The External Jugular Vein As an Injection Site in Radionuclide Angiography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Variants of the Emissary Veins: Unilateral Aplasia of Both the Sigmoid Sinus and the Internal Jugular Vein and Development of the Petrosquamosal Sinus
Folia Morphol. Vol. 70, No. 4, pp. 305–308 Copyright © 2011 Via Medica C A S E R E P O R T ISSN 0015–5659 www.fm.viamedica.pl Anatomical variants of the emissary veins: unilateral aplasia of both the sigmoid sinus and the internal jugular vein and development of the petrosquamosal sinus. A rare case report O. Kiritsi1, G. Noussios2, K. Tsitas3, P. Chouridis4, D. Lappas5, K. Natsis6 1“Hippokrates” Diagnostic Centre of Kozani, Greece 2Laboratory of Anatomy in Department of Physical Education and Sports Medicine at Serres, “Aristotle” University of Thessaloniki, Greece 3Orthopaedic Department of General Hospital of Kozani, Greece 4Department of Otorhinolaryngology of “Hippokration” General Hospital of Thessaloniki, Greece 5Department of Anatomy of Medical School of “National and Kapodistrian” University of Athens, Greece 6Department of Anatomy of the Medical School of “Aristotle” University of Thessaloniki, Greece [Received 9 August 2011; Accepted 25 September 2011] We report a case of hypoplasia of the right transverse sinus and aplasia of the ipsilateral sigmoid sinus and the internal jugular vein. In addition, development of the petrosquamosal sinus and the presence of a large middle meningeal sinus and sinus communicans were observed. A 53-year-old Caucasian woman was referred for magnetic resonance imaging (MRI) investigation due to chronic head- ache. On the MRI scan a solitary meningioma was observed. Finally MR 2D veno- graphy revealed this extremely rare variant. (Folia Morphol 2011; 70, 4: 305–308) Key words: hypoplasia, right transverse sinus, aplasia, ipsilateral sigmoid sinus, petrosquamosal sinus, internal jugular vein INTRODUCTION CASE REPORT Emissary veins participate in the extracranial A 53-year-old Caucasian woman was referred for venous drainage of the dural sinuses of the poste- magnetic resonance imaging (MRI) investigation due to rior fossa, complementary to the internal jugular chronic frontal headache complaints. -

Variant Anatomy of the External Jugular Vein
ORIGINAL COMMUNICATION Anatomy Journal of Africa. 2015. 4(1): 518 – 527 VARIANT ANATOMY OF THE EXTERNAL JUGULAR VEIN Beda O. Olabu, Poonamjeet K. Loyal, Bethleen W. Matiko, Joseph M. Nderitu , Musa K. Misiani, Julius A. Ogeng’o Corresponding Author: Beda Otieno Olabu P.O.Box 30197 – 00100 GPO, Nairobi Kenya Email: [email protected] or [email protected]. Cell phone: +254 720 915 805 or +254 736 791 617 ABSTRACT Variant anatomy of the external jugular vein is important when performing invasive procedures in the neck. Although there are a number of case reports on some of these variations, there are few descriptive cross-sectional regarding the same. This study therefore aimed at describing the variant anatomy of the external jugular vein as seen in a sample Kenyan population. One hundred and six (106) sides of the neck from 53 cadaveric specimens (70 males and 36 females) in the Department of Human Anatomy, University of Nairobi, Kenya, were used. Pattern and level of formation, course, communications and termination were studied by dissection. The vein was absent in 14.2% of cases, all males. It was formed within the substance of the parotid gland in 44%, and did not receive posterior auricular vein in 6.6%. Variant communications noted included facial vein, internal jugular, and a presence of a large anastomotic vein connecting it to the anterior jugular. It was duplicated in 2.2% cases and terminated into internal jugular vein in 7.7% of cases. The most common variations were in origin, course, communications and termination. These may limit its clinical utilization, and their awareness is important when considering the vein for any invasive procedure. -

Redalyc.Termination of the Facial Vein Into the External Jugular Vein: An
Jornal Vascular Brasileiro ISSN: 1677-5449 [email protected] Sociedade Brasileira de Angiologia e de Cirurgia Vascular Brasil D'Silva, Suhani Sumalatha; Pulakunta, Thejodhar; Potu, Bhagath Kumar Termination of the facial vein into the external jugular vein: an anatomical variation Jornal Vascular Brasileiro, vol. 7, núm. 2, junio, 2008, pp. 174-175 Sociedade Brasileira de Angiologia e de Cirurgia Vascular São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=245016526015 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative CASE REPORT Termination of the facial vein into the external jugular vein: an anatomical variation Terminação da veia facial na veia jugular externa: uma variação anatômica Suhani Sumalatha D’Silva, Thejodhar Pulakunta, Bhagath Kumar Potu* Abstract Resumo Different patterns of variations in the venous drainage have been Padrões distintos de variações na drenagem venosa já foram observed in the past. During routine dissection in our Department of observados. Durante a dissecção de rotina em nosso Departamento Anatomy, an unusual drainage pattern of the veins of the left side of de Anatomia, observou-se um padrão incomum de drenagem das veias the face of a middle aged cadaver was observed. The facial vein do lado esquerdo da face de um cadáver de meia idade. A veia facial presented a normal course from its origin up to the base of mandible, apresentava curso normal de sua origem até a base da mandíbula, e and then it crossed the base of mandible posteriorly to the facial artery. -

Ó Drainage of External Jugular Vein Into an Unusually Wider Internal
JKIMSU, Vol. 9, No. 3, July-September 2020 ISSN 2231-4261 CASE REPORT Drainage of External Jugular Vein into an Unusually Wider Internal Jugular Vein - A Rare Case Report Ashwija Shetty1, Suhani Sumalatha1, Sushma Prabhath1* 1Department of Anatomy, Kasturba Medical College Manipal, Manipal Academy of Higher Education, Manipal-576104 (Karnataka) India Abstract: The superficial veins are of utmost importance formed at the base of the skull by the union of the clinically for cannulation, which is required for sigmoid sinus and inferior petrosal sinus, runs diagnostic purposes and intravenous therapy. One such vertically downwards to unite with the SV and superficial vein in the neck region is the external form the brachiocephalic vein. Jugular veins are jugular vein. The other vein, deeper in this region, is among the accessible veins for various clinical the internal jugular vein. The internal jugular vein is and diagnostic approaches. IJV is one of the routes commonly used for central venous catheterization. for Central Venous Cannulation (CVC), which is Anomaly in the course and termination of both external and Internal Jugular Veins (IJV) are critical as feasible and accessible in almost all age groups. they serve as an important route/site to perform various EJV also serves as an alternate route for CVC diagnostic or therapeutic procedures. Present case especially in children in shock, dehydration and shows a rare variation of termination of the right also cardiac patients with higher rates of success external jugular vein into an unusually wider IJV. [1-2]. Variation as described in the present case, if found, EJV is an easily accessible superficial vein in the would ease the clinicians' task to approach a less neck. -

A Rare Variation of Superficial Venous Drainage Pattern of Neck Anatomy Section
ID: IJARS/2014/10764:2015 Case Report A Rare Variation of Superficial Venous Drainage Pattern of Neck Anatomy Section TANWI GHOSAL(SEN), SHABANA BEGUM, TANUSHREE ROY, INDRAJIT GUPta ABSTRACT jugular vein is very rare and is worth reporting. Knowledge Variations in the formation of veins of the head and neck of the variations of external jugular vein is not only important region are common and are well explained based on their for anatomists but also for surgeons and clinicians as the embryological background. Complete absence of an vein is frequently used for different surgical procedures and important and major vein of the region such as external for obtaining peripheral venous access as well. Keywords: Anomalies, External jugular vein, Retromandibular vein CASE REPOrt the subclavian vein after piercing the investing layer of deep During routine dissection for undergraduate students in the cervical fascia [1]. Apart from its formative tributaries, the Department of Anatomy of North Bengal Medical College, tributaries of EJV are anterior jugular vein, posterior external Darjeeling, an unusual venous drainage pattern of the head jugular vein, transverse cervical vein, suprascapular vein, and neck region was found on the right side in a middle aged sometimes occipital vein and communications with internal female cadaver. The right retromandibular vein (RMV) was jugular vein [Table/Fig-4]. formed within the parotid gland by the union of right maxillary During embryonic period, superficial head and neck veins and superficial temporal vein. The RMV which was wider than develop from superficial capillary plexuses which will later facial vein continued downwards and joined with the facial form primary head veins. -

Unilateral Duplication of the External Jugular Vein: a Case Report with Embryological Significance and Clinical Implications
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Unilateral Duplication of the External Jugular Vein: A Case Report with Embryological Significance and Clinical Implications Suresh B S1, Shivaleela C2, Kumar G V3 1Professor of Anatomy, 2Assistant Professor of Anatomy, 3Assistant Professor of Pediatrics, Sri Siddhartha Medical College, Tumkur, Karnataka, India. Corresponding Author: Kumar G V Received: 25/07//2014 Revised: 13/08/2014 Accepted: 16/08/2014 ABSTRACT The external jugular vein, one of the main superficial veins of the head and neck, drains blood mostly from the scalp and the face. It is formed by the union of the posterior division of the retromandibular vein with the posterior auricular vein. Here we present a case report of two external jugular veins emerging from the lower border of the parotid gland on the right side in a male cadaver aged about 60years.The present case report mainly highlights the occurrence of this rare variation, its embryological basis and clinical Implications. Key words: External jugular vein, Facial vein, Retromandibular vein, Variations. INTRODUCTION of the clavicle. It crosses the The word jugular means neck. Veins sternocleidomastoid muscle obliquely and in of the neck are superficial or deep to the the subclavian triangle, perforates the deep deep fascia. Deviation from the normal fascia. It crosses the transverse cervical pattern in the vascular system is a common nerve and its upper half runs parallel to the feature and it is far commoner in the veins great auricular nerve which ascends behind than in the arteries. The relevance and it. -
27. Veins of the Head and Neck
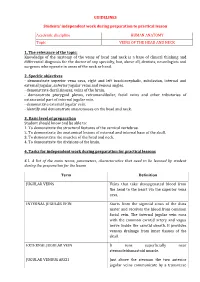
GUIDELINES Students’ independent work during preparation to practical lesson Academic discipline HUMAN ANATOMY Topic VEINS OF THE HEAD AND NECK 1. The relevance of the topic: Knowledge of the anatomy of the veins of head and neck is a base of clinical thinking and differential diagnosis for the doctor of any specialty, but, above all, dentists, neurologists and surgeons who operate in areas of the neck or head. 2. Specific objectives - demonstrate superior vena cava, right and left brachiocephalic, subclavian, internal and external jugular, anterior jugular veins and venous angles. - demonstrate dural sinuses, veins of the brain. - demonstrate pterygoid plexus, retromandibular, facial veins and other tributaries of extracranial part of internal jugular vein. - demonstrate external jugular vein. - identify and demonstrate anastomoses on the head and neck. 3. Basic level of preparation Student should know and be able to: 1. To demonstrate the structural features of the cervical vertebrae. 2. To demonstrate the anatomical lesions of external and internal base of the skull. 3. To demonstrate the muscles of the head and neck. 4. To demonstrate the divisions of the brain. 4. Tasks for independent work during preparation for practical lessons 4.1. A list of the main terms, parameters, characteristics that need to be learned by student during the preparation for the lesson Term Definition JUGULAR VEINS Veins that take deoxygenated blood from the head to the heart via the superior vena cava. INTERNAL JUGULAR VEIN Starts from the sigmoid sinus of the dura mater and receives the blood from common facial vein. The internal jugular vein runs with the common carotid artery and vagus nerve inside the carotid sheath. -

Absent External Jugular Vein – Ontogeny and Clinical Implications*
eISSN 1308-4038 International Journal of Anatomical Variations (2013) 6: 103–105 Case Report Absent external jugular vein – ontogeny and clinical implications* Published online June 23rd, 2013 © http://www.ijav.org Rashmi Avinash PATIL Abstract Lakshmi RAJGOPAL Variation in the formation, course and termination of vessels especially veins is more a norm in anatomy than a rarity. It is only to be expected because the development of an artery or a vein Praveen IYER is based on the persistence of one vascular pathway and the disappearance of the rest in a mesh of plexiform channels. Yet, total absence of an important vein merits reporting; more so, if that Department of Anatomy, Seth GS Medical College, Mumbai, vein is used for peripheral venous access by clinicians. We came across absence of right external INDIA. jugular vein during routine dissection of an adult male cadaver. The knowledge of absence of external jugular vein is also important with reference to reconstructive surgeries of head and neck. The details of this variation and its embryological basis are discussed here. Dr. Rashmi Avinash Patil Assistant Professor © Int J Anat Var (IJAV). 2013; 6: 103–105. Department of Anatomy Seth GS Medical College & KEM Hospital Acharya Donde Marg Parel, Mumbai 400012, Maharashtra, INDIA. +91 (22) 24107447 [email protected] Received April 16th, 2012; accepted September 29th, 2012 Key words [external jugular vein] [variation] Introduction drain into the internal jugular vein. The cephalic vein of the The external jugular vein (EJV) is one of the superficial veins same side was seen to drain into the right subclavian vein of the neck (the other being the anterior jugular vein). -

Endovascular Approaches to the Cavernous Sinus in the Setting of Dural Arteriovenous Fistula
brain sciences Review Endovascular Approaches to the Cavernous Sinus in the Setting of Dural Arteriovenous Fistula Justin Dye 1,*, Gary Duckwiler 2, Nestor Gonzalez 3, Naoki Kaneko 2, Robert Goldberg 4, Daniel Rootman 4, Reza Jahan 2, Satoshi Tateshima 2 and Viktor Szeder 2 1 Department of Neurosurgery, Loma Linda University, Loma Linda, CA 92354, USA 2 Division of Interventional Neuroradiology, Department of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, CA 90095, USA; [email protected] (G.D.); [email protected] (N.K.); [email protected] (R.J.); [email protected] (S.T.); [email protected] (V.S.) 3 Department of Neurosurgery, Cedars-Sinai Medical Center, Los Angeles, CA 90048, USA; [email protected] 4 Department of Ophthalmology, David Geffen School of Medicine, University of California, Los Angeles, CA 90095, USA; [email protected] (R.G.); [email protected] (D.R.) * Correspondence: [email protected]; Tel.: +1-909-558-6338 Received: 16 July 2020; Accepted: 12 August 2020; Published: 14 August 2020 Abstract: Dural arteriovenous fistulas involving the cavernous sinus can lead to orbital pain, vision loss and, in the setting of associated cortical venous reflux, intracranial hemorrhage. The treatment of dural arteriovenous fistulas has primarily become the role of the endovascular surgeon. The venous anatomy surrounding the cavernous sinus and venous sinus thrombosis that is often associated with these fistulas contributes to the complexity of these interventions. The current report gives a detailed description of the alternate endovascular routes to the cavernous sinus based on a single center’s experience as well as a literature review supporting each approach. -
L.The External Jugular Vein
& Technology Medical Radiological Sciences iagnostic Department INIS-SD-141 HIP SD0000066 this Thesis for the ofB.S.C Supervised By: UST.\ Abdel Samad Mo PAGES ARE MISSING IN THE ORIGINAL DOCUMENT Table of Contents Page Introduction A Dedication B Acknowledgment C Common Abbreviations D Chapter one: 1 - Introduction - The Significant of the study - Research problems - The rational^ of the study - The objectives of the study - The Hypotheses - Research Termonologies - Methodology of research sample - Obstacles Chapter Two: Anatomy of the Skull 4 Chapter Three : Research Procedure 22 Chapter Four : Results, Conclusion & Recommendations 53 Bibliography 54 Appendices introduction Patterns recognition leading to differential diagnosis is the essence of imaging when face with specific finding on plain radiograph CT, MR. N.M and ultra sound and this research offer imaging of skulls related to the disease. Added to this lists are description of specific imaging finding to be expected for each diagnostic entity and help the technologist to choose the most suitable position when certain disease is suspected. (A) Dedication Our families Our Friends Our Colleagues... (B) Acknowledgment We would like to express our thanks to Dr Abdei Samad Mohammed Salih for his uniimited help in the completion of this work. Thanks are also extended to the New X- Ray section in Khartoum Hospital. Thanks are also to those who help directly or indirectly hi this research. (C) Common Abbreviations CJ.N.S Central Nervous System. C.S.O.M Chronic Suppurative Otitis Media C.T. Coronary thrombosis or Cerebral thrombosis or Computerize topography. C.V.A Cerebro Vascular Accident D.S. A Digital Subtraction Angiography F.O. -

Original Article Venous Variations of the Neck and the Inferior Vena Cava: Two Cadaveric Case Reports
Int J Clin Exp Med 2019;12(7):9273-9276 www.ijcem.com /ISSN:1940-5901/IJCEM0091907 Original Article Venous variations of the neck and the inferior vena cava: two cadaveric case reports Yan-Ru Zhang1, Kaka AA Katiella2, Ge-Chen Zhang2 1Institute of Orthopedics of Henan Polytechnic University, Jiaozuo 454000, Henan Province, China; 2Medical College of Zhengzhou University, Zhengzhou 450051, Henan Province, China Received January 27, 2019; Accepted April 11, 2019; Epub July 15, 2019; Published July 30, 2019 Abstract: Anatomical variations in the venous system of the head and neck remain important for clinicians and also for radiologists and surgeons. This paper reports a case of a unilateral cervical vein variation and a disproportion of the inferior vena cava to the aorta observed in two adult male cadavers. Out of twenty well preserved dissected cadavers, these findings are rare, even in the medical literature. The left external jugular vein was formed by three proximal tributaries draining to it. The left internal jugular vein bears lymph nodes and was smaller in diameter than the right pair. As a normal pattern, the right and left subclavian veins drained to the superior vena cava. In the sec- ond cadaver, the inferior vena cava was found to be abnormal prior to its opening to the right atrium. Keywords: Veins of the neck, inferior vena cava, variations, cadavers Introduction cipital, posterior external jugular, anterior jugu- lar and transverse cervical veins [5]. Yadav et The veins draining the regions of the face and al. [2] said that the external jugular vein is used neck establish their identity only after the de- as a venos manometer and for catheterization velopment of the skull. -

The Veins of the Oesophagus by H
Thorax: first published as 10.1136/thx.6.3.276 on 1 September 1951. Downloaded from horax (1951), 6, 276. THE VEINS OF THE OESOPHAGUS BY H. BUTLER From the School of Anatomy, Cambridge (RECEIVED FOR PUBLICATION MAY 30, 1951) Among the early anatomists, Vesalius (1543) pictured the oesophageal branches of the left gastric vessels lying close to the vagus nerves. According to Bartholin (1673) the veins of the oesophagus drain into the azygos, intercostal, and jugular veins. Dionis (1703) was probably the first to point out that the veins of the oesophagus drain into the left gastric vein. Portal (1803) described oesophageal veins going to the main veins of the neck and thorax, including the bronchial veins, and to the left gastric vein. According to Preble (1900), Fauvel reported the first case of rupture of oeso- phageal varices in cirrhosis of the liver in 1858. This stimulated a considerable amount of interest in the anastomoses between the portal and systemic veins, and a number of French investigators examined the veins of the oesophagus from this point of view (Kundrat, 1886; Dusaussay, 1877; Duret, 1878; and Mariau, 1893). copyright. Their accounts are at variance on many points, particularly with regard to the area of the oesophagus draining into the portal vein. Kundrat regarded the lower one- third of the oesophagus as draining into the portal vein; according to Dusaussay and Mariau the lower two-thirds did so. None of these investigators mentioned valves or discussed the possible effect of pressure differences between the portal http://thorax.bmj.com/ and systemic veins.