08-20WC Zebic V. Rhino Foods Inc
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Harvest Festival Saturday September 25 at the Town Hall
INSIDE PRSRT STD US Postage Letters ..............................................................................................2 PAID Town News ....................................................................................2 Hinesburg, VT Community Police ..........................................................................5 Permit No 3 Business News ................................................................................7 Carpenter Carse Library ................................................................10 School News ................................................................................11 Entertainment................................................................................15 Names in the News ......................................................................16 Hinesburg Calendar......................................................................20 S E P T E M B E R 2 3 , 2 0 1 0 Hinesburg’s Lincoln Hill Sign Dedication Harvest Festival Saturday With Vermont Author Elise Guyette Author of Discovering Black Vermont: African American September 25 at the Town Hall Farmers in Hinesburg, 1790-1890 Date: Sunday September 26 Summer is officially over and celebrations of good Time: 1:00 p.m. harvests are occurring all over Vermont. Hinesburg’s Harvest Place: At the bottom of Lincoln Hill. (Please park Festival will be held on Saturday, September 25 at the Town by the gravel pit across the street) For more information Hall. Organizers have scheduled many events and exhibits please call Brown Dog -

NOFA Notes Winter 2017-2018
Winter 2018 Enid’s Thoughts .................2 A Day in the Life .................3 “Vt Farm Kids” ...................5 Policy Update ....................6 Digging into Data ..............9 “Garden Diary” Poem .........9 Jr Iron Chef VT ................. 11 New Members ................. 10 The Quarterly Newsletter of the Northeast Organic Farming Association of Vermont Organic Matters: Culture & Agriculture Our 36th annual Winter Conference, February 17-19th, 2018 By Megan Browning, Winter Conference Coordinator & Enid Wonnacott, Executive Director With over 90 workshops, there is challenges, as well as something for everyone at the NOFA the role of the next Vermont Winter Conference! Are you generation in positive a homesteader or gardener interested in change. The theme plant propagation or raising bees? A food will be addressed enthusiast excited about making herbal throughout the medicines, or learning how to render conference – in our animal fats? Are you a commercial grower keynote addresses, interested in improving your cover crop workshops, and two system, or ready to make land succession featured films:Dolores plans? Or a beginner farmer interested and Look & See: A in learning about direct marketing and Portrait of Wendell financial planning? Want to take a deeper Berry. to essential issues that are rarely in public dive? Choose from four discourse and not reflected in agricultural full-day Monday inten- Throughout the We are thrilled to wel- policies. At Farm School NYC, the sives - Direct Marketing, conference we will address come esteemed keynote mission is to train local residents in urban Hemp, Cut Flowers or agrarianism as a catalyst speakers Mary Berry, agriculture in order to build self-reliant the Executive Director Silvopasture, with plenty for social change. -
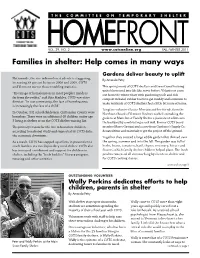
Families in Shelter: Help Comes in Many Ways
THE COMMITTEE ON TEMPORARY SHELTER VOL. 29, NO. 2 www.cotsonline.org FALL/WINTER 2011 Families in shelter: Help comes in many ways Gardens deliver beauty to uplift Nationwide, the rise in homeless students is staggering, By Amanda Petry increasing 38 percent between 2006 and 2009. COTS and Vermont mirror those troubling statistics. This spring many of COTS shelters and transitional housing units blossomed into life like never before. Volunteers came “The image of homelessness in most people’s minds is out from the winter thaw with gardening tools and rich far from the reality,” said Rita Markley, COTS executive compost in hand, rubber boots to get muddy and a mission to director. “In our community, the face of homelessness make residents at COTS shelters feel a little bit more at home. is increasingly the face of a child.” Longtime volunteer Louise Merriam and her friends from the In October, 141 schoolchildren in Chittenden County were Northwest Board of Vermont Realtors worked on making the homeless. There were an additional 48 children under age gardens at Main Street Family Shelter a permanent addition to 5 living in shelter or on the COTS shelter waiting list. the backyard by constructing a rock wall. Former COTS board The primary reason for the rise in homeless children, member Maree Gaetani and a crew from Gardener’s Supply Co. according to national study and supported by COTS data: donated time and materials to get the project off the ground. the economic downturn. Together they created a large edible garden that thrived over As a result, COTS has stepped up efforts in prevention to the spring, summer and into the fall. -

Table of Contents
TABLE OF CONTENTS City Government Electric Department. 36 City Organizational Chart . 2 Fire Department . 40 Mayor’s Message . 3 Fletcher Free Library . 43 City Officials Appointed by the Mayor . 6 Human Resources Department . 46 Vermont Legislators . 7 Innovation & Technology. 48 Mayors of Burlington . 7 Parks, Re creation & Waterfront. 49 City Council . 8 Planning & Zoning Department . 55 City Council Standing Committees . 9 Police Department. 58 City Department Information . 10 Public Works Department . 61 Important Dates . 11 School District . 66 City Holidays. 11 Telecom, Burlington . 71 Board of School Commissioners . 12 Regional Organizations City Commissioners. 13 Annual Reports Neighborhood Planning Assemblies . 15 Burlington Housing Authority . 72 Regularly Scheduled Chittenden Solid Waste District . 73 Commission Meetings . 16 Green Mountain Transit . 75 Justices of the Peace . 17 Winooski Valley Park District . 77 Department Annual Reports Miscellaneous Airport, Burlington International . 18 Annual Town Meeting . 79 Arts, Burlington City . 20 Salaries. 81 Assessor, Office of the City . 23 General Obligation Debt. 100 Attorney, Office of the City . 24 Appraised Valuation. 100 Church Street Marketplace. 27 Tax Exempt Property Summary. 100 Clerk/Treasurer, Office of the City . 29 Management Letter . 101 Code Enforcement . 31 Audit Summary . 106 Community & Economic Development Office . 32 ACKNOWLEDGMENTS Design/Production: Futura Design Printing: Queen City Printers Inc. Printed on PC Recycled Paper Cover Photo: Courtesy of Andrew Krebs Project Management: Liz Amler, Mayor’s Office This report also is available online at www.burlingtonvt.gov. Thanks to the Department of Parks, Recreation & Waterfront for the use of photos throughout this report. This publication was printed on 100% PC Recycled FSC® certified paper. -

FY2013 Annual Impact Report
Annual ReportFY 2013 Independence, inclusion, dignity, and advocacy. www.howardcenter.org 802.488.6900 HowardCenter offers life-saving professional crisis and counseling services to children and adults; supportive services to individuals with autism and intellectual disabilities who need help with education, employment, and life maintenance skills; counseling and medical services for those struggling with substance abuse, and intensive interventions for adults with serious and persistent mental health challenges. Our mission: HowardCenter improves the well-being of children, adults, families, and communities. Board of Trustees Honorary Board Senior Leadership as of June 30, 2013 Jack Dwyer Todd M. Centybear Mark Baglini William Heaslip Executive Director President E. William Leckerling A publication of Susan Cain O’Brien Bob Bick HowardCenter Elizabeth Bassett George Philibert Director, Mental Health Martie Majoros, editor Vice President Tony Villanti and Substance Abuse 208 Flynn Avenue #3J Services Burlington, VT 05401 Matthew Frazee, CPA 802.488.6900 Treasurer Lorraine Jenne Director, Operations Marna Tulin, PhD Secretary Sandra McGuire We’ve done our best to Chief Financial Officer acknowledge all of our FY13 Rick Blount donors and volunteers. If Katherine Connolly Deborah Shenk we’ve missed you, please call Gillian Eaton Director, Development (802) 488-6912 so we can Kevin Endres and Communications update our records. Sen. Sally Fox Susan Hillman Catherine Simonson Michael Lipson Director, Child, Youth and Peter McCarthy Family Services Stacey Miller, EdD Karen O’Neill Sandra Steingard, MD Duane Peterson Medical Director Michael Simoneau David Sobczak Marie Zura Connie Stabler Director, Developmental Debra Stenner Services Cover photo: HowardCenter’s Gail Stevenson, PhD First Call Staff. -

Annual Report / Fy 2014
ANNUAL REPORT / FY 2014 A publication of Howard Center Martie Majoros, editor 208 Flynn Avenue #3J, Burlington, VT 05401 LETTER TO THE COMMUNITY OUR MISSION Throughout my time at Howard Center, I have been fortunate to have had the Howard Center improves the well-being of opportunity to thank many of you in person for your support and words of wisdom. As I near the end of my 39-year tenure, I want to once again express my gratitude on children, adults, families, and communities. behalf of the individuals and families we serve each year. It has been a bit selfish on my part: I have gained more than given, learned more than taught. In the faces I’ve seen over the years, I’ve witnessed the strength and courage required BOARD OF TRUSTEES AS OF JUNE 30, 2014 SENIOR LEADERSHIP AS OF JUNE 30, 2014 to deal with life’s challenges. I’ve watched as people who could easily choose to complain about unfairness strive to make each day a positive one for themselves, Mark Baglini Todd M. Centybear President Executive Director their family and friends, and even strangers. And because of your generosity and commitment to our mission, I’ve seen faces filled with courage, hope, and joy. Elizabeth Bassett Bob Bick Vice President Director, Mental Health and You have made possible many services which benefit children, adults, and families. Substance Abuse Services Although highlighting specific programs is a bit like trying to choose a favorite child, Matthew Frazee, CPA we have much to celebrate. We have created two highly acclaimed programs that offer Treasurer Lorraine Jenne support for individuals with autism; one for pre-school children, the other for college- Director, Operations age students. -

COTS Is on the Move!
THE COMMITTEE ON TEMPORARY SHELTER VOL. 34, NO. 1 www.cotsonline.org SPRING 2016 “Know” pressure COTS is on the move! UVM meDical stuDents Winter was busy with new projects, programs proviDE heart-healthy proGram at the Daystation We’ve moved! COTS has temporarily located our programs and administrative offices to 179 S. Winooski Ave., Burlington. We will be in this new location Partnerships are key to COTS ability to until early 2017. Our phone numbers, emails, post office box remain meet the diverse needs of those who are unchanged. homeless or at risk of homelessness. We have been fortunate to work with many We have moved out of our main facility in order for the renovations and businesses and organizations to serve construction to get under way at 95 North Avenue. COTS is “ bringing it homeless people in our community. all home” with this project: We are rebuilding a permanent home for our One such partner is the University of Daystation program, creating 14 new permanent apartments, improving Vermont College of Medicine. For the program space for our housing prevention program (Housing Resource past several years, the second-year Center) and family services, and making our building more energy-efficient medical students at UVM have created and ADA accessible. unique annual programs to address This project was made possible by the support of our generous community, needs among the homeless population our successful capital campaign, and our partnership with Housing Vermont. in our community. One year, it was “Happy Feet,” addressing podiatric Our building at 95 North Avenue is now an official “hard hat” only area! We concerns; another it was “VFW – for look forward to bringing you updates on the progress of the project as well as Veterans’ Fitness & Wellness,” focusing the homelessness prevention and housing programs it will make possible. -

FY2016 Annual Impact Report
ANNUAL IMPACT REPORT FY 2016 SINCE 1865 Introducing our new First Call for Chittenden County Team PLUS 2016 CALENDAR YEAR HIGHLIGHTS Our Mission Board Senior Howard Center improves the of Trustees Leadership well-being of children, adults, as of June 30, 2016 as of June 30, 2016 families, and communities. Gail Stevenson, Ph.D., President Bob Bick Connie Stabler, Vice President Chief Executive Officer Matthew Frazee, CPA, Treasurer Sandy McGuire Kathy Connolly, Secretary Our History Chief Financial and Operations Officer Howard Center has a long and rich history as a trusted provider in our community. With Patrick Brown Catherine Simonson a legacy spanning 150 years, Howard Center Daniel Calder Chief Client Services Officer Thomas J. (TJ) Donovan, Jr. has been leading the charge for progressive, Sandra Steingard, M.D. Gillian Eaton compassionate, high quality care and treatment Chief Medical Officer for those members of our community in Kerrick Johnson need. Founded in 1865 as an agency serving Michael Kupersmith 2 the children of the destitute, it now offers E. William Leckerling life-saving professional crisis and counseling Pam Mackenzie services to children and adults; therapeutic Meg O’Donnell George Philibert A publication of the Howard Center Development and interventions and education programs for Communications Office, Martie Majoros, editor. children with emotional and behavioral Rep. Ann Pugh 208 Flynn Avenue #3J, Burlington, VT 05401 issues; supportive services to individuals Michael Simoneau Lusenge Emmanuel Siriwayo We’ve done our best to acknowledge all of our FY16 (July 1, with autism and intellectual disabilities who 2015–June 30, 2016) donors, volunteers, and community need help with education, employment, and David Sobczak partners. -
Addressing Global Climate Change Locally
AddressingAddressing GlobalGlobal ClimateClimate ChangeChange LocallyLocally Vermont Case Studies for Clean Energy for Towns and Schools: Safe Money and Go Green Cape & Islands Renewable Energy Collaborative and Waquoit Bay National Estuarine Research Reserve May 18, 2007 Debra L. Sachs, Alliance for Climate Action Today’s Remarks . • Introduction and brief background • Economic development and energy efficiency advocates can foster opportunities • Vermont Energy & Climate Action Network- structure/role of energy committees • Communities--planning, implementing strategies • Ideas, lessons learned in leadership AllianceAlliance forfor ClimateClimate ActionAction MembersMembers City of Burlington Vermont Department of Public Service Underground Railway Theater--Vermont Vermont Interfaith Power & Light OurOur VisionVision • To support the reduction of greenhouse gas emissions by at least 10 percent; • To inspire, facilitate and motivate behavior change; • To monitor community progress; and • To collaborate with others to expand efforts throughout Vermont and beyond. ClimateClimate ActionAction PlanPlan Keep the vision consistent… The Climate Action Plan A Plan to Save Energy and Reduce Greenhouse Gas Emissions • Municipal Development Plan • Climate Action Plan • Legacy Plan Burlington Climate Protection Task Force Burlington, Vermont, USA March 2000 Adopted by Burlington City Council--May 1, 2000 IndividualIndividual actionsactions toto growinggrowing partnershipspartnerships…… • 10% Challenge Program …voluntary program encouraging households, -
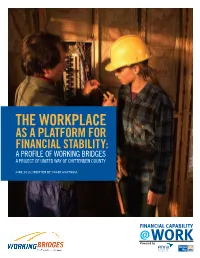
The Workplace As a Platform for Financial Stability: a Profile of Working Bridges a Project of United Way of Chittenden County
THE WORKPLACE AS A PLATFORM FOR FINANCIAL STABILITY: A PROFILE OF WORKING BRIDGES A PROJECT OF UNITED WAY OF CHITTENDEN COUNTY JUNE 2015 | WRITTEN BY: INGER GIUFFRIDA ACKNOWLEDGEMENTS The Workplace as a Platform for Financial Stability: A Profile of Working Bridges was researched and writ- ten by Inger Giuffrida, financial educator and asset building consultant. Since 2009, Ms. Giuffrida has provided training and technical assistance to grantees of the FINRA Investor Education Foundation and United Way Worldwide’s Financial Education in Your Community grant program. She may be contacted at [email protected]. The author would like to thank Lisa Falcone, Working Bridges Project Director, and Lisa Jensen, Working Bridges Resource Coordinator, for their invaluable insights and contributions to this profile. The author would also like to thank Ted Castle, President and CEO of Rhino Foods, Inc.; Gina Catanzarita, Director of Human Resources, Engelberth Construction; and Adam Leonard, Director of Human Resources, Sheraton Hotel and Conference Center, Burlington, Vermont. FINANCIAL CAPABILITY@WORK The FINRA Investor Education Foundation and United Way Worldwide’s Financial Capability@Work project is an effort to build on the success of community-based efforts to deliver financial education and related ser- vices in the workplace and help similar community-based organizations design, implement, and evaluate the impact of workplace financial capability initiatives tailored to meet the needs of their own local communities. FINRA INVESTOR EDUCATION FOUNDATION The FINRA Investor Education Foundation supports innovative research and educational projects that give underserved Americans the knowledge, skills and tools necessary for financial success throughout life. For details about grant programs and other FINRA Foundation initiatives, visit www.finrafoundation.org. -
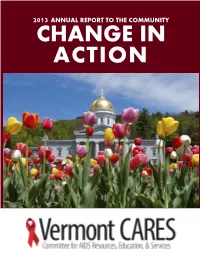
2013 Annual Report to the Community Change in Action
2013 ANNUAL REPORT TO THE COMMUNITY CHANGE IN ACTION From the Executive Director Dear Friends and Supporters, I am so proud to share with you Vermont CARES’ results from the last year, which saw us serving thousands of Vermonters affected by HIV/AIDS through a mix of volunteers, staff, and long-term supporters. In an era when our clients’ needs continue to increase, it has been so critically important to have an organization like Vermont CARES offering HIV testing, expanded HIV prevention, HIV medical support, and AIDS housing. In the last year, thanks to your support and contributions, we have been able to : House, feed, and support the medical costs of over 170 In the last year we Vermonters living with HIV or AIDS—this is roughly one in have been able to three of our neighbors with the virus. house, feed, and Offer over 500 rapid-result HIV tests free of charge to help people learn if they have HIV and, if so, to segue them directly support the medical into medical care to keep them healthier—and happier—longer. costs of 1 in 3 of our Expand our syringe exchange program to reach even more people who use injection drugs and need access to sterile neighbors with HIV. injection equipment in order to avoid HIV or Hepatitis C infection. We’ve leveraged a new $5,000 grant to be able to serve 50 new participants in the southern part of our service area. Educate over 2,400 Vermonters at risk of HIV through presentations in schools, social clubs, civic organizations, employers, or substance abuse treatment centers. -

2023 Consolidated Plan for Housing & Community Development One
2018- 2023 Consolidated Plan for Housing & Community Development One Year Action Plan City of Burlington, Vermont Prepared by Community & Economic Development Office Room 32 – City Hall 149 Church Street Burlington, VT 05401 802-865-7144 www.burlingtonvt.gov/CEDO This document is available upon request in alternative format for persons with disabilities. Consolidated Plan BURLINGTON NA 1 OMB Control No: 2506-0117 (exp. 06/30/2018) Executive Summary ES-05 Executive Summary The City is required to have a Consolidated Plan for Housing & Community Development in order to receive funding under two federal programs: the Community Development Block Grant (CDBG) and HOME Investment Partnership Act (HOME) programs. The CDBG program grows local economies and improves the quality of lives for low- and moderate-income residents. The HOME program is designed to create affordable housing for low-income households through building, buying, and/or rehabilitating housing for rent or homeownership. The U.S. Department of Housing & Urban Development (HUD) provides direct grants to over 1,200 state and local governments, called entitlement communities, including the City of Burlington, on a formula basis each year. The City, in turn, awards grants and loans to local nonprofits and also provides direct services to residents and businesses through several CDBG-funded programs. In 2018, the City will receive $786,789 in CDBG funding and $539,670 in HOME funding. The Consolidated Plan provides detailed information about city demographics, the local housing market and the local economy. It outlines housing, community and economic development needs and priorities for the City. This Consolidated Plan covers the five-year period beginning in July 2018.