Clinical Practice Guidelines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hydronephrosis
Hydronephrosis Natasha Brownrigg RN(EC), MN, NP-Pediatrics Assistant Clinical Professor, McMaster School of Nursing Nurse Practitioner, Pediatric Urology, McMaster Children’s Hospital, Hamilton, ON, Canada Dr. Jorge DeMaria Pediatric Urologist, McMaster Children’s Hospital Professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada Dr. Luis H.P. Braga Pediatric Urologist, McMaster Children’s Hospital. Associate professor Department of Surgery/Urology, McMaster University, Hamilton, ON, Canada What is hydronephrosis? Hydro Nephrosis Hydronephrosis += Refers to water Refers to the kidney A build up of fluid or fluid (urine) in the kidney Hydronephrosis is the medical term for a build-up of urine in the kidney. As the urine builds up, it stretches or dilates the inside of the kidney, known as the collecting system. If an unborn baby has hydronephrosis, an ultrasound scan will show a build-up of urine in the kidney. This is called “antenatal hydronephrosis.” Hydronephrosis is found in as many as five out of 100 pregnancies. Hydronephrosis may also be found after birth. For example, if a baby has a urinary tract infection, an ultrasound of the baby’s kidneys and bladder may detect hydronephrosis. Key points to remember if your baby has hydronephrosis • Your baby can grow and develop normally with hydronephrosis. • Hydronephrosis may affect one kidney or both. • Hydronephrosis is a finding, not a disease. • Further tests are needed to find the cause of hydronephrosis. • If the cause is known, a pediatric urologist will discuss the possible treatment. Surgery is sometimes required to correct the cause of the hydronephrosis. Hydronephrosis is often transient and improves without any intervention. -

Leading Article the Molecular and Genetic Base of Congenital Transport
Gut 2000;46:585–587 585 Gut: first published as 10.1136/gut.46.5.585 on 1 May 2000. Downloaded from Leading article The molecular and genetic base of congenital transport defects In the past 10 years, several monogenetic abnormalities Given the size of SGLT1 mRNA (2.3 kb), the gene is large, have been identified in families with congenital intestinal with 15 exons, and the introns range between 3 and 2.2 kb. transport defects. Wright and colleagues12 described the A single base change was identified in the entire coding first, which concerns congenital glucose and galactose region of one child, a finding that was confirmed in the malabsorption. Subsequently, altered genes were identified other aZicted sister. This was a homozygous guanine to in partial or total loss of nutrient absorption, including adenine base change at position 92. The patient’s parents cystinuria, lysinuric protein intolerance, Menkes’ disease were heterozygotes for this mutation. In addition, it was (copper malabsorption), bile salt malabsorption, certain found that the 92 mutation was associated with inhibition forms of lipid malabsorption, and congenital chloride diar- of sugar transport by the protein. Since the first familial rhoea. Altered genes may also result in decreased secretion study, genomic DNA has been screened in 31 symptomatic (for chloride in cystic fibrosis) or increased absorption (for GGM patients in 27 kindred from diVerent parts of the sodium in Liddle’s syndrome or copper in Wilson’s world. In all 33 cases the mutation produced truncated or disease)—for general review see Scriver and colleagues,3 mutant proteins. -

Acute Kidney Injury: Challenges and Opportunities
Acute kidney injury: Challenges and opportunities Abstract: Community-acquired acute kidney injury (CA-AKI) can be a devastating diagnosis for any patient and can increase mortality during hospitalization. There can be long-term consequences for those who survive the initial insult. This article discusses CA-AKI and its implications for APRNs. By Nhan L.A. Dinh, MSN, CNP, AGACNP-BC, CCRN cute kidney injury (AKI) is a heterogeneous risk of CKD, but if clinicians do not recognize the kidney disorder that increases in-hospital diagnosis, they cannot follow up or intervene. An AKI A morbidity and mortality. In 2016 data, the diagnosis also increases the chance of another AKI incidence of AKI was 20% for Medicare patients with episode, with a 30% risk of a recurrent AKI episode both chronic kidney disease (CKD) and diabetes.1 Us- within 1 year.1 ing Veterans Affairs (VA) 2016 data, AKI occurred in Mortality is increased with an AKI episode. Medi- more than 25% of hospitalized veterans over age 22, care data from 2016 shows an in-hospital mortality of but less than 50% of those with lab-documented AKI 8.2% but this increases to over 13% when includ- were coded as such.1 The chief concern here is a missed ing patients who were discharged to hospice.1 The in- opportunity for intervention. AKI increases long-term hospital mortality for patients without AKI was only Keywords: acute kidney injury (AKI), Acute Kidney Injury Network (AKIN), chronic kidney disease (CKD), community-acquired acute kidney injury (CA-AKI), hospital-acquired acute kidney injury (HA-AKI), Kidney Disease Improving Global Outcomes (KDIGO), SvetaZi / Shutterstock Nephrotoxic Injury Negated by Just-in-time Action (NINJA), sick day rules 48 The Nurse Practitioner • Vol. -
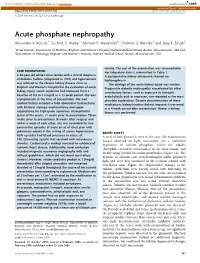
Acute Phosphate Nephropathy Alexander K
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector http://www.kidney-international.org the renal consult & 2009 International Society of Nephrology Acute phosphate nephropathy Alexander K. Rocuts1, Sushrut S. Waikar1, Mariam P. Alexander1,2, Helmut G. Rennke2 and Ajay K. Singh1 1Renal Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA and 2Department of Pathology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA minute. The rest of the examination was unremarkable. CASE PRESENTATION HerlaboratorydataissummarizedinTable1. A 60-year-old white Latino female with a clinical diagnosis A postoperative kidney ultrasound showed no of diabetes mellitus (diagnosed in 1993) and hypertension hydronephrosis. was referred to the chronic kidney disease clinic at The etiology of the acute kidney injury was unclear. Brigham and Women’s Hospital for the evaluation of acute Progressive diabetic nephropathy exacerbated by other kidney injury; serum creatinine had increased from a contributory factors, such as exposure to lisinopril, baseline of 0.9 to 1.5 mg/dl in a 11-week period. She was acetylsalicylic acid, or naproxen, was regarded as the most asymptomatic at the time of presentation. Her past plausible explanation. Despite discontinuation of these medical history included a total abdominal hysterectomy medications, kidney function did not improve; it worsened with bilateral salpingo oophorectomy and upper in a 4-week period after presentation. Hence, a kidney vaginectomy for high-grade squamous intraepithelial biopsy was performed. lesion of the cervix, 11 weeks prior to presentation. Three weeks prior to presentation (8 weeks after surgery) and within a week of each other, she was evaluated for two consecutive episodes of acute onset of chest pain with pulmonary edema in the setting of severe hypertension. -

A Case of Calciphylaxis with an Unfavorable Outcome
CASE LETTER 671 However, the present patient exhibited the peculiarity References of an intense inflammatory infiltrate in the dermis rarely seen previously. According to this case, an atypical intense 1. Sitaru C, Zillikens D. Mechanisms of blister induction by autoan- inflammation could be a distinct histopathological feature tibodies. Exp Dermatol. 2005;14:861---75. of trauma-induced pemphigus. Further research is neces- 2. Sagi L, Trau H. The Koebner phenomenon. Clin Dermatol. sary to ascertain if greater inflammation in dermis is more 2011;29:231---6. related to trauma-induced pemphigus as opposed to those 3. Jang HW, Chun SH, Lee JM, Jeon J, Hashimoto T, Kim IH. Radiotherapy-induced pemphigus vulgaris. J Dermatol. not related to trauma. 2014;41:851---2. In conclusion, this report describes a presumably new 4. Daneshpazhooh M, Fatehnejad M, Rahbar Z, Balighi K, case of trauma-induced pemphigus. To the author’s knowl- Ghandi N, Ghiasi M, et al. Trauma-induced pemphigus: a edge, there are no prior reports of pemphigus involving case series of 36 patients. J Dtsch Dermatol Ges. 2016;14: predominantly the breasts with such a peculiar dispo- 166---71. sition. It is proposed that a hypothetical continuous 5. Balighi K, Daneshpazhooh M, Azizpour A, Lajevardi V, trauma with the bra could explain this unique loca- Mohammadi F, Chams-Davatchi C. Koebner phenomenon tion. in pemphigus vulgaris patients. JAAD Case Rep. 2016;2: 419---21. Financial support Fernando Garcia-Souto None declared. Department of Dermatology, Valme University Hospital, Seville, Spain Author’s contributions E-mail: [email protected] Received 14 November 2019; accepted 5 March 2020 Fernando Garcia-Souto: Conception and planning of the manuscript; writing and critical revision of the manuscript; https://doi.org/10.1016/j.abd.2020.03.010 approval of the final version. -

Annotations Prognosis for Vesicoureteric Reflux
Arch Dis Child 1999;81:287–294 287 Arch Dis Child: first published as 10.1136/adc.81.4.287 on 1 October 1999. Downloaded from The Journal of the Royal College of Paediatrics and Child Health Annotations Prognosis for vesicoureteric reflux The prevalence of vesicoureteric reflux (VUR) has been to disentangle in this group of patients. The development estimated to be 2% of the child population.1 In children with of proteinuria is indicative of progressive glomerulosclero- VUR demonstrated on micturating cystourethrography sis and is a bad prognostic feature particularly when the there is a tendency for the grade of VUR to improve or for patient also has hypertension. VUR to disappear with time and with increasing age.23VUR has been identified as a risk factor for the development of Historical perspective urinary tract infections (UTI) and is present in a third of A review of literature in the preantibiotic era suggests that young children presenting with this problem. In addition, it chronic pyelonephritis was a very serious condition in chil- is a risk factor for renal scarring, otherwise called reflux dren and adults. Weiss and Parker described a series of nephropathy.45 VUR is also associated with renal dysplasia postmortem cases16: antecedent clinical features included and other developmental abnormalities of the urinary tract.6 recurrent fevers, presumably due to persistent untreated There is now abundant evidence for inheritance by an auto- infection, anaemia, hypertension, growth failure, and preg- somal dominant mechanism.7 nancy complications. There is evidence for a falling preva- lence of this condition, which is probably due to a true reduction of reflux nephropathy because of modern medi- Pathogenesis of reflux nephropathy cal care, particularly the treatment of acute pyelonephritis Studies have suggested that reflux nephropathy develops with antibiotics; alternatively the decline may represent following UTI in very early childhood or infancy.8 New changing fashions in disease classification. -

Glomerulosclerosis in Reflux Nephropathy
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Kidney International, Vol. 21(1982), pp. 528—534 NEPHROLOGY FORUM Glomeruloscierosis in reflux nephropathy Principal discussant: RAMzI S. COTRAN Department of Pathology, Brigham and Women's Hospital, Boston, Massachusetts penis, testes, and urethral meatus were normal. The prostate was of normal size. Editors The BUN was 14 mg/dl; creatinine, 1.3 mg/dl (creatinine clearance, 113 mI/mm); blood chemistries were normal; the blood glucose was 93 JORDANJ. COHEN mg/dl; and the complement profile was normal. Serum protein was 7.5 JOHN 1. HARRINGTON gIdI with 4.3 g/dl albumin. Urinalysis showed a pH of 5; a specific JEROME P.KASSIRER gravity of 1.015; 4+ protein, no cells, and no bacteria. Urine culture was sterile. The 24-hour urine protein excretion was 2.4 g. Editor Chest x-ray showed borderline cardiomegaly with clear lungs. An Managing intravenous pyelogram revealed bilateral coarse scarring with caliecta- CHERYL J. ZUSMAN sis. The right kidney was smaller than the left. There was moderate ureterectasia extending down to the ureterovesical junction. A voiding cystourethrogram revealed a large-capacity bladder; the patient had no MichaelReese Hospital and Medical Center urge to void after almost 500 ml of contrast material was instilled. Bilateral reflux was greater and persistent on the left and was intermit- University of Chicago, tent on the right. The left ureter was dilated and tortuous. A left Pritzker School of Medicine ureterocele and right bladder diverticulum were visualized. and A biopsy of the left kidney showed focal scarring with interstitial New England Medical Center fibrosis and chronic inflammation, tubular atrophy, and dilation. -

Assessment Report
17 September 2020 EMA/522604/2020 Corr.1 Committee for Medicinal Products for Human Use (CHMP) Assessment report Velphoro Common name: sucroferric oxyhydroxide Procedure No. EMEA/H/C/002705/X/0020/G Note Assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us An agency of the European Union Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 © European Medicines Agency, 2021. Reproduction is authorised provided the source is acknowledged. Table of contents 1. Background information on the procedure .............................................. 6 1.1. Submission of the dossier ...................................................................................... 6 1.2. Steps taken for the assessment of the product ......................................................... 7 2. Scientific discussion ................................................................................ 8 2.1. Problem statement ............................................................................................... 8 2.1.1. Disease or condition ........................................................................................... 8 2.1.2. Epidemiology and risk factors, screening tools/prevention ...................................... 8 2.1.3. Biologic features ............................................................................................... -
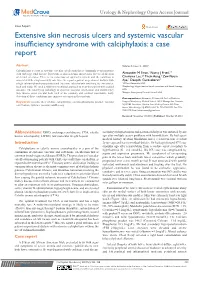
Extensive Skin Necrosis Ulcers and Systemic Vascular Insufficiency Syndrome with Calciphylaxis: a Case Report
Urology & Nephrology Open Access Journal Case Report Open Access Extensive skin necrosis ulcers and systemic vascular insufficiency syndrome with calciphylaxis: a case report Abstract Volume 5 Issue 4 - 2017 Calciphylaxis is a part of systemic vascular calcification that is commonly seen in patients 1 2,3 with end stage renal disease. It presents as skin ischemia and necrosis due to calcification Alexander M Swan, Nancy J Fried, 2,3 2 of dermal arterioles. There is no consensus on optimal treatment and the condition is Charisma Lee, Thein Aung, Zaw Nyein associated with a high mortality rate. Here we report a patient on peritoneal dialysis with Aye,2 Deepthi Gunasekaran2 a high calcium-phosphorus product and extensive calciphylaxis involving the extremities, 1Wilkes University, USA back and scalp. We used a multi-interventional approach to treat this patient with a good 2Nephrology Hypertension Renal transplant and Renal Therapy, outcome. The underlying pathology of systemic vascular calcification and insufficiency USA 3 may involve other vascular beds such as the coronary and cerebral vasculature. Early Rutgers New Jersey Medical School, USA detection of these conditions may improve outcomes in these patents. Correspondence: Alexander M Swan, AA Prof of Medicine, Keywords: necrotic ulcer of skin, calciphylaxis, calcium-phosphorus product, vascular Rutgers New Jersey Medical School, 185 S Orange Ave, Newark, calcification, systemic vascular insufficiency NJ 07103, President, Garden State Kidney Center, 345 Main Street, Woodbridge, NJ 07095, USA, Tel 732-750-5555, Fax 732- 750-5550, Email Received: November 10, 2017 | Published: October 26, 2017 Abbreviations: ESRD, end-stage renal disease; CUA, calcific secondary to hypertension and peritoneal dialys is was initiated 5years uremic arterilopathy; LMWH, low molecular weight heparin ago after multiple access problems with hemodialysis. -

Inherited Renal Tubulopathies—Challenges and Controversies
G C A T T A C G G C A T genes Review Inherited Renal Tubulopathies—Challenges and Controversies Daniela Iancu 1,* and Emma Ashton 2 1 UCL-Centre for Nephrology, Royal Free Campus, University College London, Rowland Hill Street, London NW3 2PF, UK 2 Rare & Inherited Disease Laboratory, London North Genomic Laboratory Hub, Great Ormond Street Hospital for Children National Health Service Foundation Trust, Levels 4-6 Barclay House 37, Queen Square, London WC1N 3BH, UK; [email protected] * Correspondence: [email protected]; Tel.: +44-2381204172; Fax: +44-020-74726476 Received: 11 February 2020; Accepted: 29 February 2020; Published: 5 March 2020 Abstract: Electrolyte homeostasis is maintained by the kidney through a complex transport function mostly performed by specialized proteins distributed along the renal tubules. Pathogenic variants in the genes encoding these proteins impair this function and have consequences on the whole organism. Establishing a genetic diagnosis in patients with renal tubular dysfunction is a challenging task given the genetic and phenotypic heterogeneity, functional characteristics of the genes involved and the number of yet unknown causes. Part of these difficulties can be overcome by gathering large patient cohorts and applying high-throughput sequencing techniques combined with experimental work to prove functional impact. This approach has led to the identification of a number of genes but also generated controversies about proper interpretation of variants. In this article, we will highlight these challenges and controversies. Keywords: inherited tubulopathies; next generation sequencing; genetic heterogeneity; variant classification. 1. Introduction Mutations in genes that encode transporter proteins in the renal tubule alter kidney capacity to maintain homeostasis and cause diseases recognized under the generic name of inherited tubulopathies. -

Hypertensive Kidney Disease Hypertensive Kidney
JAMA PATIENT PAGE The Journal of the American Medical Association KIDNEY DISEASE Hypertensive Kidney Disease ypertension (high blood pressure) causes problems for many organs in the body, including the kidneys. Kidney problems Hcaused by high blood pressure (hypertensive kidney disease) occur often in persons who have undetected, untreated, or poorly controlled hypertension. Kidney problems are also called renal dysfunction or renal failure. Certain groups of people, including African Americans and Native Americans, are more at risk for having hypertensive kidney disease. High blood pressure is the second leading cause of kidney failure, surpassed only by diabetes. African Americans are 6 times more likely than whites to have chronic renal failure related to high blood pressure. The November 20, 2002, issue of JAMA includes an article about high blood pressure and its effect on the kidneys. WHY IS HIGH BLOOD PRESSURE DANGEROUS? FOR MORE INFORMATION High blood pressure makes the heart work harder and can also damage the small blood • American Heart Association vessels in the body. These vessels are in all organs of the body, including the kidneys, the 800/242-8721 heart, and the brain. Damage to the arteries (blood vessels that carry blood to organs) www.americanheart.org results in insufficient blood flow to those organs and organ damage. In the kidney, this • National Institute of Diabetes & organ damage is called nephrosclerosis. The kidneys lose their ability to filter blood, Digestive & Kidney Diseases allowing buildup of substances that can be toxic to the body. Eventually the kidneys fail, www.niddk.nih.gov/health/kidney and dialysis (filtration of blood by a special machine) or a kidney transplant becomes /pubs/highblood/highblood.htm necessary to preserve the person’s life. -

AACE Annual Meeting 2021 Abstracts Editorial Board
June 2021 Volume 27, Number 6S AACE Annual Meeting 2021 Abstracts Editorial board Editor-in-Chief Pauline M. Camacho, MD, FACE Suleiman Mustafa-Kutana, BSC, MB, CHB, MSC Maywood, Illinois, United States Boston, Massachusetts, United States Vin Tangpricha, MD, PhD, FACE Atlanta, Georgia, United States Andrea Coviello, MD, MSE, MMCi Karel Pacak, MD, PhD, DSc Durham, North Carolina, United States Bethesda, Maryland, United States Associate Editors Natalie E. Cusano, MD, MS Amanda Powell, MD Maria Papaleontiou, MD New York, New York, United States Boston, Massachusetts, United States Ann Arbor, Michigan, United States Tobias Else, MD Gregory Randolph, MD Melissa Putman, MD Ann Arbor, Michigan, United States Boston, Massachusetts, United States Boston, Massachusetts, United States Vahab Fatourechi, MD Daniel J. Rubin, MD, MSc Harold Rosen, MD Rochester, Minnesota, United States Philadelphia, Pennsylvania, United States Boston, Massachusetts, United States Ruth Freeman, MD Joshua D. Safer, MD Nicholas Tritos, MD, DS, FACP, FACE New York, New York, United States New York, New York, United States Boston, Massachusetts, United States Rajesh K. Garg, MD Pankaj Shah, MD Boston, Massachusetts, United States Staff Rochester, Minnesota, United States Eliza B. Geer, MD Joseph L. Shaker, MD Paul A. Markowski New York, New York, United States Milwaukee, Wisconsin, United States CEO Roma Gianchandani, MD Lance Sloan, MD, MS Elizabeth Lepkowski Ann Arbor, Michigan, United States Lufkin, Texas, United States Chief Learning Officer Martin M. Grajower, MD, FACP, FACE Takara L. Stanley, MD Lori Clawges The Bronx, New York, United States Boston, Massachusetts, United States Senior Managing Editor Allen S. Ho, MD Devin Steenkamp, MD Corrie Williams Los Angeles, California, United States Boston, Massachusetts, United States Peer Review Manager Michael F.