Foundation Concepts of Health Management Information Systems
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Artificial Intelligence in Health Care: the Hope, the Hype, the Promise, the Peril
Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril Michael Matheny, Sonoo Thadaney Israni, Mahnoor Ahmed, and Danielle Whicher, Editors WASHINGTON, DC NAM.EDU PREPUBLICATION COPY - Uncorrected Proofs NATIONAL ACADEMY OF MEDICINE • 500 Fifth Street, NW • WASHINGTON, DC 20001 NOTICE: This publication has undergone peer review according to procedures established by the National Academy of Medicine (NAM). Publication by the NAM worthy of public attention, but does not constitute endorsement of conclusions and recommendationssignifies that it is the by productthe NAM. of The a carefully views presented considered in processthis publication and is a contributionare those of individual contributors and do not represent formal consensus positions of the authors’ organizations; the NAM; or the National Academies of Sciences, Engineering, and Medicine. Library of Congress Cataloging-in-Publication Data to Come Copyright 2019 by the National Academy of Sciences. All rights reserved. Printed in the United States of America. Suggested citation: Matheny, M., S. Thadaney Israni, M. Ahmed, and D. Whicher, Editors. 2019. Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. NAM Special Publication. Washington, DC: National Academy of Medicine. PREPUBLICATION COPY - Uncorrected Proofs “Knowing is not enough; we must apply. Willing is not enough; we must do.” --GOETHE PREPUBLICATION COPY - Uncorrected Proofs ABOUT THE NATIONAL ACADEMY OF MEDICINE The National Academy of Medicine is one of three Academies constituting the Nation- al Academies of Sciences, Engineering, and Medicine (the National Academies). The Na- tional Academies provide independent, objective analysis and advice to the nation and conduct other activities to solve complex problems and inform public policy decisions. -

Annual Report 2018–2019 Our Vision
ANNUAL REPORT 2018–2019 OUR VISION We shape tomorrow. We confront problems and create solutions. We expand information’s impact and technology’s potential. Together, our faculty, staff, students, and alumni make the world a better place—day by day, project by project, leap by leap. LEADERSHIP Raj Acharya Since its establishment in 2000, the Luddy School of Informatics, Computing, and Dean Engineering has built a reputation as one of the broadest of its kind. Our more than 3,000 students come from Indiana and around the world, and our unique blend Mathew Palakal of programs in informatics, computer science, intelligent systems engineering, Senior Executive Associate information and library science, data science, and more create an interdisciplinary, Dean collaborative environment where ideas thrive. Erik Stolterman Bergqvist Our forward-looking school is a mélange, a salad bowl of disparate but related Senior Executive Associate disciplines. That salad bowl provides us with a holistic taste of creativity and Dean innovation while preserving and enhancing the taste of the individual components. Esfandiar Haghverdi As we have grown exponentially through our first two decades, we have maintained Executive Associate Dean for our core values with an open-minded view of tomorrow, one that has allowed us to Undergraduate Education stay on the cutting edge of technology while anticipating what the future holds. David Leake We accomplished much during the 2018-19 school year. Our information and library Executive Associate Dean science program was ranked second in the world behind only Harvard by the 2018 Academic Ranking of World Universities. Researchers at our school garnered Kay Connelly $16.1 million in grants from the National Science Foundation, the National Institute Associate Dean for Research of Health, the National Cancer Institute, the Department of Defense, and other prestigious organizations, and our school ranks 12th in computer and information Karl F. -
Applications of Digital Image Processing in Real Time World
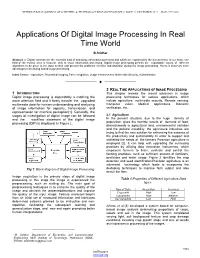
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VOLUME 8, ISSUE 12, DECEMBER 2019 ISSN 2277-8616 Applications Of Digital Image Processing In Real Time World B.Sridhar Abstract :-- Digital contents are the essential kind of analyzing, information perceived and which are explained by the human brain. In our brain, one third of the cortical area is focused only to visual information processing. Digital image processing permits the expandable values of different algorithms to be given to the input section and prevent the problems of noise and distortion during the image processing. Hence it deserves more advantages than analog based image processing. Index Terms:-- Agriculture, Biomedical imaging, Face recognition, image enhancement, Multimedia Security, Authentication —————————— —————————— 2 REAL TIME APPLICATIONS OF IMAGE PROCESSING 1 INTRODUCTION This chapter reviews the recent advances in image Digital image processing is dependably a catching the processing techniques for various applications, which more attention field and it freely transfer the upgraded include agriculture, multimedia security, Remote sensing, multimedia data for human understanding and analyzing Computer vision, Medical applications, Biometric of image information for capacity, transmission, and verification, etc,. representation for machine perception[1]. Generally, the stages of investigation of digital image can be followed 2.1 Agriculture and the workflow statement of the digital image In the present situation, due to the huge density of population, gives the horrible results of demand of food, processing (DIP) is displayed in Figure 1. diminishments in agricultural land, environmental variation and the political instability, the agriculture industries are trying to find the new solution for enhancing the essence of the productivity and sustainability.―In order to support and satifisfied the needs of the farmers Precision agriculture is employed [2]. -
Health Informatics Principles
Health Informatics Principles Foundational Curriculum: Cluster 4: Informatics Module 7: The Informatics Process and Principles of Health Informatics Unit 2: Health Informatics Principles FC-C4M7U2 Curriculum Developers: Angelique Blake, Rachelle Blake, Pauliina Hulkkonen, Sonja Huotari, Milla Jauhiainen, Johanna Tolonen, and Alpo Vӓrri This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and 21/60 innovation programme under Grant Agreement No. 727552 1 EUUSEHEALTHWORK Unit Objectives • Describe the evolution of informatics • Explain the benefits and challenges of informatics • Differentiate between information technology and informatics • Identify the three dimensions of health informatics • State the main principles of health informatics in each dimension This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and FC-C4M7U2 innovation programme under Grant Agreement No. 727552 2 EUUSEHEALTHWORK The Evolution of Health Informatics (1940s-1950s) • In 1940, the first modern computer was built called the ENIAC. It was 24.5 metric tonnes (27 tons) in volume and took up 63 m2 (680 sq. ft.) of space • In 1950 health informatics began to take off with the rise of computers and microchips. The earliest use was in dental projects during late 50s in the US. • Worldwide use of computer technology in healthcare began in the early 1950s with the rise of mainframe computers This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and FC-C4M7U2 innovation programme under Grant Agreement No. -

Draft Common Framework for Earth-Observation Data
THE U.S. GROUP ON EARTH OBSERVATIONS DRAFT COMMON FRAMEWORK FOR EARTH-OBSERVATION DATA Table of Contents Background ..................................................................................................................................... 2 Purpose of the Common Framework ........................................................................................... 2 Target User of the Common Framework ................................................................................. 4 Scope of the Common Framework........................................................................................... 5 Structure of the Common Framework ...................................................................................... 6 Data Search and Discovery Services .............................................................................................. 7 Introduction ................................................................................................................................. 7 Standards and Protocols............................................................................................................... 8 Methods and Practices ............................................................................................................... 10 Implementations ........................................................................................................................ 11 Software ................................................................................................................................ -

14 School Subject Informatics (Computer Science) in Russia: Educational Relevant Areas
i i i i School Subject Informatics (Computer Science) in Russia: Educational Relevant Areas EVGENIY KHENNER and IGOR SEMAKIN, Perm State National Research University, Russia This article deals with some aspects of studying Informatics in Russian schools. Those aspects are part of the ‘third dimension’ of the Darmstadt model (they are also projected on the other two dimensions of this model) and include evolution of the subject, regulatory norms conforming to the Federal Educational Standards, the learning objectives, the required learning outcomes, and the Unified National Examination in Informatics, which is required for admission to a number of university programs. It is interesting to note that correspondence between requirements for the outcomes of learning Informatics in Russian school and the requirements of K-12 Computer Science Standards (USA) is quite satisfactory. It is noteworthy that the relatively high level of school education in Informatics in Russia is determined by the well-established methodological system with a 30-year history, the subject’s being on the list of core disciplines at school, as well as the existence of a state-sponsored system of education teachers of Informatics. Categories and Subject Descriptors: K.3.2 [Computers and Education]: Computer and Information Science Education—Computer science education General Terms: Algorithms, Languages, Security Additional Key Words and Phrases: History of Informatics in school, education policies, educational standards, qualification and professional experience of teachers, learning objectives and outcomes, structural components of Informatics, curriculum issues, Unified National Exam, extracurricular activities, textbooks, didactic software ACM Reference Format: Khenner, E. and Semakin, I. 2014. School subject informatics (computer science) in Russia: Educational relevant areas. -

Information- Processing Conceptualizations of Human Cognition: Past, Present, and Future
13 Information- Processing Conceptualizations of Human Cognition: Past, Present, and Future Elizabeth E Loftus and Jonathan w: Schooler Historically, scholars have used contemporary machines as models of the mind. Today, much of what we know about human cognition is guided by a three-stage computer model. Sensory memory is attributed with the qualities of a computer buffer store in which individual inputs are briefly maintained until a meaningful entry is recognized. Short-term memory is equivalent to the working memory of a computer, being highly flexible yet having only a limited capacity. Finally, long-term memory resembles the auxiliary store of a computer, with a virtually unlimited capacity for a variety of information. Although the computer analogy provides a useful framework for describing much of the present research on human cogni- tion, it is insufficient in several respects. For example, it does not ade- quately represent the distinction between conscious and non-conscious thought. As an alternative. a corporate metaphor of the mind is suggested as a possible vehiclefor guiding future research. Depicting the mind as a corporation accommodates many aspects of cognition including con- sciousness. In addition, by offering a more familiar framework, a corpo- rate model is easily applied to subjective psychological experience as well as other real world phenomena. Currently, the most influential approach in cognitive psychology is based on analogies derived from the digital computer. The information processing approach has been an important source of models and ideas but the fate of its predecessors should serve to keep us humble concerning its eventual success. In 30 years, the computer-based information processing approach that cur- rently reigns may seem as invalid to the humlln mind liSthe wax-tablet or tl'kphOlIl' switchhoard mmkls do todoy. -

B.A. in Computing and Informatics 856-256-4805
College of Science and Mathematics Contact Department of Computer Science Robinson Hall B.A. in Computing and Informatics 856-256-4805 www.rowan.edu/computerscience Curriculum About this program The curriculum for the major is divided into The Bachelor of Arts in Computing and Informatics is a new degree designed for three major areas: Foundation courses, Basic students who are interested in pursuing careers in information technology which requires Core Areas, and Computing and Informatics a solid understanding of the principles of computing – but not the underpinnings of Electives. computer science theory and mathematics. Such careers include, but are not limited to: The Foundation courses represent a sequence of courses primarily focused on programming Programmers Software QA / Testing Engineers skills across a variety of infrastructure Infrastructure Administrators Computer Service Coordinators platforms. Introductory courses will expose Support Technicians Deployment Technicians students to programming concepts in two different languages (e.g.,, Java, C++ or (e.g., Help Desk support) (e.g., end-user support for system releases) Python). Students will then master more Technical Application Trainers Technical Documentation Specialists complex programming via the completion of two Advanced Programming Workshops. How does this program differ from the B.S. in Computer Students will also be required to complete the Science? Basic Core Areas which cover data structures, In comparison to the existing B.S. in Computer Science, this -

ALGORITHMS of INFORMATICS Volume 3 Antoncom Budapest, 2011
ALGORITHMS OF INFORMATICS Volume 3 AnTonCom Budapest, 2011 This electronic book was prepared in the framework of project Eastern Hungarian Informatics Books Repository no. TÁMOP-4.1.2-08/1/A-2009-0046. This electronic book appeared with the support of European Union and with the co-financing of European Social Fund. Editor: Antal Iványi Authors of Volume 3: Béla Vizvári (Chapter 24), Antal Iványi and Shariefuddin Pirzada (Chapter 25), Zoltán Kása, and Mira-Cristiana Anisiu (Chapter 26), Ferenc Szidarovszky and László Domoszlai, (Chapter 27), László Szirmay-Kalos and László Szécsi (Chapter 28), Antal Iványi (Chapter 29), Shariefuddin Pirzada, Antal Iványi and Muhammad Ali Khan (Chapter 30) Validators of Volume 3: Gergely Kovács (Chapter 24), Zoltán Kása (Chapter 25), Antal Iványi (Chapter 26), Sándor Molnár (Chapter 27), György Antal (Chapter 28), Zoltán Kása (Chapter 29), Zoltán Kása (Chapter 30), Anna Iványi (Bibliography) c 2011 AnTonCom Infokommunikációs Kft. Homepage: http://www.antoncom.hu/ Contents Introduction to Volume 3 ........................... 1207 24.The Branch and Bound Method ..................... 1208 24.1. An example: the Knapsack Problem ................. 1208 24.1.1. The Knapsack Problem .................... 1209 24.1.2. A numerical example ...................... 1211 24.1.3. Properties in the calculation of the numerical example . 1214 24.1.4. How to accelerate the method ................. 1216 24.2. The general frame of the B&B method ................ 1217 24.2.1. Relaxation ............................ 1217 24.2.2. The general frame of the B&B method ............ 1224 24.3. Mixed integer programming with bounded variables ......... 1229 24.3.1. The geometric analysis of a numerical example . 1230 24.3.2. The linear programming background of the method . -

Integrated Biomedical and Clinical Research Informatics for Translational Medicine and Therapeutics”
“Integrated Biomedical and Clinical Research Informatics for Translational Medicine and Therapeutics” J. Richard Landis, PhD Robert M. Curley, MS Gregg Fromell, MD Center for Clinical Epidemiology and Biostatistics (CCEB) Office of Human Research (OHR) University of Pennsylvania School of Medicine CCEB Philadelphia, PA 19104-6021 http://cceb.med.upenn.edu/main/index.html CCEB 2 http://www.med.upenn.edu/ohr The Office of Human Research (OHR) seeks to promote human research for the advancement of healthcare while ensuring the highest level of research participant safety and facilitating the highest quality research by: • Realizing the best research standards through adherence to University and government research policies and regulations • Supporting investigators and research teams through process improvement, innovative technologies, and education and training initiatives • Propagating best operational practices to maximize the efficiencies of research activities CCEB • Collaborating with University organizations involved with human 3 research Introduction • NIH increasingly promotes translational collaborations among basic science and clinical research programs • SCCORs, PPGs, U01s illustrate interplay of translational science, requiring data integration across the entire research enterprise (basic, translational, clinical) • Biostatistics -- fundamental challenge at the data analytic stage, incorporating data elements from all sources into comprehensive risk and/or efficacy models • Data management systems -- typically isolated, not -

Distributed Cognition: Understanding Complex Sociotechnical Informatics
Applied Interdisciplinary Theory in Health Informatics 75 P. Scott et al. (Eds.) © 2019 The authors and IOS Press. This article is published online with Open Access by IOS Press and distributed under the terms of the Creative Commons Attribution Non-Commercial License 4.0 (CC BY-NC 4.0). doi:10.3233/SHTI190113 Distributed Cognition: Understanding Complex Sociotechnical Informatics Dominic FURNISSa,1, Sara GARFIELD b, c, Fran HUSSON b, Ann BLANDFORD a and Bryony Dean FRANKLIN b, c a University College London, Gower Street, London; UK b Imperial College Healthcare NHS Trust, London; UK c UCL School of Pharmacy, London; UK Abstract. Distributed cognition theory posits that our cognitive tasks are so tightly coupled to the environment that cognition extends into the environment, beyond the skin and the skull. It uses cognitive concepts to describe information processing across external representations, social networks and across different periods of time. Distributed cognition lends itself to exploring how people interact with technology in the workplace, issues to do with communication and coordination, how people’s thinking extends into the environment and sociotechnical system architecture and performance more broadly. We provide an overview of early work that established distributed cognition theory, describe more recent work that facilitates its application, and outline how this theory has been used in health informatics. We present two use cases to show how distributed cognition can be used at the formative and summative stages of a project life cycle. In both cases, key determinants that influence performance of the sociotechnical system and/or the technology are identified. We argue that distributed cognition theory can have descriptive, rhetorical, inferential and application power. -

Technical Standards for Bioinformatics and Medical Informatics
SJ Quinney College of Law, University of Utah Utah Law Digital Commons Utah Law Faculty Scholarship Utah Law Scholarship 8-2020 Technical Standards For Bioinformatics and Medical Informatics Jorge L. Contreras Adrian Thorogood Follow this and additional works at: https://dc.law.utah.edu/scholarship Part of the Health Information Technology Commons Forthcoming in Bioinformatics, Medical Informatics and the Law (Jorge L. Contreras, A. James Cuticchia & Gregory Kirsch, eds., Edward Elgar: 2021) TECHNICAL STANDARDS FOR BIOINFORMATICS AND MEDICAL INFORMATICS Jorge L. Contreras* and Adrian Thorogood† Contents INTRODUCTION I. STANDARDS AND STANDARD SETTING: A BRIEF OVERVIEW A. Types of Standards B. Standards Development Organizations II. COMPETITION AND ANTITRUST ISSUES IN STANDARDS DEVELOPMENT A. Improper Exclusion B. Improper Exchange of Information C. Compliance Certification D. Abuse of Process E. Policies and Precautions III. INTELLECTUAL PROPERTY AND STANDARDS DEVELOPMENT A. Copyright in Standards B. Patenting and Standards C. SDO Patent Policies IV. THE INFORMATICS STANDARDS LANDSCAPE A. Terminological Artifacts B. Reporting Requirements C. Exchange Formats D. Other V. INFORMATICS STANDARDS POLICIES TODAY: ASSESSMENT AND RECOMMENDATIONS A. Summary of Informatics SDO Policies B. Policy Recommendations C. Making Policies Binding CONCLUSIONS APPENDIX 1 - Selected Bioinformatics and Health Informatics Standards Development Organizations and Standards APPENDIX 2 - Sample Informatics “Open” Standards Development Policy * Presidential Scholar and Professor of Law, University of Utah S.J. Quinney College of Law; Adjunct Professor, Department of Human Genetics, University of Utah School of Medicine. † Academic Associate, Centre of Genomics and Policy (CGP), McGill University; Regulatory and Ethics Manager, Global Alliance for Genomics and Health (GA4GH). Thorogood acknowledges funding support from the Canadian Institutes of Health Research, Genome Canada, and Genome Quebec.