Obesity and Prostate Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
DNA Methylation Patterns from Peripheral Blood Separate Coronary Artery Disease Patients with and Without Heart Failure
ESC HEART FAILURE ORIGINAL RESEARCH ARTICLE ESC Heart Failure 2020; 7: 2468–2478 Published online 2 July 2020 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/ehf2.12810 DNA methylation patterns from peripheral blood separate coronary artery disease patients with and without heart failure Chris R. Bain1,2,3*†† , Mark Ziemann1,3,4,5††, Antony Kaspi1,3,4, Abdul Waheed Khan1, Rachael Taylor1, Hugh Trahair1, Ishant Khurana1,3,4, Harikrishnan Kaipananickal1,3,4,6, Sophie Wallace2,3, Assam El-Osta1,3,4,7,8, Paul S. Myles2,3 and Kiymet Bozaoglu1,9 1Baker IDI Heart and Diabetes Institute, Melbourne, VIC, Australia; 2Department of Anaesthesiology and Perioperative Medicine, The Alfred Hospital and Monash University, The Alfred Centre, Level 6, 99 Commercial Road, Melbourne, VIC 3004, Australia; 3Central Clinical School, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia; 4Epigenetics in Human Health and Disease Laboratory, Department of Diabetes, Central Clinical School, Monash University, Melbourne, VIC, Australia; 5School of Life and Environmental Sciences, Faculty of Science, Engineering and Built Environment, Deakin University, Melbourne, VIC, Australia; 6Department of Clinical Pathology, University of Melbourne, Melbourne, VIC, Australia; 7Hong Kong Institute of Diabetes and Obesity, The Chinese University of Hong Kong, Shatin, Hong Kong SAR; 8Faculty of Health, Department of Technology, Biomedical Laboratory Science, University College Copenhagen, Copenhagen, Denmark; 9Murdoch Children’s Research Institute and Department of Paediatrics, University of Melbourne, Melbourne, VIC, Australia Abstract Aims Natriuretic peptides are useful for diagnosis and prognostication of heart failure of any cause. Now, research aims to discover novel biomarkers that will more specifically define the heart failure phenotype. -

Molecular Effects of Isoflavone Supplementation Human Intervention Studies and Quantitative Models for Risk Assessment
Molecular effects of isoflavone supplementation Human intervention studies and quantitative models for risk assessment Vera van der Velpen Thesis committee Promotors Prof. Dr Pieter van ‘t Veer Professor of Nutritional Epidemiology Wageningen University Prof. Dr Evert G. Schouten Emeritus Professor of Epidemiology and Prevention Wageningen University Co-promotors Dr Anouk Geelen Assistant professor, Division of Human Nutrition Wageningen University Dr Lydia A. Afman Assistant professor, Division of Human Nutrition Wageningen University Other members Prof. Dr Jaap Keijer, Wageningen University Dr Hubert P.J.M. Noteborn, Netherlands Food en Consumer Product Safety Authority Prof. Dr Yvonne T. van der Schouw, UMC Utrecht Dr Wendy L. Hall, King’s College London This research was conducted under the auspices of the Graduate School VLAG (Advanced studies in Food Technology, Agrobiotechnology, Nutrition and Health Sciences). Molecular effects of isoflavone supplementation Human intervention studies and quantitative models for risk assessment Vera van der Velpen Thesis submitted in fulfilment of the requirements for the degree of doctor at Wageningen University by the authority of the Rector Magnificus Prof. Dr M.J. Kropff, in the presence of the Thesis Committee appointed by the Academic Board to be defended in public on Friday 20 June 2014 at 13.30 p.m. in the Aula. Vera van der Velpen Molecular effects of isoflavone supplementation: Human intervention studies and quantitative models for risk assessment 154 pages PhD thesis, Wageningen University, Wageningen, NL (2014) With references, with summaries in Dutch and English ISBN: 978-94-6173-952-0 ABSTRact Background: Risk assessment can potentially be improved by closely linked experiments in the disciplines of epidemiology and toxicology. -
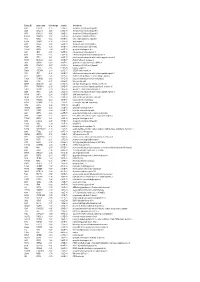
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

Content Based Search in Gene Expression Databases and a Meta-Analysis of Host Responses to Infection
Content Based Search in Gene Expression Databases and a Meta-analysis of Host Responses to Infection A Thesis Submitted to the Faculty of Drexel University by Francis X. Bell in partial fulfillment of the requirements for the degree of Doctor of Philosophy November 2015 c Copyright 2015 Francis X. Bell. All Rights Reserved. ii Acknowledgments I would like to acknowledge and thank my advisor, Dr. Ahmet Sacan. Without his advice, support, and patience I would not have been able to accomplish all that I have. I would also like to thank my committee members and the Biomed Faculty that have guided me. I would like to give a special thanks for the members of the bioinformatics lab, in particular the members of the Sacan lab: Rehman Qureshi, Daisy Heng Yang, April Chunyu Zhao, and Yiqian Zhou. Thank you for creating a pleasant and friendly environment in the lab. I give the members of my family my sincerest gratitude for all that they have done for me. I cannot begin to repay my parents for their sacrifices. I am eternally grateful for everything they have done. The support of my sisters and their encouragement gave me the strength to persevere to the end. iii Table of Contents LIST OF TABLES.......................................................................... vii LIST OF FIGURES ........................................................................ xiv ABSTRACT ................................................................................ xvii 1. A BRIEF INTRODUCTION TO GENE EXPRESSION............................. 1 1.1 Central Dogma of Molecular Biology........................................... 1 1.1.1 Basic Transfers .......................................................... 1 1.1.2 Uncommon Transfers ................................................... 3 1.2 Gene Expression ................................................................. 4 1.2.1 Estimating Gene Expression ............................................ 4 1.2.2 DNA Microarrays ...................................................... -

Original Article Dysregulated Expression of Micrornas and Mrnas in Myocardial Infarction
Am J Transl Res 2015;7(11):2291-2304 www.ajtr.org /ISSN:1943-8141/AJTR0012948 Original Article Dysregulated expression of microRNAs and mRNAs in myocardial infarction Yaping Wang1,2, Xiaohong Pan1, Youqi Fan1, Xinyang Hu1,2, Xianbao Liu1,2, Meixiang Xiang1,2, Jian’an Wang1,2 1Department of Cardiology, Second Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310009, PR China; 2Key Lab of Cardiovascular Disease, Second Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310009, PR China Received July 15, 2015; Accepted October 31, 2015; Epub November 15, 2015; Published November 30, 2015 Abstract: Acute myocardial infarction (AMI) is a major cause of mortality in the general population. However, the molecular phenotypes and therapeutic targets of AMI patients remain unclear. By profiling genome-wide transcripts and microRNAs (miRNAs) in a cohort of 23 AMI patients and 23 non-AMI patients, we found 218 dysregulated genes identified in the infarcted heart tissues from AMI patients relative to non-AMI controls. Pathway enrichment analy- sis of the dysregulated genes pointed to cell signaling/communication, cell/organism defense and cell structure/ motility. We next compared the expression profiles of potential regulating miRNAs, suggesting that dysregulation of a number of AMI-associated genes (e.g., IL12A, KIF1A, HIF1α and CDK13) may be attributed to the dysregulation of their respective regulating miRNAs. One potentially pathogenic miRNA-mRNA pair, miR-210-HIF1α, was confirmed in a mouse model of myocardial infarction (MI). Inhibition of miR-210 expression improved the survival and cardiac function of MI mice. In conclusion, we presented the pathologic relationships between miRNAs and their gene targets in AMI. -

Microarray Bioinformatics and Its Applications to Clinical Research
Microarray Bioinformatics and Its Applications to Clinical Research A dissertation presented to the School of Electrical and Information Engineering of the University of Sydney in fulfillment of the requirements for the degree of Doctor of Philosophy i JLI ··_L - -> ...·. ...,. by Ilene Y. Chen Acknowledgment This thesis owes its existence to the mercy, support and inspiration of many people. In the first place, having suffering from adult-onset asthma, interstitial cystitis and cold agglutinin disease, I would like to express my deepest sense of appreciation and gratitude to Professors Hong Yan and David Levy for harbouring me these last three years and providing me a place at the University of Sydney to pursue a very meaningful course of research. I am also indebted to Dr. Craig Jin, who has been a source of enthusiasm and encouragement on my research over many years. In the second place, for contexts concerning biological and medical aspects covered in this thesis, I am very indebted to Dr. Ling-Hong Tseng, Dr. Shian-Sehn Shie, Dr. Wen-Hung Chung and Professor Chyi-Long Lee at Change Gung Memorial Hospital and University of Chang Gung School of Medicine (Taoyuan, Taiwan) as well as Professor Keith Lloyd at University of Alabama School of Medicine (AL, USA). All of them have contributed substantially to this work. In the third place, I would like to thank Mrs. Inge Rogers and Mr. William Ballinger for their helpful comments and suggestions for the writing of my papers and thesis. In the fourth place, I would like to thank my swim coach, Hirota Homma. -

FLAME: a Web Tool for Functional and Literature Enrichment Analysis of Multiple Gene Lists
bioRxiv preprint doi: https://doi.org/10.1101/2021.06.02.446692; this version posted June 2, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. FLAME: a web tool for functional and literature enrichment analysis of multiple gene lists Foteini Thanati1,†, Evangelos Karatzas1,†, Fotis A. Baltoumas1, Dimitrios J. Stravopodis2, Aristides G. Eliopoulos3,4,5, Georgios A. Pavlopoulos1,4,* 1 Institute for Fundamental Biomedical Research, BSRC "Alexander Fleming", Athens, Greece 2 Department of Biology, National and Kapodistrian University of Athens, Athens, Greece 3 Department of Biology, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece 4 Center for New Biotechnologies and Precision Medicine, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece 5 Center of Basic Research, Biomedical Research Foundation of the Academy of Athens, Athens, Greece †Equally contributing authors *To whom correspondence should be addressed. Tel: +30-210-9656310; Fax: +30-210-9653934; Email: [email protected] Present Address: Georgios A. Pavlopoulos, Institute for Fundamental Biomedical Research, BSRC "Alexander Fleming", 34 Fleming Street, Vari, 16672, Greece ABSTRACT Functional enrichment is a widely used method for interpreting experimental results by identifying classes of proteins/genes associated with certain biological functions, pathways, diseases or phenotypes. Despite the variety of existing tools, most of them can process a single list per time, thus making a more combinatorial analysis more complicated and prone to errors. In this article, we present FLAME, a web tool for combining multiple lists prior to enrichment analysis. -

Integrative Personal Omics Profiles During Periods of Weight Gain And
Article Integrative Personal Omics Profiles during Periods of Weight Gain and Loss Graphical Abstract Authors Brian D. Piening, Wenyu Zhou, Ke´ vin Contrepois, ..., Tracey L. McLaughlin, George M. Weinstock, Michael P. Snyder Correspondence [email protected] (T.L.M.), [email protected] (G.M.W.), [email protected] (M.P.S.) In Brief Extensive multi-omic profiling of the blood and microbiomes of healthy and insulin-resistant humans as they gain and lose weight reveals insights into the systemic impacts of weight gain. Highlights d Analysis of insulin-sensitive and -resistant individuals across multiple omes d We reveal molecular changes in the human body after modest short-term weight gain d Reversal of short-term weight gain eliminates negative molecular alterations d Open-access multi-omic resource for further bioinformatics developments Piening et al., 2018, Cell Systems 6, 1–14 February 28, 2018 ª 2017 Elsevier Inc. https://doi.org/10.1016/j.cels.2017.12.013 Please cite this article in press as: Piening et al., Integrative Personal Omics Profiles during Periods of Weight Gain and Loss, Cell Systems (2017), https://doi.org/10.1016/j.cels.2017.12.013 Cell Systems Article Integrative Personal Omics Profiles during Periods of Weight Gain and Loss Brian D. Piening,1,16 Wenyu Zhou,1,16 Ke´ vin Contrepois,1,16 Hannes Ro¨ st,1,16 Gucci Jijuan Gu Urban,1,10 Tejaswini Mishra,1 Blake M. Hanson,2 Eddy J. Bautista,2,15 Shana Leopold,2 Christine Y. Yeh,1,4,5,11 Daniel Spakowicz,2 Imon Banerjee,12 Cynthia Chen,12 Kimberly Kukurba,1 Dalia Perelman,3 Colleen Craig,3 Elizabeth Colbert,3 Denis Salins,1 Shannon Rego,1 Sunjae Lee,7 Cheng Zhang,7 Jessica Wheeler,1 M. -

Identification of Novel Regulatory Genes in Acetaminophen
IDENTIFICATION OF NOVEL REGULATORY GENES IN ACETAMINOPHEN INDUCED HEPATOCYTE TOXICITY BY A GENOME-WIDE CRISPR/CAS9 SCREEN A THESIS IN Cell Biology and Biophysics and Bioinformatics Presented to the Faculty of the University of Missouri-Kansas City in partial fulfillment of the requirements for the degree DOCTOR OF PHILOSOPHY By KATHERINE ANNE SHORTT B.S, Indiana University, Bloomington, 2011 M.S, University of Missouri, Kansas City, 2014 Kansas City, Missouri 2018 © 2018 Katherine Shortt All Rights Reserved IDENTIFICATION OF NOVEL REGULATORY GENES IN ACETAMINOPHEN INDUCED HEPATOCYTE TOXICITY BY A GENOME-WIDE CRISPR/CAS9 SCREEN Katherine Anne Shortt, Candidate for the Doctor of Philosophy degree, University of Missouri-Kansas City, 2018 ABSTRACT Acetaminophen (APAP) is a commonly used analgesic responsible for over 56,000 overdose-related emergency room visits annually. A long asymptomatic period and limited treatment options result in a high rate of liver failure, generally resulting in either organ transplant or mortality. The underlying molecular mechanisms of injury are not well understood and effective therapy is limited. Identification of previously unknown genetic risk factors would provide new mechanistic insights and new therapeutic targets for APAP induced hepatocyte toxicity or liver injury. This study used a genome-wide CRISPR/Cas9 screen to evaluate genes that are protective against or cause susceptibility to APAP-induced liver injury. HuH7 human hepatocellular carcinoma cells containing CRISPR/Cas9 gene knockouts were treated with 15mM APAP for 30 minutes to 4 days. A gene expression profile was developed based on the 1) top screening hits, 2) overlap with gene expression data of APAP overdosed human patients, and 3) biological interpretation including assessment of known and suspected iii APAP-associated genes and their therapeutic potential, predicted affected biological pathways, and functionally validated candidate genes. -

A Meta-Analysis of the Effects of High-LET Ionizing Radiations in Human Gene Expression
Supplementary Materials A Meta-Analysis of the Effects of High-LET Ionizing Radiations in Human Gene Expression Table S1. Statistically significant DEGs (Adj. p-value < 0.01) derived from meta-analysis for samples irradiated with high doses of HZE particles, collected 6-24 h post-IR not common with any other meta- analysis group. This meta-analysis group consists of 3 DEG lists obtained from DGEA, using a total of 11 control and 11 irradiated samples [Data Series: E-MTAB-5761 and E-MTAB-5754]. Ensembl ID Gene Symbol Gene Description Up-Regulated Genes ↑ (2425) ENSG00000000938 FGR FGR proto-oncogene, Src family tyrosine kinase ENSG00000001036 FUCA2 alpha-L-fucosidase 2 ENSG00000001084 GCLC glutamate-cysteine ligase catalytic subunit ENSG00000001631 KRIT1 KRIT1 ankyrin repeat containing ENSG00000002079 MYH16 myosin heavy chain 16 pseudogene ENSG00000002587 HS3ST1 heparan sulfate-glucosamine 3-sulfotransferase 1 ENSG00000003056 M6PR mannose-6-phosphate receptor, cation dependent ENSG00000004059 ARF5 ADP ribosylation factor 5 ENSG00000004777 ARHGAP33 Rho GTPase activating protein 33 ENSG00000004799 PDK4 pyruvate dehydrogenase kinase 4 ENSG00000004848 ARX aristaless related homeobox ENSG00000005022 SLC25A5 solute carrier family 25 member 5 ENSG00000005108 THSD7A thrombospondin type 1 domain containing 7A ENSG00000005194 CIAPIN1 cytokine induced apoptosis inhibitor 1 ENSG00000005381 MPO myeloperoxidase ENSG00000005486 RHBDD2 rhomboid domain containing 2 ENSG00000005884 ITGA3 integrin subunit alpha 3 ENSG00000006016 CRLF1 cytokine receptor like -

Enhancer Variants Associated With
Kikuchi et al. BMC Medical Genomics (2019) 12:128 https://doi.org/10.1186/s12920-019-0574-8 RESEARCH ARTICLE Open Access Enhancer variants associated with Alzheimer’s disease affect gene expression via chromatin looping Masataka Kikuchi1* , Norikazu Hara2, Mai Hasegawa1, Akinori Miyashita2, Ryozo Kuwano2,3, Takeshi Ikeuchi2 and Akihiro Nakaya1* Abstract Background: Genome-wide association studies (GWASs) have identified single-nucleotide polymorphisms (SNPs) that may be genetic factors underlying Alzheimer’s disease (AD). However, how these AD-associated SNPs (AD SNPs) contribute to the pathogenesis of this disease is poorly understood because most of them are located in non-coding regions, such as introns and intergenic regions. Previous studies reported that some disease-associated SNPs affect regulatory elements including enhancers. We hypothesized that non-coding AD SNPs are located in enhancers and affect gene expression levels via chromatin loops. Methods: To characterize AD SNPs within non-coding regions, we extracted 406 AD SNPs with GWAS p-values of less than 1.00 × 10− 6 from the GWAS catalog database. Of these, we selected 392 SNPs within non-coding regions. Next, we checked whether those non-coding AD SNPs were located in enhancers that typically regulate gene expression levels using publicly available data for enhancers that were predicted in 127 human tissues or cell types. We sought expression quantitative trait locus (eQTL) genes affected by non-coding AD SNPs within enhancers because enhancers are regulatory elements that influence the gene expression levels. To elucidate how the non- coding AD SNPs within enhancers affect the gene expression levels, we identified chromatin-chromatin interactions by Hi-C experiments. -
Systematic Bromodomain Protein Screens Identify Homologous Recombination and R-Loop Suppression Pathways Involved in Genome Integrity
Downloaded from genesdev.cshlp.org on October 5, 2021 - Published by Cold Spring Harbor Laboratory Press RESOURCE/METHODOLOGY Systematic bromodomain protein screens identify homologous recombination and R-loop suppression pathways involved in genome integrity Jae Jin Kim,1,2,9 Seo Yun Lee,1,2,9 Fade Gong,1,2,8 Anna M. Battenhouse,1,2,3 Daniel R. Boutz,1,2,3 Aarti Bashyal,4 Samantha T. Refvik,1,2,5 Cheng-Ming Chiang,6 Blerta Xhemalce,1,2,7 Tanya T. Paull,1,2,5,7 Jennifer S. Brodbelt,4,7 Edward M. Marcotte,1,2,3 and Kyle M. Miller1,2,7 1Department of Molecular Biosciences, 2Institute for Cellular and Molecular Biology, 3Center for Systems and Synthetic Biology, 4Department of Chemistry, The University of Texas at Austin, Austin, Texas 78712, USA; 5The Howard Hughes Medical Institute; 6Simmons Comprehensive Cancer Center, Department of Biochemistry, Department of Pharmacology, University of Texas Southwestern Medical Center, Dallas, Texas 75390, USA; 7Livestrong Cancer Institutes, Dell Medical School, The University of Texas at Austin, Austin, Texas 78712, USA Bromodomain proteins (BRD) are key chromatin regulators of genome function and stability as well as therapeutic targets in cancer. Here, we systematically delineate the contribution of human BRD proteins for genome stability and DNA double-strand break (DSB) repair using several cell-based assays and proteomic interaction network analysis. Applying these approaches, we identify 24 of the 42 BRD proteins as promoters of DNA repair and/or ge- nome integrity. We identified a BRD-reader function of PCAF that bound TIP60-mediated histone acetylations at DSBs to recruit a DUB complex to deubiquitylate histone H2BK120, to allowing direct acetylation by PCAF, and repair of DSBs by homologous recombination.