older or those who have at least one chronic health condition make up 70% of those who have been hospitalized and 88% of deaths for COVID-19. Nearly 65% of all COVID-19 infections reported have been among those under 45 years old. Abrazo hospitals named in new ranking Top 10 Four Abrazo hospitals are named in the Arizona top 10 list of a new national hospital ranking from the Lown Institute, a nonpartisan nonprofit based in Massachusetts. Abrazo Arrowhead Campus, Abrazo Central Campus, Abrazo Scottsdale Campus and Abrazo West Campus are included in Lown Institute Hospitals Index released this week. The Index measures fall under three categories: • Civic Leadership, which assesses a commitment to equity, inclusion and community health; • Value of Care, which measures use of unnecessary services; and • Patient Outcomes, which evaluates patient outcomes, safety and satisfaction. Lown assessed nearly 3,300 hospitals on 42 metrics including data from a wide variety of sources including public records, Medicare claims, SEC filings and other databases. -

Arizona Institutional Review Board Directory
2016 Arizona Institutional Review Board Directory Arizona Biomedical Research Commission Front Cover and Section Photographs Copyright ©2013 iStockphoto LP. iStockphoto®, iStock®, iStockaudio®, iStockvideo®, iStockalypse™, Vetta® and CopySpace® are trademarks of iStockphoto LP. All other marks are the property of their respective owners. Notice The Arizona Department of Health Services does not discriminate on the basis of disability in the administration of its programs and services as prescribed by Title II of the Americans with Disabilities Act of 1990 and Section 504 of the Rehabilitation Act of 1973. If you need this publication in an alternative format, please contact: Arizona Biomedical Research Commission 250 N. 17th Ave., Phoenix, AZ 85007 (602) 364-0157 [email protected] Permission to quote from or reproduce this publication is granted when due acknowledgment is made. 2016 Arizona Institutional Review Board Directory Douglas A. Ducey Governor, State of Arizona Cara Christ, M.D. Director, Arizona Department of Health Services Commissioners Commission Staff ADHS Support Staff General Public Executive Director Administrative Services Officer Brandy Wells, M.S. Victor Waddell, Ph.D. Michelle Cardenas Cosmo Magliozzi Commission Coordinator Finance Lead John Ragan Theresa Napoleon Nikki Strattard Medical Community Program Manager John Cover Jennifer Botsford Mitchell Shub, M.D. Hugo Vargas, M.D. Scientific Community Howard Eng, DrPH 3 Table of Contents About ABRC .......................................................................................................................................................... -

Tenet Healthcare Corporation Annual Report 2020
Tenet Healthcare Corporation Annual Report 2020 Form 10-K (NYSE:THC) Published: February 24th, 2020 PDF generated by stocklight.com UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, DC 20549 Form 10-K ☒ Annual report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the fiscal year endedD ecember 31, 2019 OR ☐ Transition report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the transition period from to Commission File Number 1-7293 ________________________________________ TENET HEALTHCARE CORPORATION (Exact name of Registrant as specified in its charter) Nevada 95-2557091 (State of Incorporation) (IRS Employer Identification No.) 14201 Dallas Parkway Dallas, TX 75254 (Address of principal executive offices, including zip code) (469) 893-2200 (Registrant’s telephone number, including area code) ________________________________________________________ Securities registered pursuant to Section 12(b) of the Act: Title of each class Trading symbol Name of each exchange on which registered Common stock, $0.05 par value THC New York Stock Exchange 6.875% Senior Notes due 2031 THC31 New York Stock Exchange Securities registered pursuant to Section 12(g) of the Act: None ________________________________________________________ Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨ Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No x Indicate by check mark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days. -

2016 RESIDENCY PLACEMENTS ©2017 St
2016 RESIDENCY PLACEMENTS ©2017 St. George’s University All maps designed by Freepik. St. George’s University University Centre, Grenada, West Indies c/o University Support Services, LLC The North American Correspondent 3500 Sunrise Highway, Building 300 Great River, NY 11739 USA US/Canada Toll-Free: 1 (800) 899-6337 UK Freephone: 0800 1699061 Worldwide: +1 (631) 665-8500 Fax: +1 (631) 665-5590 [email protected] sgu.edu/md Table of Contents Residency Placements . 4 Internship . 31 Anesthesiology . 7 Neurological Surgery . 32 Child and Adolescent Psychiatry . 9 Neurology . 33 Child Neurology . 10 Obstetrics and Gynecology . 35 Diagnostic Radiology . 11 Orthopaedic Surgery . 37 Emergency Medicine . 12 Pathology . 38 Family Medicine . 14 Pediatrics . 40 Foundation . 20 Physical Medicine and Rehabilitation . 43 Internal Medicine . 21 Psychiatry . 44 Internal Medicine/Pediatrics . 29 Surgery . 47 Internal Medicine/Psychiatry . 30 Transitional Year . 50 NOTE: Residency placements in countries outside of the United States appear after state listings . Table of Contents | 1 99p0 99p0 Residency Placements In 2016, St . George’s University’s pipeline to some of the 2016 class alone, there’s Chase Dean, an orthopaedic top residency positions throughout the United States surgery resident at University of Colorado School of and Canada continued, with more than 880 residencies Medicine; Christopher McDaniel, who matched in a obtained by its students and graduates across a wide range combined internal medicine/pediatrics position at the of fields . University of Tennessee; and I-sanna Gibbons-Fideler, a pathology resident at Ohio State University Hospital East . All told, SGU is the No . 1 provider of doctors into first- They are just a few examples of SGU graduates’ success . -

Fleecing Patients: Hospitals Charge Patients More Than Four Times the Cost of Care
Fleecing Patients Hospitals Charge Patients More Than Four Times the Cost of Care November 2020 www.NationalNursesUnited.org Fleecing Patients Hospitals Charge Patients More Than Four Times the Cost of Care TABLE OF CONTENTS Summary of Findings 5 Introduction 6 Health Expenditures and the U.S. Economy 8 Rising Hospital Profits 12 Rising Hospital Prices 13 Charge-to-Cost Ratio in the United States 14 Charge-to-Cost Ratio Among Hospital Systems 19 Higher CCRs Correspond to Higher Net Income 21 Highest CCRs by State and Region 23 Beyond Charges: Other Hospital Practices to Maximize Profit 24 Conclusion 26 Appendices 27 Endnotes 88 Fleecing Patients » November 2020 3 LIST OF FIGURES AND APPENDICES Figure 1. U.S. Gross Domestic Product, 1999–2018 (page 8) Figure 2. National Health Expenditures, 1999–2018 (page 9) Figure 3. National Health Expenditure as Percentage of National Gross Domestic Product, 1999–2018 (page 9) Figure 4. National Health Expenditures Components, 2018 (page 10) Figure 5. National Hospital Expenditures, 1999–2018 (page 11) Figure 6. National Hospital Expenditures as Percentage of Health Expenditures, 1999–2018 (page 11) Figure 7. U.S. Hospitals’ Net Income, 1999–2018 (page 12) Figure 8. U.S. Hospitals’ Net Income, 1999–2018, Table (page 12) Figure 9. Consumer Price Index for Outpatient, Inpatient, and Medical Care, 1999–2018 (page 13) Figure 10. U.S. Hospitals’ Average Charge-to-Cost Ratio, 1999–2018 (page 15) Figure 11. System Owners of the Top 100 Hospitals by CCR (page 16) Figure 12. Charge-to-Cost Ratio by Provider Control Type, 2018 (page 17) Figure 13.