Understanding Service Needs of Under Five Year Olds
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

West Midlands Police and Crime Commissioner Register of Gifts And
West Midlands Police and Crime Commissioner Register of Gifts and Hospitality - Police and Crime Commissioner and Deputy Police and Crime Commissioner Note: This register contains details of declarations made by the PCC and DPCC and includes details of offers of gifts and hospitality not accepted Name Name of person or organisation Details of Gift or hospitality Estimate of value Date offer received Comments Funeral for Don Jones partner to Cllr Diana refreshments offered after Bob Jones Holl-Allen funeral £10.00 23/11/2012 declined passed to office staff for Bob Jones Harmeet Singh Bhakna Punjabi News Indian Sweets £5.00 23/11/2012 consumption Bob Jones Asian Business Forum Samosas and pakoras offered £7.00 28/11/2012 refreshments consumed Bob Jones Home office PCC welcome Buffet lunch provided £7.00 03/12/2012 refreshments consumed Bob Jones APPG on Polcing meeting Buffett and wine offered £10.00 03/12/2012 buffet consumed, wine declined Bob Jones Connect Public Affairs lunch buffet offered £12.00 04/12/2012 Buffet consumed Annual Karate Awards presentation Bob Jones evening food and drink offered £12.00 07/12/2012 food and drink declined invite to Brisitsh Police Symphony Orchestra BPSO accepted but ticket unavailable on Yvonne Mosquito Steria sponsors Proms night special £21.00 08/12/2012 the evening Gavin Chapman and John Torrie - Steria Invite to supper at Hotel du Vin Yvonne Mosquito sponsors flollowing BPSO Proms £30.00 08/12/2012 declined Christmas lunch and drink offered. Small comemorative food consumed, Alcohol declined, Bob -

Birmingham Mental Health Recovery and Employment Service Prospectus - 2018
Birmingham Mental Health Recovery and Employment Service Prospectus - 2018 Hope - Control - Opportunity Birmingham Mental Health Recovery Service The Recovery Service offers recovery and wellbeing sessions to support mental, physical and emotional wellbeing in shared learning environments in the community. It will support people to identify and build on their own strengths and make sense of their experiences. This helps people take control, feel hopeful and become experts in their own wellbeing and recovery. Education and Shared Learning The Recovery Service provides an enablement approach to recovery, with an aim to empower people to live well through shared learning. As human beings we all experience our own personal recovery journeys and can benefit greatly from sharing and learning from each other in a safe and equal space. Co-production We aim for all courses to be developed and/or delivered in partnership with people who have lived experience (i.e. of mental health issues and/ or learning disabilities) or knowledge of caring for someone with these experiences. This model of shared learning allows for rich and diverse perspectives on living well with mental health or related issues. Eligibility This service shall be provided to service users who are: • Aged 18 years and above • Registered with a Birmingham GP for whom the commissioner is responsible for funding healthcare services • Residents of Birmingham registered with GP practices within Sandwell and West Birmingham CCG • Under the care of secondary mental health services or on the GP Serious Mental Illness register. Principles of Participation 1. Treat all service users and staff with compassion, dignity and respect and to not discriminate against or harass others at any time, respecting their rights, life choices, beliefs and opinions. -

4506 18 Draft Attachment 01.Pdf
West Midlands Police Freedom of Information POLICE STATIONS & BEAT OFFICES CLOSED SINCE APRIL 2010 DATE CURRENT CLOSED PROPERTY ADDRESS STATUS 20/05/2010 BORDESLEY GREEN POLICE STATION 280-282 Bordesley Green, Birmingham B9 5NA SOLD 20/5/10 27/07/2010 NORTHGATE BO 32 Northgate, Cradley Heath B64 6AU AGREEMENT TERMINATED 01/08/2010 BRAMFORD PRIMARY SCHOOL BO Park Road, Woodsetton, Dudley DY1 4JH AGREEMENT TERMINATED ST THOMAS'S COMMUNITY NETWORK 01/08/2010 Beechwood Road, Dudley DY2 7QA AGREEMENT TERMINATED BO 22/09/2010 WALKER ROAD BO 115 Walker Road, Blakenall, Walsall WS3 1DB AGREEMENT TERMINATED 23/09/2010 GREENFIELD CRESCENT BO 10 Greenfield Crescent, Edgbaston, Birmingham B15 3AU AGREEMENT TERMINATED 26/10/2010 EVERDON ROAD BO 40 Everdon Road, Coventry CV6 4EF AGREEMENT TERMINATED 08/11/2010 MERRY HILL BO Unit U56B Upper Mall Phase 5, Merry Hill Centre, Dudley DY5 1QX AGREEMENT TERMINATED 03/02/2011 COURTAULDS BO 256 Foleshill Road, Great Heath, Coventry CV6 5AB AGREEMENT TERMINATED 25/02/2011 ASTON FIRE STATION NURSERY BO The Nursery Building, Ettington Road, Aston, Birmingham B6 6ED AGREEMENT TERMINATED 28/02/2011 BLANDFORD ROAD BO 125 Blandford Road, Quinton, Birmingham B32 2LT AGREEMENT TERMINATED 05/04/2011 LOZELLS ROAD BO 173A Lozells Road, Lozells, Birmingham B19 1RN AGREEMENT TERMINATED 30/06/2011 LANGLEY BO Albright & Wilson, Station Road, Langley, Oldbury B68 0NN AGREEMENT TERMINATED BILSTON POLICE STATION 10/08/2011 15 Mount Pleasant, Bilston WV14 7LJ SOLD 10/8/11 (old) HOLLYHEDGE HOUSE & MEWS 05/09/2011 2 Hollyhedge Road, -

Warding Arrangements for Legend Ladywood Ward
Newtown Warding Arrangements for Soho & Jewellery Quarter Ladywood Ward Legend Nechells Authority boundary Final recommendation North Edgbaston Ladywood Bordesley & Highgate Edgbaston 0 0.1 0.2 0.4 Balsall Heath West Kilometers Contains OS data © Crown copyright and database right 2016. $ Bournville & Cotteridge Allens Cross Warding Arrangements for Longbridge & West Heath Ward Legend Frankley Great Park Northfield Authority boundary King's Norton North Final recommendation Longbridge & West Heath King's Norton South Rubery & Rednal 0 0.15 0.3 0.6 Kilometers Contains OS data © Crown copyright and database right 2016. $ Warding Arrangements for Lozells Ward Birchfield Legend Authority boundary Final recommendation Aston Handsworth Lozells Soho & Jewellery Quarter Newtown 0 0.05 0.1 0.2 Kilometers Contains OS data © Crown copyright and database right 2016. $ Small Heath Sparkbrook & Balsall Heath East Tyseley & Hay Mills Warding Balsall Heath West Arrangements for Moseley Ward Edgbaston Legend Authority boundary Final recommendation Sparkhill Moseley Bournbrook & Selly Park Hall Green North Brandwood & King's Heath Stirchley Billesley 0 0.15 0.3 0.6 Kilometers Hall Green South Contains OS data © Crown copyright and database right 2016. $ Perry Barr Stockland Green Warding Pype Hayes Arrangements for Gravelly Hill Nechells Ward Aston Legend Authority boundary Final recommendation Bromford & Hodge Hill Lozells Ward End Nechells Newtown Alum Rock Glebe Farm & Tile Cross Soho & Jewellery Quarter Ladywood Heartlands Bordesley & Highgate 0 0.15 0.3 0.6 Kilometers Bordesley Green Contains OS data © Crown copyright and database right 2016. $ Small Heath Handsworth Aston Warding Lozells Arrangements for Newtown Ward Legend Authority boundary Final recommendation Newtown Nechells Soho & Jewellery Quarter 0 0.075 0.15 0.3 Ladywood Kilometers Contains OS data © Crown copyright and database Ladywood right 2016. -

8A Bus Time Schedule & Line Route
8A bus time schedule & line map 8A Birmingham Inner Circle Anticlockwise View In Website Mode The 8A bus line Birmingham Inner Circle Anticlockwise has one route. For regular weekdays, their operation hours are: (1) Saltley: 4:49 AM - 11:46 PM Use the Moovit App to ƒnd the closest 8A bus station near you and ƒnd out when is the next 8A bus arriving. Direction: Saltley 8A bus Time Schedule 49 stops Saltley Route Timetable: VIEW LINE SCHEDULE Sunday 6:59 AM - 11:46 PM Monday 4:49 AM - 11:46 PM Alum Rock Rd, Saltley Adderley Road, Birmingham Tuesday 4:49 AM - 11:46 PM Saltley Trading Estate, Saltley Wednesday 4:49 AM - 11:46 PM Hereford Square, Birmingham Thursday 4:49 AM - 11:46 PM Nechells Place, Saltley Friday 4:49 AM - 11:46 PM 1 Mainstream Way, Birmingham Saturday 4:49 AM - 11:46 PM Goodrick Way, Nechells Green Lingard Close, Birmingham Nechells Police Station, Saltley Nechells Place, Birmingham 8A bus Info Direction: Saltley Cromwell St, Nechells Green Stops: 49 Trip Duration: 57 min Cheston Rd, Aston Line Summary: Alum Rock Rd, Saltley, Saltley William Henry street, Birmingham Trading Estate, Saltley, Nechells Place, Saltley, Goodrick Way, Nechells Green, Nechells Police Aston Cross, Aston Station, Saltley, Cromwell St, Nechells Green, Cheston 1 Rocky lane, Birmingham Rd, Aston, Aston Cross, Aston, Upper Sutton St, Aston, Selston Rd, Newtown, Alma St, Newtown, Upper Sutton St, Aston Holte School, Newtown, Lozells St, Lozells, Church Dunsfold Croft, Birmingham St, Hockley, Hockley Circus, Hockley, Barr Street, Hockley, Unett St, Hockley, -

COVID Enforcement Patrols Regular Enforcement Patrols Are Undertaken to Ensure Businesses Are Complying with Coronavirus Legislation
COVID Marshals • 25 COVID Marshals and 8 Park Marshals employed since November providing a hi-vis presence on the street. • Visiting all Wards but are particularly focusing on those with the highest infection rates. • Assisting with surge testing in Great Park and Frankley. • Providing advice to businesses on good practice and to citizens on the use of face coverings. • Eyes and ears for Enforcement Team providing valuable feedback on businesses who are not complying with the legislation so that enforcement work can be prioritised. • Large number of “free” face coverings are being distributed by the COVID Marshals on a daily basis. To date over 18,500 face coverings have been distributed. • Public interactions has now a last fallen considerably since the latest lockdown was introduced. (mid Jan-Feb) • Enclosed shopping centres found to have the highest level of non-compliance with regards to the wearing of face coverings. • Between the 16th Jan and 14th Feb the majority of face coverings (40% - 1,345) were distributed in the City Centre. • 446 masks were distributed by the Park COVID Marshals (13%). PA F 1 1 1 1 1 20 12 20 40 60 80 0 2 4 6 8 GE th 0 0 0 0 0 0 0 ace J a 3 n – 14 Acocks Green th Fe Alum Rock b co ( e Aston x c lu Billesley d in v g Bordesley & Highgate L a erings d ywoo Bordesley Green Bournville & Cotteridge d ) Brandwood & King's Heath Bromford & Hodge Hill Castle Vale Erdington distri Frankley Great Park Gravelly Hill Hall Green North Hall Green South but Handsworth Handsworth Wood Harborne ed Holyhead King's Norton North b King's Norton South y w Kingstanding Longbridge & West Heath Lozells ar Moseley Newtown d b Northfield Perry Barr y CO Perry Common Pype Hayes Sheldon Small Heath VID Soho & Jewellery Quarter South Yardley Sparkbrook & Balsall Heath East Marshals Sparkhill Stirchley Sutton Four Oaks Sutton Mere Green Sutton Trinity Sutton Vesey Tyseley & Hay Mills Weoley & Selly Oak Yardley West & Stechford PA public No 1 1 2 2 3 3 4 12 50 0 5 0 5 0 5 0 GE th 0 0 0 0 0 0 0 0 Jan 4 . -

Newtown, Oscott, Perry Barr, Soho, Oldbury
Equality and Diversity Strategy ASTON, HANDSWORTH, JEWELLERY QUARTER, LOZELLS, NECHELLS, NEWTOWN, OSCOTT, PERRY BARR, SOHO, OLDBURY, ROWLEY REGIS, TIPTON, SMETHWICK, WEST BROMWICH ASTON, HANDSWORTH, JEWELLERY QUARTER, LOZELLS, NECHELLS, NEWTOWN, OSCOTT, PERRY BARR, SOHO, OLDBURY, ROWLEY REGIS, TIPTON, SMETHWICK, WEST BROMWICH ASTON, HANDSWORTH, JEWELLERY QUARTER, LOZELLS, NECHELLS, NEWTOWN, OSCOTT, PERRY BARR, SOHO, OLDBURY, ROWLEY REGIS, TIPTON, SMETHWICK, WEST BROMWICH ASTON, HANDSWORTH, JEWELLERY QUARTER, LOZELLS, NECHELLS, NEWTOWN, OSCOTT, PERRY BARR, SOHO, OLDBURY, ROWLEY REGIS, TIPTON, SMETHWICK, WEST BROMWICH ASTON, HANDSWORTH, JEWELLERY QUARTER, LOZELLS, NECHELLS, NEWTOWN, OSCOTT, PERRY BARR, SOHO, OLDBURY, ROWLEY REGIS, TIPTON, SMETHWICK, WEST BROMWICH C5206 GUJARATI Translation 1A ùf PYf #e `eQf WhMf¶\ R¶ÀPe]fHÌ T ]epFh ^A¶ef, Pef Ao¶Ue A¶[l YR¶R¶ Yfb]]e YeKf¶ #pCyfú C5206Wef\h ^Af¶ Pf]h A¶ef$ ½Zz¡PþTf #alò #eUf\e Kf¶z\þVeüT TpW[ U[ VeüT A¶[]e z]þTpPhFrench A¶[ef .................... TranslationC5206 1A BENGALI SiTranslation vous ne 1Apouvez pas lire le document ci-joint, veuillez demander Translation 1B C5206àIf youquelqu'un can not read qui the parle attached anglais document, d'appeler please get ce someone numéro who pour speaks obtenir EnglishPolish deto ring l’aidethis number ………………………… for help ………………………… ùf PYf #e `eQf WhMf¶\ R¶ÀPe]fHÌ T ]epFh ^A¶ef, Pef Ao¶Ue A¶[l YR¶R¶ Yfb]]e YeKf¶ #pCyfú TranslationåKAeM^Wef\h ^Af¶ svzuË Pf]h 1B1A A¶ef$ kAgj-pñAif^ ½Zz¡PþTf &U[ ÁpiM^ HÌOe]f\e pxew^ Kf¶z\þVeüT Mo pArel^, TpW[ U[ áMugòh VeüT A¶[]e ker^ z]þTpPhsAhAezù^r A¶[ef. jMù éver^jI blew^ pAer^M åmM kAõek^ if^ey^ ............................... -

West Midlands Police ,~, "
eA~If you have issues viewing or accessing this file contact us at NCJRS.gov. '1- Z-9' -& '-- ~t, REPORT OF THE CHIEF CONSTABLE .Report OF THE WEST MIDLANDS POLICE ,~, ", FOR THE OF YEAR 1981 .. 'T':-'f. CHIEF CONSTABLE c::) I o o co I CY") OF THE co , ,-t' ,1' /1 t WEST MIDLANDS POLICE I, ; Chief Constable's Office " Lloyd House ;:, '. .1/' ,.~ Co/more Circus Oueensway i 1 -: , t'l Birmingham B46NO I) ( . 1 \.' ..J. • '''1 '.1 c ; 1", r' , :', L') ~_ " "I 1981 11' Ql'" 1..l' : L_ ;. tf" '+(' t- L :.' (' ll_ :") I ! WEST MIDLANDS POLICE , Police Headquarters Lloyd House Colmore Circus Queensway Telephone No. 021-236 5000 Birmingham B4 6NQ Telex 337321 MEMBERS OF THE POLICE AUTHORITY Chief Constable Deputy Chief Constable Sir Philip Knights CBE QPM Assistant Chief Constables Mr R Broome Chairman: Councillor E T Shore (Birmingham, Sattley) Administration and Supplies Crime Mr L Sharp LL.B Operations Mr D H Gerty LL.B. Mr K J Evans Vice-Chairman: Councillor T J Savage (Birmingham, Erdington) Organisation & Development Mr G E Coles B Jur Personnel & Training Staff Support Mr J B Glynn Mr T Meffen Local Authority Representatives Magistrate Criminal Investigation Department Members Chief Superintendent C W Powell (Operations) Chief Superintendent T Light (Support Services) Ward Chief Administrative Officer Councillor D M Ablett (Dudley, No.6) JD Baker Esq JP FCA ... Chief Superintendent PC J Price MA (Oxon) Councillor D Benny JP (Birmingham, Sandwell) K H Barker Esq Councillor E I Bentley (Meriden, No.1) OBE DL JP FRICS ..;. Personnel Department Councillor D Fysh (Wolverhampton No.4) Captain J E Heydon Chief Superintendent R P Snee Councillor J Hunte (Birmingham,Handsworth) ERD JP i Councillor K RIson (Stourbridge, No.1) J B Pendle Esq JP I. -

Birmingham City Council
BIRMINGHAM CITY COUNCIL REPORT OF THE ACTING SERVICE DIRECTOR REGULATION AND ENFORCEMENT TO THE LICENSING AND PUBLIC PROTECTION COMMITTEE 18 DECEMBER 2019 ALL WARDS PROSECUTIONS AND CAUTIONS – SEPTEMBER AND OCTOBER 2019 1. Summary 1.1 This report summarises the outcome of legal proceedings taken by Regulation and Enforcement during the months of September and October 2019. 2. Recommendation 2.1 That the report be noted. Contact Officer: Paul Lankester Interim Assistant Director, Regulation and Enforcement Telephone: 0121 675 2495 E-Mail: [email protected] 1 3. Results 3.1 During the months of September and October 2019 the following cases were heard at Birmingham Magistrates Court, unless otherwise stated: ▪ 141 Environmental Health cases were finalised resulting in fines of £210,795. Prosecution costs of £37,693 were awarded. Two simple cautions were administered as set out in Appendix 1. ▪ Ten Licensing cases were finalised resulting in fines of £3,859 and 42 penalty points issued. Prosecution costs of £4,009 were awarded. 15 simple cautions were administered as set out in Appendix 2. ▪ Four Trading Standards cases were finalised resulting in fines of £3,601, a 21 month custodial sentence and a five year disqualification from being a Director. Prosecution costs in the sum of £7,493 were awarded and an agreed POCA confiscation order was made in the sum of £36,493. One simple caution was administered as set out in Appendix 3. ▪ 15 Waste Enforcement cases were finalised resulting in fines of £78,980. Prosecution costs in the sum of £8,148 were awarded. No simple cautions were administered as set out in Appendix 4. -

Pharmacy Minor Ailment Scheme
The Pharmacy Minor Ailments Service covers the following conditions Minor Ailment/Condition Acute Cough under 16 and over 16 Acute Fever under 16 Acute Bacterial Conjunctivitis under 16 and over 16 Acute Pain / Earache/Headache/ Temperature over 16 Athletes Foot under 16 and over 16 Bites and Stings and Allergies under 16 and over 16 Cold sores under 16 and over 16 Cold and Flu under 16 and over 16 Constipation under 16 and over 16 Cystitis over 16 Diarrhoea under 16 and over 16 Dry Skin (Simple Eczema) under 16 Dermatitis/Allergic type rashes under 16 and over 16 Earache under 16 Earwax under 16 and over 16 Hay Fever under 16 and over 16 Heartburn/Indigestion over 16 Haemorrhoids over 16 Infant Decongestant under 16 Mouth Ulcers and Teething under 16 Mouth Ulcers over 16 Nappy Rash under 16 Oral Thrush under 16 and over 16 Scabies under 16 and over 16 Sore Throat over 16 Sprains and Strains over 16 Sunburn under 16 Threadworm under 16 and over 16 Vaginal Thrush over 16 Warts and Verruca’s under 16 Participating Pharmacies in the Sandwell and West Birmingham area: Pharmacy Name Pharmacy Address Postcode Al-Shafa Pharmacy 93 Shireland Road, Smethwick B66 4QJ Al-Shifa Pharmacy 164 Lozells Rd, Birmingham B19 2SX ASDA Pharmacy within ASDA store off Windmill Lane, Smethwick, Birmingham B66 3EN ASDA Pharmacy within ASDA store Old Park Lane, Oldbury, West Midlands B69 4PU ASDA Pharmacy within ASDA store One Stop Shopping Centre, Walsall Road, Perry Barr, Birmingham B42 1AB ASDA Pharmacy within ASDA Superstore Wednesbury Oak Road, Tipton DY4 -
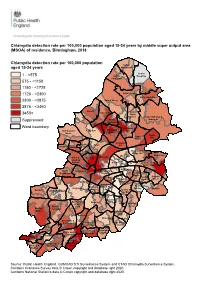
MSOA) of Residence, Birmingham, 2018
Chlamydia detection rate per 100,000 population aged 15-24 years by middle super output area (MSOA) of residence, Birmingham, 2018 Chlamydia detection rate per 100,000 population Sutton aged 15-24 years Mere Green Sutton 1 - <575 Sutton Roughley Four Oaks 575 - <1150 1150 - <1725 1725 - <2300 Sutton Trinity Sutton Reddicap 2300 - <2875 Sutton Vesey 2875 - <3450 Oscott Kingstanding Sutton 3450+ Wylde Green Sutton Walmley & Perry Minworth Suppressed Common Ward boundary Erdington Handsworth Perry Barr Stockland Wood Green Castle Pype Vale Hayes Gravelly Birchfield Aston Hill Holyhead Handsworth Lozells Bromford & Hodge Hill Ward End Shard End Soho & Newtown Nechells Jewellery Quarter Alum Rock Glebe Farm & Tile Cross Heartlands North Ladywood Bordesley & Edgbaston Highgate Yardley East Garretts Bordesley Yardley Green Green Small West & Heath Stechford Sparkbrook & South Balsall Balsall Heath Edgbaston Yardley Sheldon Heath East Tyseley & Quinton Harborne West Hay Mills Sparkhill Bournbrook Moseley & Selly Acocks Weoley & Park Green Bartley Selly Oak Green Hall Green North Stirchley Billesley Bournville & Cotteridge Brandwood & Hall Green King's Heath South Allens Cross Druids Heath Highter's King's Norton & Monyhull Heath North Frankley Northfield Great Park King's Longbridge & Norton Rubery & West Heath South Rednal Source: Public Health England, GUMCAD STI Surveillance System and CTAD Chlamydia Surveillance System. Contains Ordnance Survey data © Crown copyright and database right 2020. Contains National Statistics data © Crown copyright -

Commission on Gangs and Violence: Uniting to Improve Safety
Commission on Gangs and Violence: Uniting to improve safety November 2017 Rev Dr. Carver Anderson Contents Abbreviations 4 Letter to Commission 5 Acknowledgements 6 Foreword 9 Report Summary 11 1. Introduction 1.1 Background to Commission 23 1.2 Why another report? 24 1.3 Key factors explored 25 1.4 Intended outcomes 26 1.5 Report structure 27 2. Methodological considerations 2.1 Introduction 27 2.2 Mixed methods approach 28 2.3 Ethical and sensitivity issues 28 2.4 Field work 28 2.5 Time scales and analysis 31 3. The Birmingham context: understanding the issues and challenges 3.1 Introduction 33 3.2 Interpretations and perspectives regarding gangs and violence in 34 Birmingham –views from social research studies and reports 3.3 The current issues and challenges 38 3.4 Interventions and responses to gang-associated criminality and 47 violence 2 4. Community-led research: results, rationales and recommendations 4.1 Introduction 49 4.2 Criminal Justice and public health considerations 51 4.3 Gang labels – contested and reinforced 55 4.4 Community-involved and community-led partnerships 61 4.5 Individuals and families (‘street’ and ‘natural’) – support structures 64 and interventions 4.6 Education training and preventative considerations 68 4.7 The voices of young people (‘uninvolved’, ‘gang-associated’, 71 ‘victims’ and ‘perpetrators’) 4.8 Specialist providers and culturally competent grassroots 79 organisations 4.9 Faith groups – an untapped component 84 4.10 Prison influences 91 4.11 Statutory and business sector responses 94 5. Framework for building effective community-involved partnerships 5.1 Introduction 99 5.2 Trust, moral dilemmas and confidence factors 99 5.3 Leadership, ownership and sustainability 102 5.4 Conceptual framework: towards effective partnerships 104 6.