Strategic Plan for Limerick City 2009 - 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

National Library of Ireland
ABOUT TOWN (DUNGANNON) AISÉIRGHE (DUBLIN) No. 1, May - Dec. 1986 Feb. 1950- April 1951 Jan. - June; Aug - Dec. 1987 Continued as Jan.. - Sept; Nov. - Dec. 1988 AISÉIRÍ (DUBLIN) Jan. - Aug; Oct. 1989 May 1951 - Dec. 1971 Jan, Apr. 1990 April 1972 - April 1975 All Hardcopy All Hardcopy Misc. Newspapers 1982 - 1991 A - B IL B 94109 ADVERTISER (WATERFORD) AISÉIRÍ (DUBLIN) Mar. 11 - Sept. 16, 1848 - Microfilm See AISÉIRGHE (DUBLIN) ADVERTISER & WATERFORD MARKET NOTE ALLNUTT'S IRISH LAND SCHEDULE (WATERFORD) (DUBLIN) March 4 - April 15, 1843 - Microfilm No. 9 Jan. 1, 1851 Bound with NATIONAL ADVERTISER Hardcopy ADVERTISER FOR THE COUNTIES OF LOUTH, MEATH, DUBLIN, MONAGHAN, CAVAN (DROGHEDA) AMÁRACH (DUBLIN) Mar. 1896 - 1908 1956 – 1961; - Microfilm Continued as 1962 – 1966 Hardcopy O.S.S. DROGHEDA ADVERTISER (DROGHEDA) 1967 - May 13, 1977 - Microfilm 1909 - 1926 - Microfilm Sept. 1980 – 1981 - Microfilm Aug. 1927 – 1928 Hardcopy O.S.S. 1982 Hardcopy O.S.S. 1929 - Microfilm 1983 - Microfilm Incorporated with DROGHEDA ARGUS (21 Dec 1929) which See. - Microfilm ANDERSONSTOWN NEWS (ANDERSONSTOWN) Nov. 22, 1972 – 1993 Hardcopy O.S.S. ADVOCATE (DUBLIN) 1994 – to date - Microfilm April 14, 1940 - March 22, 1970 (Misc. Issues) Hardcopy O.S.S. ANGLO CELT (CAVAN) Feb. 6, 1846 - April 29, 1858 ADVOCATE (NEW YORK) Dec. 10, 1864 - Nov. 8, 1873 Sept. 23, 1939 - Dec. 25th, 1954 Jan. 10, 1885 - Dec. 25, 1886 Aug. 17, 1957 - Jan. 11, 1958 Jan. 7, 1887 - to date Hardcopy O.S.S. (Number 5) All Microfilm ADVOCATE OR INDUSTRIAL JOURNAL ANOIS (DUBLIN) (DUBLIN) Sept. 2, 1984 - June 22, 1996 - Microfilm Oct. 28, 1848 - Jan 1860 - Microfilm ANTI-IMPERIALIST (DUBLIN) AEGIS (CASTLEBAR) Samhain 1926 June 23, 1841 - Nov. -

Publications
Publications National Newspapers Evening Echo Irish Examiner Sunday Business Post Evening Herald Irish Field Sunday Independent Farmers Journal Irish Independent Sunday World Irish Daily Star Irish Times Regional Newspapers Anglo Celt Galway City Tribune Nenagh Guardian Athlone Topic Gorey Echo New Ross Echo Ballyfermot Echo Gorey Guardian New Ross Standard Bray People Inish Times Offaly Express Carlow Nationalist Inishowen Independent Offaly Independent Carlow People Kerryman Offaly Topic Clare Champion Kerry’s Eye Roscommon Herald Clondalkin Echo Kildare Nationalist Sligo Champion Connacht Tribune Kildare Post Sligo Weekender Connaught Telegraph Kilkenny People South Tipp Today Corkman Laois Nationalist Southern Star Donegal Democrat Leinster Express Tallaght Echo Donegal News Leinster Leader The Argus Donegal on Sunday Leitrim Observer The Avondhu Donegal People’s Press Letterkenny Post The Carrigdhoun Donegal Post Liffey Champion The Nationalist Drogheda Independent Limerick Chronnicle Tipperary Star Dublin Gazette - City Limerick Leader Tuam Herald Dublin Gazette - North Longford Leader Tullamore Tribune Dublin Gazette - South Lucan Echo Waterford News & Star Dublin Gazette - West Lucan Echo Western People Dundalk Democrat Marine Times Westmeath Examiner Dungarvan Leader Mayo News Westmeath Independent Dungarvan Observer Meath Chronnicle Westmeath Topic Enniscorthy Echo Meath Topic Wexford Echo Enniscorthy Guardian Midland Tribune Wexford People Fingal Independent Munster Express Wicklow People Finn Valley Post Munster Express Magazines -

Limerick Timetables
Limerick B A For more information For online information please visit: locallinklimerick.ie Call us at: 069 78040 Email us at: [email protected] Ask your driver or other staff member for assistance Operated By: Local Link Limerick Fares: Adult Return/Single: €5.00/€3.00 Student & Child Return/Single: €3.00/€2.00 Adult Train Connector: €1.50 Student/Child Train Connector: €1.00 Multi Trip Adult/Child: €8.00/€5.00 Weekly Student/Child: €12.00 5 day Weekly Adult: €20.00 6 day Weekly Adult: €25.00 Free Travel Pass holders and children under 5 years travel free Our vehicles are wheelchair accessible Contents Route Page Ballyorgan – Ardpatrick – Kilmallock – Charleville – Doneraile 4 Newcastle West Service (via Glin & Shanagolden) 12 Charleville Child & Family Education Centre 20 Spa Road Kilfinane to Mitchelstown 21 Mountcollins to Newcastle West (via Dromtrasna) 23 Athea Shanagolden to Newcastle West Desmond complex 24 Castlemahon via Ballingarry to Newcastle West - Desmond Complex 25 Castlmahon to Newcastle West - Desmond Complex 26 Ballykenny to Newcastle West- Desmond Complex 27 Shanagolden to Newcastle West - Special Olympics 28 Tournafulla to Newcastle West - Special Olympics 29 Abbeyfeale to Newcastle West - Special Olympics 30 Elton to Hospital 31 Adare to Newcastle West 32 Kilfinny via Adare to Newcastle West 33 Feenagh via Ballingarry to Newcastle West - Desmond Complex 34 Knockane via Patrickswell to Dooradoyle 35 Knocklong to Dooradoyle 36 Rathkeale via Askeaton to Newcastle West to Desmond Complex 37 Ballingarry to -

Political Constructions of Transnational EU Migrants in Ireland
FROM THE MOUTHS OF JANUS: Political constructions of transnational EU migrants in Ireland Martin J. Power, Amanda Haynes, Eoin Devereux Introduction INTERNATIONAL RESEARCH INDICATES that recessionary periods may be accom- panied by a decline in the quality of relations between the majority population and migrant groups as the latter are at risk of being scapegoated for the economic down- turn. In that context, political leadership on the matter of immigration is of crucial importance, with political parties having a key role to play in framing how the public understand immigration. This article is based on research which examined how politicians construct non-Irish EU immigrants to Ireland through an analysis of the content of statements attributed to this group in the print media. The article focuses on those statements relating to welfare and the economy, which were among a larger range of themes identified in the wider study. Our sample of articles demonstrates that representatives on both the left and right of the political spectrum were found to commonly address the issue of immigration as a social problem, whether by contributing to its framing as a problem, or by seek- ing to contradict its problematisation. In particular, our analysis demonstrated that some representatives of mainstream parties contribute to a discourse whereby migrants are constructed as fraudulent and as burdens on the economy. Drawing on theories (McLaren and Johnson, ;Blumer,;Quillian,;Espenshadeand Hempstead, ) that link anti-immigrant hostility to perceptions of resource com- petition, our paper argues that such political constructions of EU migrants reflect a neoliberal understanding of citizenship which prioritises the economic citizen. -

Derelict Sites Register - 2020
DERELICT SITES REGISTER - 2020 REF NUMBER LOCATION OF LAND DESIGNATED AREA EIRCODE 1 DS-001-91 4 Wellesley Lane, (off Henry Street), Limerick. Limerick City West 2 DS-002-91 3 Wellesley Lane, (off Henry Street), Limerick. Limerick City West 3 DS-003-91 2 Wellesley Lane, (off Henry Street), Limerick. Limerick City West 4 DS-004-91 1 Wellesley Lane, (off Henry Street), Limerick. Limerick City West 5 DS-005-91 23 Wickham Street, Limerick. Limerick City West V94 XN53 6 DS-006-91 22 Wickham Street, Limerick. Limerick City West V94 P2F6 7 DS-001-93 Knightstreet, Ballingarry, Co. Limerick. Adare/Rathkeale 8 DS-004-04 West end, Kilfinane, Co. Limerick. Kilmallock/ Cappamore 9 DS-005-04 Disused Shop & Shed, Kilfinane, Co. Limerick. Kilmallock/ Cappamore 10 DS-007-04 Main St Croom, Co. Limerick. Adare/Rathkeale 11 DS-011-04 The Square, Kilfinane, Co. Limerick. Kilmallock/ Cappamore 12 DS-001-05 Market House, Kilfinane, Co. Limerick. Kilmallock/ Cappamore 13 DS-005-05 Glengort Schoolhouse, Tournafulla Newcastlewest 14 DS-008-06 Main Street, Bruff, Co. Limerick. Kilmallock/ Cappamore 15 DS-009-06 Ballyvulhane, Bruff, Co. Limerick. Kilmallock/ Cappamore 16 DS-001-07 Corgrigg, Foynes, Co. Limerick. Adare/Rathkeale 17 DS-003-08 Cogan Street, Limerick. Limerick City West 18 DS-007-08 Ballyneety North, Templebredon, Co. Limerick. Kilmallock/ Cappamore Creamery Store/Londis, Herbertstown, Co. 19 DS-003-09 Kilmallock/ Cappamore Limerick. 20 DS-002-10 Athea Upper, Athea, Co. Limerick. Newcastlewest 21 DS-017-12 86 Lenihan Avenue, Limerick. Limerick City West 22 DS-016-11 106 Hyde Road, Limerick. -
Limerick Manual
RECORD OF MONUMENTSAND PLACES as Established under Section 12 of the National Monuments ’ (Amendment)Act 1994 COUNTYLIMERICK Issued By National Monumentsand Historic Properties Service 1997 j~ Establishment and Exhibition of Record of Monumentsand Places under Section 12 of the National Monuments (Amendment)Act 1994 Section 12 (1) of the National Monuments(Amendment) Act 1994 states that Commissionersof Public Worksin Ireland "shall establish and maintain a record of monumentsand places where they believe there are monumentsand the record shall be comprised of a list of monumentsand such places and a mapor mapsshowing each monumentand such place in respect of each county in the State." Section 12 (2) of the Act provides for the exhibition in each county of the list and mapsfor that county in a mannerprescribed by regulations madeby the Minister for Arts, Culture and the Gaeltacht. The relevant regulations were made under Statutory Instrument No. 341 of 1994, entitled National Monuments(Exhibitior~ of Record of Monuments)Regulations, 1994. This manualcontains the list of monumentsand places recorded under Section 12 (1) of the Act for the Countyof Limerick whichis exhibited along with the set of mapsfor the Countyof Limerick showingthe recorded monumentsand places. Protection of Monumentsand Places included in the Record Section 12 (3) of the Act provides for the protection of monumentsand places included in the record stating that "When the owner or occupier (not being the Commissioners) of monumentor place which has been recorded under -

Graigue, Adare Aidan and Róisín
Adrian Kelly - Broad street, Adare Aidan and Denise Hayes - Graigue, Adare Aidan and Róisín Lee - Graigue, Adare Alan Fitzpatrick - Rathkeale Road, Adare Andrew Normoyle - The Avenue, Adare Andy O'Connell - Knockanes, Adare Anita and Paudie Griffin - 63 The Village, Adare Anne and Hans Droog - 3 Woodlands, Adare Anne Geary - 31 The Village, Adare Bill Heffernan - Kilbreedy, Kilcornan Brenda Fitzgerald - Graigue, Adare Brian Hall and Sinead O'Donoghue - 62 The Village, Adare Catherine O'Grady - Beabus, Adare Chris and Deidre Moore - Rossbeigh, Cummeen, Adare Colette and Pat Hackett - Gortfadda, Adare Colm and Marie Cribbin - Curraghbeg, Adare Conor Geaney - Knockanes, Adare Damien Mordan and Trisha Lavin - 25 Abbey View, Adare Dan and Lorna Sheehan - 6 Abbeyview, Station Road, Adare Darina Drumm - Nurses Cottage, Rathkeale Road, Adare David and Bernie Minogue - Tiglin, Graigue, Adare Declan and Nicola Maxwell - 7 Limetree Avenue, Adare Declan Fitzgerald - Graigue, Adare Derry and Aisling Heraty - 65 The Village, Adare Diarmaid and Sinead FitzGerald - Graigue, Adare Diarmuid Geary - The Demense, Adare Donncha Sheehan - 6, Abbey View, Adare Eamonn and Aisling Fitzgerald - Gortnagrour, Adare Eamonn Kirby - Kilknockan, Adare Ed Joyce and Siobhan Clifford - Graigue, Adare Eoghan Toomey - Tuogh, Adare Evelyn and Kieran O’Brien - Graigue, Adare Fergal McNamara and Nicky McMahon – 5 The Village , Adare Fionan Kelliher and Eavan Sheehan - Graigue, Adare Gerard and Helen Barry - 33 The Village, Adare Gillian Griffin - 9 The Village, Adare Grace McNamara -

Dear Sir/Madam, As a Limerick Native I Feel Passionately About My Home
Dear Sir/Madam, As a Limerick native I feel passionately about my home town, Limerick City. I applaud the efforts made by all those involved so far but feel that there should be significantly more ambition in terms of our housing and public transport networks. Limerick is at a size currently that allows us to plan for future growth, which is why we need to design and implement a light rail network now ahead of that growth, one which we can grow into in the future. I would implore you to design the city with a population of 300,000 in mind. I would also suggest and request that Limerick-Shannon, Cork and Waterford be allowed to update their MASPS as and when local development plans are put in place. For ease of reference I have attached a clean copy and marked up version of the Draft RSES which show my proposed and considered changes to the existing draft RSES. I trust you will take them under consideration. Thanking you in advance. Is mise le meas, p.s. I sent this email and its attachments from my personal account earlier today and also made a submission online. Apologies for the overlap. 1.0 | Introduction 1.1 | Overview Limerick City is the largest urban centre in Ireland’s Mid-West and the country’s third largest city. The NPF supports ambitious growth targets to enable Limerick City to grow by at least 50% to 2040 and to enhance its significant potential to become a city of scale. Shannon is a significant employment centre with assets such as Shannon International Airport, Shannon FreeZone and the International Aviation Services Centre (IASC). -
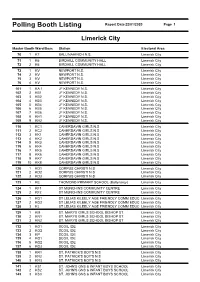
Polling Booth Listing Report Date 22/01/2020 Page 1
Polling Booth Listing Report Date 22/01/2020 Page 1 Limerick City Master Booth Ward/Desc Station Electoral Area 70 1 K7 BALLINAHINCH N.S. Limerick City 71 1 K6 BIRDHILL COMMUNITY HALL Limerick City 72 2 K6 BIRDHILL COMMUNITY HALL Limerick City 73 1 KV NEWPORT N.S. Limerick City 74 2 KV NEWPORT N.S. Limerick City 75 3 KV NEWPORT N.S. Limerick City 76 4 KV NEWPORT N.S. Limerick City 101 1 KA.1 JF KENNEDY N.S. Limerick City 102 2 KB1 JF KENNEDY N.S. Limerick City 103 3 KB2 JF KENNEDY N.S. Limerick City 104 4 KB3 JF KENNEDY N.S. Limerick City 105 5 KB4 JF KENNEDY N.S. Limerick City 106 6 KB5 JF KENNEDY N.S. Limerick City 107 7 KB6 JF KENNEDY N.S. Limerick City 108 8 KH1 JF KENNEDY N.S. Limerick City 109 9 KH2 JF KENNEDY N.S. Limerick City 110 1 KC1 CAHERDAVIN GIRLS N.S Limerick City 111 2 KC2 CAHERDAVIN GIRLS N.S Limerick City 112 3 KK1 CAHERDAVIN GIRLS N.S Limerick City 113 4 KK2 CAHERDAVIN GIRLS N.S Limerick City 114 5 KK3 CAHERDAVIN GIRLS N.S Limerick City 115 6 KK4 CAHERDAVIN GIRLS N.S Limerick City 116 7 KK5 CAHERDAVIN GIRLS N.S Limerick City 117 8 KK6 CAHERDAVIN GIRLS N.S Limerick City 118 9 KK7 CAHERDAVIN GIRLS N.S Limerick City 119 10 KK8 CAHERDAVIN GIRLS N.S Limerick City 120 1 KD1 CORPUS CHRISTI N.S Limerick City 121 2 KD2 CORPUS CHRISTI N.S Limerick City 122 3 KD3 CORPUS CHRISTI N.S Limerick City 123 1 KE THOMOND PRIMARY SCHOOL (Ballynanty) Limerick City 124 1 KF1 ST MUNCHINS COMMUNITY CENTRE Limerick City 125 2 KF2 ST MUNCHINS COMMUNITY CENTRE Limerick City 126 1 KG1 ST LELIAS KILEELY AGE FRIENDLY COMM EDUC Limerick City 127 2 KG2 ST LELIAS KILEELY AGE FRIENDLY COMM EDUC Limerick City 128 3 KJ ST LELIAS KILEELY AGE FRIENDLY COMM EDUC Limerick City 129 1 KM ST. -
Limerick Metropolitan District Movement Framework
Limerick City and County Council Limerick Metropolitan District Movement Framework Study 2 The following people and organisations contributed Mr David Clements to the development of the Movement Framework Organisations/Individuals consulted as part of Study: the development of the study: Limerick City and County Council: Ultan Gogarty – Limerick Institute of Technology Paul Crowe Orlaith Borthwick, Gary Rowan – Limerick Chamber Vincent Murray Miriam Flynn – Bus Éireann Rory McDermott Joe Hoare – University Hospital Limerick Carmel Lynch Insp. Paul Reidy, Sgt. Peter Kelly – An Garda Neal Boyle Síochána John J. Ryan Helen O’Donnell, Philip Danaher – Limerick City Kieran Reeves Business Association Mairead Corrigan Brian Kirby – Mary Immaculate College Robert Reidy, John Moroney – University of Limerick Smarter Travel Office: Limerick Pat O’Neill Michael Curtin – Eurobus Limerick Lise-Ann Sheehan Consultant Members of the Project Team for National Transport Authority: delivery of the Movement Framework Study: Mr Hugh Creegan Tiago Oliveira, Arup Consulting Engineers David O’Keeffe, Arup Consulting Engineers Clifford Killeen, Arup Consulting Engineers Images Photography for this report was provided by Limerick City & County Council and Arup Consulting Engineers. Graphics for this report were provided by Arup Consulting Engineers. 3 Limerick Metropolitan District Movement Framework Study 1 Executive Summary and Introduction 7 1.1 Executive Summary 8 1.2 Introduction - The Limerick Metropolitan District Movement Framework Study 9 2 Literature -

Tickets for the Patrickswell Community Council Annual Dog Night On
Volume 12, Issue 8 September 2012 - Free Visit our website Patrickswellcommunitycouncil.wordpress.com ~ Tickets for the Patrickswell Community Council Annual Dog Night on December 7th 2012 are available from members of the Community Council or the Resource Centre from 18/10/12 ~ The Patrickswell Community Council are compiling information for a Parish Journal and are seeking your help with regard to the following: ~ School photographs past and present, stories and history of the local schools. New Property for Patrickswell Community Stories or photographs of events that Council took place such as Carnivals, Festivals, Marquees, St. Patricks Day The Community Council are in the process of purchasing parades, Sports events, Dog shows/ the Resource House from Limerick County Council. It is Coursing/Dog Racing. hoped that the contract will be signed this week. This is ~ Poems, Songs and Stories. ~ Stories and Memories of those who ~ the first step in our plans to develop a Community emigrated from the area. Centre to cater for all the needs of the Community. We ~ Births, Marriages or other celebrated have acquired a loan for the purchase from Clann Credo events. which we hope to pay back as quickly as possible. We Please contact any of the following greatly appreciate the support of the Community with committee members if you can provide our fundraising efforts to date and look forward to your any of the above, Mary O`Brien – 0876234799. support in the coming years. Our next fundraiser is a Caitriona Fitzgerald – 0879760264. Community night out at the greyhound track in Sally Walsh – 0872278979. December. The Community Council would also like to Michael McSweeney – 0879397712. -

'One Diocese,Many Stories' Limerick Diocesan Assembly
‘ONE DIOCESE, MANY STORIES’ LIMERICK DIOCESAN ASSEMBLY 5th October 2019 Rathkeale House Hotel Table of Contents Foreword ....................................................................................................... 4 Introduction ................................................................................................... 5 Community and Sense of Belonging Theme ................................................... 6 Lectio Divina; Small Christian Communities: Newcastlewest Parish .................................... 7 Welcome and Hospitality: Cratloe Parish .............................................................................. 8 Local Pilgrimage: The Well at Barrigone: St Senan’s Parish (Shanagolden / Foynes / Robertstown) ........................................................................................................................ 10 Trócaire - making the story local: Limerick Diocese Trócaire Volunteer Group .................. 13 Laudato Si; Caring for our Common Home: Salesian Sisters ............................................... 15 Traveller Outreach ............................................................................................................... 16 Missionary Outreach; Synod Group of Frontline Workers .................................................. 17 Pastoral Care of the Family Theme ............................................................... 18 Family Fun Days: World Meeting of Families Diocesan Committee .................................... 19 Visible Reminders of an Invisible