Final Project Report with Manual
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
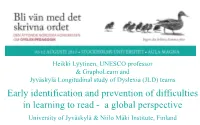
Early Identification and Prevention of Difficulties in Learning to Read - a Global Perspective University of Jyväskylä & Niilo Mäki Institute, Finland
Heikki Lyytinen, UNESCO professor & GraphoLearn and Jyväskylä Longitudinal study of Dyslexia (JLD) teams Early identification and prevention of difficulties in learning to read - a global perspective University of Jyväskylä & Niilo Mäki Institute, Finland .. or how I am trying to approach the goal of my present duty as UNESCO Chair/professor On Inclusive Literacy Learning for All For more, see …GraphoLearn.info and for our related publications, heikki.lyytinen.info Compromised reading skill Biological reasons (% of population) » Global > 5% » Finland > 3% (and other transparent languages) Educational reasons » Global - up to 90% (in developing some countries) » Finland – 0% » >500 million compromised readers! The development of reading accuracy (% correct) during the 1. Grade in Finland Procentage Procentage 36 100 36 100 80 of correct items 27 75 of correct 27 orrect 60 18 18 50 itmes 40 items36 from correct 9 9 25 20 Onumber Number items from 36 0 0 0 0 School +10 vk 1.Gr ends School +10 vk. 1.Gr entry +5 week +15 week entry ends +5 week +15 week Individual development The average development Aro et al., 2004 Early identification - Jyväskylä Longitudinal study of Dyslexia (JLD) & Graphogame – our tool for the prevention of RDs The Jyväskylä Longitudinal study of Dyslexia (JLD): An intensive follow-up of children at familial risk for dyslexia from birth > JLD 1994- Timo Ahonen, Mikko Aro, Kenneth Eklund, Jane Erskine, Tomi Guttorm, Leena Holopainen, Jarmo Hämäläinen, Ritva Ketonen, Marja-Leena Laakso, Seija Leinonen, Paavo Leppänen, -

Full Issue Vol. 2 No. 4
Swedish American Genealogist Volume 2 | Number 4 Article 1 12-1-1982 Full Issue Vol. 2 No. 4 Follow this and additional works at: https://digitalcommons.augustana.edu/swensonsag Part of the Genealogy Commons, and the Scandinavian Studies Commons Recommended Citation (1982) "Full Issue Vol. 2 No. 4," Swedish American Genealogist: Vol. 2 : No. 4 , Article 1. Available at: https://digitalcommons.augustana.edu/swensonsag/vol2/iss4/1 This Full Issue is brought to you for free and open access by Augustana Digital Commons. It has been accepted for inclusion in Swedish American Genealogist by an authorized editor of Augustana Digital Commons. For more information, please contact [email protected]. Swedish American Genea o ist A journal devoted to Swedish American biography, genealogy and personal history CONTENTS The Emigrant Register of Karlstad 145 Swedish American Directories 150 Norwegian Sailor Last Survivor 160 Norwegian and Swedish Local Histories 161 An Early Rockford Swede 171 Swedish American By-names 173 Literature 177 Ancestor Tables 180 Genealogical Queries 183 Index of Personal Names 187 Index of Place Names 205 Index of Ships' Names 212 Vol. II December 1982 No. 4 I . Swedish Americanij Genealogist ~ Copyright © I 982 S1tiedish Amerh·an Geneal,,gtst P. 0 . Box 2186 Winte r Park. FL 32790 !I SSN 0275-9314 ) Editor and P ub lisher Nils Will ia m Olsson. Ph.D .. F.A.S.G. Contributing Editors Glen E. Brolardcr. Augustana Coll ege . Rock Island. IL: Sten Carls,on. Ph.D .. Uppsala Uni versit y. Uppsala . Sweden: Carl-Erik Johans,on. Brigham Young Univ ersity.J>rovo. UT: He nn e Sol Ib e . -

Geology of the Northern Norrbotten Ore Province, Northern Sweden Paper 12 (13) Editor: Stefan Bergman
Rapporter och meddelanden 141 Geology of the Northern Norrbotten ore province, northern Sweden Paper 12 (13) Editor: Stefan Bergman Rapporter och meddelanden 141 Geology of the Northern Norrbotten ore province, northern Sweden Editor: Stefan Bergman Sveriges geologiska undersökning 2018 ISSN 0349-2176 ISBN 978-91-7403-393-9 Cover photos: Upper left: View of Torneälven, looking north from Sakkara vaara, northeast of Kiruna. Photographer: Stefan Bergman. Upper right: View (looking north-northwest) of the open pit at the Aitik Cu-Au-Ag mine, close to Gällivare. The Nautanen area is seen in the back- ground. Photographer: Edward Lynch. Lower left: Iron oxide-apatite mineralisation occurring close to the Malmberget Fe-mine. Photographer: Edward Lynch. Lower right: View towards the town of Kiruna and Mt. Luossavaara, standing on the footwall of the Kiruna apatite iron ore on Mt. Kiirunavaara, looking north. Photographer: Stefan Bergman. Head of department, Mineral Resources: Kaj Lax Editor: Stefan Bergman Layout: Tone Gellerstedt och Johan Sporrong, SGU Print: Elanders Sverige AB Geological Survey of Sweden Box 670, 751 28 Uppsala phone: 018-17 90 00 fax: 018-17 92 10 e-mail: [email protected] www.sgu.se Table of Contents Introduktion (in Swedish) .................................................................................................................................................. 6 Introduction .............................................................................................................................................................................. -

Data Retention in the EU
Evidence for necessity of data retention in the EU Table of Contents 1. Introduction ................................................................................................................................. 2 2. Context ........................................................................................................................................ 2 3. How communications data are used ............................................................................................ 3 4. Overview of types of cases in which data are important ............................................................. 4 5. Consequences of absence of data retention ................................................................................. 5 6. Cross-border aspects of data retention......................................................................................... 6 7. Statistics and quantitative data .................................................................................................... 7 Article 10 ......................................................................................................................................... 7 Available statistics ........................................................................................................................... 7 Limitations of quantitative data ....................................................................................................... 8 Conceptual and methodological issues ........................................................................................... -

Disposal of Plastic End-Of-Life-Boats
TemaNord 2013:582 TemaNord Ved Stranden 18 DK-1061 Copenhagen K www.norden.org Disposal of plastic end-of-life-boats Disposal of plastic end-of-life-boats Of Europe’s approximately 6 million boats almost half are found in the Nordic countries. In spite of the long durability of plastic boats, the problem of End of Life Boats (ELB) now starts to arise. However, the responsibilities are unclear and there is no regulation on how the dismantling and disposal is to be conducted. Investigations have been going on in the various Nordic countries on how to perform scrapping of plastic boats, but there is yet no consensus on how to handle the problem. The aim of this study was to provide information on statistics on boats in the Nordic countries and relate to the future need for scrapping plastic boats (ELB). More specific, the project dealt with the magnitude of dumping of boats, contents of contaminants in ELBs as well as possibilities for reuse and recycling of materials. Part of the project was to organize a Nordic Workshop with essential stakeholders and their views on ELB is compiled in this report. The project provides a good background to the problem of disposing of boats and highlights the various issues that must be addressed. Since the scrapping of boats is a future waste problem which need to be solved, this project is relevant to many different stakeholders from boaters, boat organizations, shipyards, waste companies and government institutions at various levels. TemaNord 2013:582 ISBN 978-92-893-2651-3 TN2013582 omslag.indd 1 15-10-2013 07:16:48 Disposal of plastic end-of-life-boats Britta Eklund, ITM Stockholm University, Sweden – project leader Hanna Haaksi, Keep the Archipelago Tidy, Finland Frode Syversen, Mepex Consult AS, Norway and Rasmus Eisted, Rambøll Danmark A/S, Denmark TemaNord 2013:582 Disposal of plastic end-of-life-boats Britta Eklund, ITM Stockholm University, Sweden – project leader. -

Gulo Gulo) Depredation Control in Västerbotten County
Faculty of Forest Sciences Analysis of the successfulness of wolverine (Gulo gulo) depredation control in Västerbotten County Fredrika Vretling Examensarbete i ämnet biologi Department of Wildlife, Fish, and Environmental studies Umeå 2016 Analysis of the successfulness of wolverine (Gulo gulo) depredation control in Västerbotten County Fredrika Vretling Supervisor: Göran Ericsson, Dept. of Wildlife, Fish, and Environmental Studies Assistant supervisor: Camilla Sandström, Umeå University, Linda Backlund and Michael Schneider, County Administrative Board Västerbotten Examiner: Fredrik Widemo, Dept. of Wildlife, Fish, and Environmental Studies Credits: 30 HEC Level: A2E Course title: Master degree thesis in Biology at the Department of Wildlife, Fish, and Environmental Studies Course code: EX0764 Programme/education: Jägmästarprogrammet Place of publication: Umeå Year of publication: 2016 Cover picture: - Title of series: Examensarbete i ämnet biologi Number of part of series: 2016:15 Online publication: http://stud.epsilon.slu.se Keywords: Wolverine, Gulo gulo, depredation control, quota harvest, hunting methods, semi- domesticated reindeer husbandry, qualitative interview Sveriges lantbruksuniversitet Swedish University of Agricultural Sciences Faculty of Forest Sciences Department of Wildlife, Fish, and Environmental Studies Abstract During the last five years, permitted quota of wolverine to be removed by depredation control have not been filled in the County of Västerbotten. Few hunting attempts have been successful. Because of this, issues regarding the depredation of reindeer may not be solved. The aim of this study was to evaluate the successfulness of hunting of wolverines for depredation control in Västerbotten County. Results from this study show that interviewees viewed depredation control as a positive management tool, but that possibilities for hunting were rather limited. -

Temporary Employment Agencies in the Nordic Countries
Temporary Employment Agencies in the Nordic Countries Ronnie Eklund The purpose of this article is to trace the origins and development of temporary manpower procurement policies in the Nordic countries.1 1 Legal Framework with Respect to Employment Exchange and Temporary Employment Agencies In the past, the Nordic provisions in force concerning promotion of employment entrusted the monopoly of employment procurement to public employment agencies. The origins of this phenomenon are international. Article 1 of the ILO Employment Service Convention No. 88/1948 sets the standard stipulating that the ratifying member “shall maintain or ensure the maintenance of a free public employment service”. All the four Nordic countries have ratified this Convention.2 When discussing the issue of temporary employment agencies, it must be borne in mind that public employment agencies, whose main task it is to channel job opportunities to job seekers, are bypassed in those segments of the labour market where temporary employment agencies or other persons act as intermediaries. Such activities frustrate the objectives of the state monopoly. The ILO Convention No. 96/1949 on Fee-Charging Employment Agencies (revising Convention No. 34/1933) either bans the activities of fee-charging employment agencies, which are conducted with a view to profit, or provides for 1 At the end of 1993 I presented before the Expert Committee of the Nordic Council a Report on the Hiring-out of Manpower in the Nordic Countries (In- och uthyrning av arbetskraft i de nordiska länderna September 1993, mimeographed). The term “Nordic countries” refers to: Denmark, Finland, Norway and Sweden. Iceland was not included. -

Temporary Employment Agencies in the Nordic Countries
Temporary Employment Agencies in the Nordic Countries Ronnie Eklund The purpose of this article is to trace the origins and development of temporary manpower procurement policies in the Nordic countries. 1 1 Legal Framework with Respect to Employment Exchange and Temporary Employment Agencies In the past, the Nordic provisions in force concerning promotion of employment entrusted the monopoly of employment procurement to public employment agencies. The origins of this phenomenon are international. Article 1 of the ILO Employment Service Convention No. 88/1948 sets the standard stipulating that the ratifying member “shall maintain or ensure the maintenance of a free public employment service”. All the four Nordic countries have ratified this Convention. 2 When discussing the issue of temporary employment agencies, it must be borne in mind that public employment agencies, whose main task it is to channel job opportunities to job seekers, are bypassed in those segments of the labour market where temporary employment agencies or other persons act as intermediaries. Such activities frustrate the objectives of the state monopoly. The ILO Convention No. 96/1949 on Fee-Charging Employment Agencies (revising Convention No. 34/1933) either bans the activities of fee-charging employment agencies, which are conducted with a view to profit, or provides for 1 At the end of 1993 I presented before the Expert Committee of the Nordic Council a Report on the Hiring-out of Manpower in the Nordic Countries ( In- och uthyrning av arbetskraft i de nordiska länderna September 1993, mimeographed). The term “Nordic countries” refers to: Denmark, Finland, Norway and Sweden. Iceland was not included. -

Vol23-No3-Final-Web
The Quarterly Vol. 23, No. 3 Fall 2015 The Swedish Finn Historical Society — http://finlander.genealogia.fi/sfhswiki/index.php Svenska Dagen 2015 at the Swedish Club By Rikki Nyman Friday, November 6, 2015, the Swedish Culture Center and the Swedish Finn Historical Society had the pleasure of jointly hosting what may become an annual event in Seattle: Svenska Dagen. After a fine dinner of pork roast, meatballs, red cabbage, potatoes, and apple crisp, Kjell Herberts of the Institute of Migration and Åbo Academi University in Finland, gave an enlightening talk on the multilingualism of the current Finnish population specifi- cally in reference to the many changes in demographics over the last 100 years. Svenska Dagen, also referred to as Finnish Swedish Heritage Day, is celebrated in Finland by small events, especially in schools, throughout the country. It dates back to 1908 when Swedish-speaking Finns sought a means to strengthen their community. The economical Swedish-Finns tied the event into Gustav Adolphus Day in Sweden, which marked the death of the Swedish king when he was killed at the Battle of Lützen on November 6, 1632. Though the event originally focused on King Gustav Adolphus and Swedishness per se, over time the empha- sis shifted from Swedishness to embracing bilingualism throughout Finland and a deeper appreciation of the Kjell Herberts presenting at Svenska Dagen. cultural cross-pollination that has made Finland what it is today—a small, but strong and flexible culture notable continued p. 67 Contents Regular Content Feature Content Calendar—Fall 2015 63 Svenska Dagen 2015 61 From the President 64 Historial Significance of Svenska Dagen 68 From the Editor 65 Looking for Lutefisk 69 Recipes—Christmas Edition 82 Lidman Family in Petalax 70 Donations to the Archive 84 Sideby Shipbuilding Museum Turns 20 72 Member News 85 2015 Reunion of Swedish-speaking Cousins 74 Associated Organizations & Contacts 87 The Quarterly Vol. -
Innovation Capabilities, Design and Cutting Edge
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Osuva Carita Eklund Innovation Capabilities, Design and Cutting Edge Innovative Growth in the 21st Century aaa ACTA WASAENSIA 426 ACADEMIC DISSERTATION To be presented, with the permission of the Board of the School of Accounting and Finance of the University of Vaasa, for public examination in Auditorium Kurtén (C203) on the 30th of August, 2019, at noon. Reviewers Professor Tuomas Takalo Hanken School of Economics Department of Economics PL 479 FI-00101 Helsinki Finland Associate professor Ebbe Krogh Graversen Aarhus University Department of Political Science, Danish Centre for Studies in Research and Research Policy School Bartholins Allé 7 DK-8000 Aarhus C Denmark III Julkaisija Julkaisupäivämäärä Vaasan yliopisto Elokuu 2019 Tekijä(t) Julkaisun tyyppi Carita Eklund Esseeväitöskirja ORCID tunniste Julkaisusarjan nimi, osan numero orcid.org/0000-0002-4217-0927 Acta Wasaensia, 426 Yhteystiedot ISBN Vaasan yliopisto 978-952-476-872-6 (painettu) Rahoituksen ja laskentatoimen yksikkö 978-952-476-873-3 (verkkoaineisto) Taloustiede URN:ISBN:978-952-476-873-3 PL 700 ISSN FI-65101 VAASA 0355-2667 (Acta Wasaensia 426, painettu) 2323-9123 (Acta Wasaensia 426, verkkoaineisto) Sivumäärä Kieli 124 englanti Julkaisun nimike Innovaatiokyvykkyys, Muotoilu ja Suunnannäyttäjät - Innovatiivinen kasvu 2100- vuosisadalla Tiivistelmä Tässä väitöskirjassa tarkastellaan aineettoman pääoman ja muotoilu-osaamisen vaikutusta niin innovaatioihin kuin yrityksien tuottavuuteen ja yrityksen nopeaan kasvuun. Ensimmäinen essee tarkastelee kuinka muotoilu-osaaminen eri vaiheissa innovaatioprosessia vaikuttaa uusien tuotteiden kehittämiseen. Kirjallidessa on teoreettista keskustelua muotoilun ja muotoilu-osaamisen vaikutuksesta innovaatioihin mutta empiiristä tutkimusta on toistaiseksi vähän. Essee luo uuden konseptin, design- skaalan, jonka avulla designin suhdetta innovaatioihin tarkastellaan CIS-kyselyaineiston avulla. -

To SAG, Volume XXII (2002)
Swedish American Genealogist Volume 22 Number 4 Article 12 12-1-2002 Index to SAG, Volume XXII (2002) James E. Erickson Follow this and additional works at: https://digitalcommons.augustana.edu/swensonsag Part of the Genealogy Commons, and the Scandinavian Studies Commons Recommended Citation Erickson, James E. (2002) "Index to SAG, Volume XXII (2002)," Swedish American Genealogist: Vol. 22 : No. 4 , Article 12. Available at: https://digitalcommons.augustana.edu/swensonsag/vol22/iss4/12 This Article is brought to you for free and open access by the Swenson Swedish Immigration Research Center at Augustana Digital Commons. It has been accepted for inclusion in Swedish American Genealogist by an authorized editor of Augustana Digital Commons. For more information, please contact [email protected]. Index to SAG, Volume XXII (2002) James E. Erickson The Index to SAG, Volume XXII (2002) is divided into the following parts: • Index of Contents, pages 224-226 • Index of Personal Names, pages 227-237 • Index of Place Names, pages 238-246 • Index of Ship Names, page 246 oOo Index of Contents Footprints of Family by Larry Oakes 1 Anna Marta's Story by Emelia Thunander Nordling 21 My Search for Angermanland Ancestors in Sweden and America by Bruce William Anderson 25 Genealogical Workshop: Documents Carried by a Swedish Emigrant in 1920 by James E. Erickson 41 CD Reviews 50 Swedes in Canada : A Project to Research and Write a History of Swedes in Canada 53 Genealogical Queries 55 Index to SAG, Volume XXII(2002) 225 America in My Childhood by Ulf Beijbom 57 Vilhelm Moberg Relatives-Morbroder, Moster and Sy ster-in the United States by James E. -

Lithosphere 2012
INSTITUTE OF SEISMOLOGY UNIVERSITY OF HELSINKI REPORT S-56 LITHOSPHERE 2012 SEVENTH SYMPOSIUM ON THE STRUCTURE, COMPOSITION AND EVOLUTION OF THE LITHOSPHERE IN FINLAND PROGRAMME AND EXTENDED ABSTRACTS edited by Ilmo Kukkonen, Emilia Kosonen, Kati Oinonen, Olav Eklund, Annakaisa Korja, Toivo Korja, Raimo Lahtinen, Juha Pekka Lunkka and Markku Poutanen Geological Survey of Finland Espoo, November 6-8, 2012 Helsinki 2012 ii Editor-in-Chief: Pekka Heikkinen Guest Editors: Ilmo Kukkonen, Emilia Kosonen, Kati Oinonen, Olav Eklund, Annakaisa Korja, Toivo Korja, Raimo Lahtinen, Juha Pekka Lunkka and Markku Poutanen Publisher: Institute of Seismology P.O. Box 68 FI-00014 University of Helsinki Finland Phone: +358-9-1911 (swichboard) Fax: +358-9-191 51698 http://www.helsinki.fi/geo/seismo/ ISSN 0357-3060 ISBN 978-952-10-5066-4 (Paperback) Helsinki University Print Helsinki 2012 ISBN 978-952-10-5067-1 (PDF) iii LITHOSPHERE 2012 SEVENTH SYMPOSIUM ON THE STRUCTURE, COMPOSITION AND EVOLUTION OF THE LITHOSPHERE IN FINLAND PROGRAMME AND EXTENDED ABSTRACTS Geological Survey of Finland, Espoo, November 6-8, 2012 CONTRIBUTING ORGANIZATIONS Finnish National Committee of the International Lithosphere Programme (ILP) Finnish Geodetic Institute Geological Survey of Finland University of Helsinki University of Oulu Åbo Akademi University ORGANIZING COMMITTEE AND EDITORS Ilmo Kukkonen Geological Survey of Finland P.O. B. 96, FI-02151 Espoo, Finland E-mail: ilmo.kukkonen [at] gtk.fi Olav Eklund Geology and mineralogy, Åbo Akademi University Domkyrkotorget 1, FI-20500 Åbo/Turku, Finland E-mail: olav.eklund [at] abo.fi Annakaisa Korja Institute of Seismology, Dept. of Geosciences and Geography P.O.B. 68, FI-00014 University of Helsinki, Finland E-mail: annakaisa.korja [at] helsinki.fi Toivo Korja Department of Physics, University of Oulu P.O.B 3000, FI-90014 University of Oulu, Finland E-mail: toivo.korja [at] oulu.fi Emilia Kosonen Institute of Seismology, Dept.