Licensed Hospitals Updated 7-16-2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2016 Recognition Targets for Hospitals
Patient Safety Reporting Program 2016 Recognition Targets for Hospitals March 2016 Recognition targets provide attainable goals for healthcare facilities participating in the Patient Safety Reporting Program (PSRP). Targets can also help facilities incrementally and effectively build adverse event review and reporting into their culture of safety. On a statewide level, targets ensure OPSC receives enough adverse event reports to build a strong database of prevention strategies so that all Oregon healthcare facilities can learn from one another. Targets are effective as of January 1, 2016. Although a participant may meet or exceed targets at any time throughout the year, the facility should continue to report adverse events according to reporting program guidelines. Healthcare facilities that meet targets are recognized annually for their transparency efforts and commitment to patient safety. For more information, visit oregonpatientsafety.org. Meet Targets Exceed Targets Quantity The number of reports submitted by a participating Submit at least the Submit at least the facility minimum quantity minimum quantity target for target for Goal: Help ensure PSRP obtains enough reports to your facility your facility build a strong database for learning. (see page 2) (see page 2) Acceptable Quality The report identifies contributing factors, root Submit at least 2 Submit 75% of causes, and system-level action plans reports that are reports with acceptable quality acceptable quality Goal: Provide enough information so that your experience can help others learn and improve. See the Guide to Quality Reporting Timeliness The amount of time that passes between discovery Submit 50% of reports of an adverse event and when a report is submitted within 45 days of to PSRP event discovery Goal: Respond immediately after an adverse event to collect full and reliable information, reduce delays, and develop strong solutions. -
Weekly Report
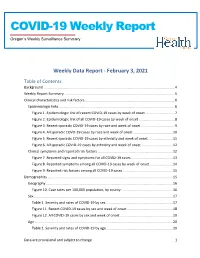
COVID-19 Weekly Report Oregon’s Weekly Surveillance Summary Novel Coronavirus (COVID-19) Weekly Data Report - February 3, 2021 Table of Contents Background ........................................................................................................................................... 4 Weekly Report Summary ..................................................................................................................... 5 Clinical characteristics and risk factors ............................................................................................... 6 Epidemiologic links ........................................................................................................................... 6 Figure 1. Epidemiologic link of recent COVID-19 cases by week of onset ............................... 7 Figure 2. Epidemiologic link of all COVID-19 cases by week of onset ...................................... 8 Figure 3. Recent sporadic COVID-19 cases by race and week of onset .................................... 9 Figure 4. All sporadic COVD-19 cases by race and week of onset .......................................... 10 Figure 5. Recent sporadic COVID-19 cases by ethnicity and week of onset .......................... 11 Figure 6. All sporadic COVID-19 cases by ethnicity and week of onset .................................. 12 Clinical symptoms and reported risk factors ................................................................................ 12 Figure 7. Reported signs and symptoms for all COVID-19 cases ........................................... -

Nutrition Practice Care Guidelines for Preterm Infants in the Community 2013 Revision
Nutrition Practice Care Guidelines for Preterm Infants in the Community 2013 Revision Oregon Appendix Oregon Appendix to the Nutrition Practice Care Guidelines for Preterm Infants in the Community, 2013 Revision Providing optimal care for premature infants in the community and their families requires care coordination. Care coordination takes an understanding of what services are available in the community and how to qualify and access these services. The purpose of the Oregon appendix is to connect health care providers, advocates and families with contact names of individuals and organizations. Change is constant. We recognize that information is likely to change as soon as the document is published. But it is a start and we hope it is a useful and dynamic resource. Please submit suggestions for additions, changes to the attention of the Oregon Pediatric Nutrition Practice Group at [email protected] Appendix contents: • Developmental, Feeding and NICU Follow-up clinics and Level III Neonatal Intensive Care Units in Oregon and Southwest Washington • Lactation Clinics and Equipment Rentals in Oregon and Southwest Washington • Oregon Public Health Nurse Services • Oregon Health Department Contact Information • Oregon Nurse-Family Partnership • Oregon WIC Local Agency Contact List • Northwest Mothers Milk Bank Donor Drop-off Sites Developmental, Feeding and NICU Follow-up Clinics and Level III Neonatal Intensive Care Units in Oregon and Southwest Washington City, Medical Center Clinic Phone Specialists Oregon Number Bend St. Charles Medical -

Trauma Surge Plan-HPO Compress Part 1
Oregon Healthcare Preparedness Region 1 Trauma Surge Plan TRAUMA SURGE PLAN: CORE PLANNING GROUP About Us Our Mission: To assist hospitals, hospital staff, and first responders in preparing for events which overwhelm the region’s trauma system through education and the provision of resources. The outcome is the safe management and care of the critically injured, and enhancement of a seamless transition of care. Who we are: A collaborative team of experts representing the region's emergency preparedness, first responder, and trauma center leadership. Core Planning Group Members: Tanya Shanks-Connors, Legacy Health Roy Ball, Legacy Health Angela Heckathorn, Legacy Health Mark Dollar, Legacy Health Kathryn Richer, NW Oregon Health Preparedness Organization Jonathan Jui, Multnomah County Emergency Medical Services Sherrie Forsloff, Oregon Health & Science University Mercedes Wilson, Oregon Health & Science University Acknowledgements This was truly a multi-discipline, multi-agency, multi-jurisdiction, and multi-year effort. Its success is due to our many partners in contributing agencies, as well as funders. We express our deep gratitude to the following for their support: o Clackamas County Emergency Management o Legacy Health o Multnomah County Emergency Management o Multnomah County Emergency Medical Services o NW Oregon Health Preparedness Organization o Oregon Health Authority o Oregon Health Science & University o Regional Disaster Preparedness Organization o U.S Department of Health and Human Services o Washington County Emergency Management For further information, or to contact a member of the Core Planning Group please go to our Hospital Emergency Preparedness website at: hospitalemergencypreparedness.org Oregon Healthcare Preparedness Region 1 | Trauma Surge Plan 1 | P a g e Table of Contents Introduction ................................................................................................................................................. -

Oregon COVID-19 Weekly Report
Informe semanal de COVID-19 Resumen de vigilancia semanal de Oregón Nuevo coronavirus (COVID-19) División de Salud Pública de Oregón Publicado el 9 de diciembre de 2020 Antecedentes Los datos del Informe semanal de COVID-19 se concluirán todos los domingos a las 11 p. m., hora de verano del Pacífico, y el informe se publicará el miércoles. Tenga en cuenta que los datos informados aquí se están actualizando continuamente. Para obtener información actualizada a diario, visite el sitio web sobre COVID-19 de la Autoridad de Salud de Oregón (Oregon Health Authority, OHA): https://govstatus.egov.com/OR-OHA-COVID-19. Hasta las 11 p. m. del domingo, 6 de diciembre, hubo 85,788 casos de COVID-19 informados a la Autoridad de Salud de Oregón. De estos, 3,741 (4.4 %) son casos “presuntos”, digamos personas que tienen síntomas compatibles con COVID-19 y contacto cercano con un caso confirmado, pero no tuvieron una prueba de laboratorio que lo confirme. Aunque no están confirmados, los casos presuntos muy probablemente tengan COVID-19, debido a los síntomas específicos y a la exposición conocida. Se les recomienda a los casos presuntos que se realicen pruebas de detección para confirmar si tienen COVID-19. Los casos presuntos que obtengan un resultado positivo se recategorizan a casos confirmados. Estos datos representan una visión global de los factores de riesgo de COVID-19, características clínicas y demográficas de los casos e incluyen datos sobre casos con exámenes complementarios pendientes. No se ha entrevistado a todos los casos al momento del presente informe. -

Impact of Policies on Rural Communities Oregon
Impact of Policies on Rural Communities Oregon Sequestration2 Bad Debt Reimbursement Cut3 2% Inpatient and Outpatient Medicare Revenue Cut 35% Medicare Bad Debt Reimburesment Cut Provider Operating Annual Potential Job Potential GDP Annual Potential Job Potential GDP Provider Name/Number 1 Type Margin 1 Revenue Lost 1 Loss 4 Loss 5 Revenue Lost Loss 4 Loss 5 Bay Area Hospital (380090) RPPS 5.1% $1,402,674 21 $2,694,287 $335,951 5 $645,302 Blue Mountain Hospital (381305) CAH 12.4% $103,038 2 $230,097 $22,265 0 $49,721 CHI St. Anthony Hospital (381319) CAH 14.1% $295,649 4 $570,912 $62,980 1 $121,616 Columbia Memorial Hospital (381320) CAH 13.3% $536,031 9 $1,188,408 $312,917 5 $693,753 Coquille Valley Hospital (381312) CAH -1.0% $221,858 3 $409,956 $18,291 0 $33,799 Curry General Hospital (381322) CAH -0.2% $285,231 5 $630,182 $100,353 2 $221,718 Good Shepherd Health Care System (381325) CAH 4.5% $425,575 7 $923,659 $62,123 1 $134,829 Grande Ronde Hospital (381321) CAH 3.6% $445,021 7 $879,693 $167,414 3 $330,936 Harney District Hospital (381307) CAH -1.8% $103,560 2 $240,129 $17,862 0 $41,417 Lake District Hospital (381309) CAH 0.3% $120,338 3 $338,664 $11,533 0 $32,456 Lower Umpqua Hospital District (381311) CAH -5.8% $121,920 2 $285,842 $68,875 1 $161,478 Mercy Medical Center (380027) RPPS 16.5% $1,187,722 20 $2,610,228 $101,817 2 $223,760 Mid-Columbia Medical Center (380001) RPPS 3.2% $477,045 9 $1,109,291 $139,303 3 $323,927 PeaceHealth Cottage Grove Community Medical Center CAH 19.4% $237,056 4 $483,247 $87,272 1 $177,907 (381301) 1 CMS Healthcare Cost Report Information System (HCRIS) Q1 2020. -

Beacon Name Changing to Affinity
September 30, 2016 Dear Provider, A few months ago we sent you some information and an attestation of acknowledgement that the Beacon network name will be changing to the Affinity network for the 2017 plan year. With 2017 open enrollment beginning in November, we want to make sure you are aware of changes to Moda’s Beacon Network, which is available to individuals purchasing health coverage directly from Moda or through the federal marketplace exchange. For plans effective January 1, 2017, the Beacon Network name in your area will change to the Affinity Network. The Beacon Network will continue to serve members in select Western Oregon counties. The Affinity Network will be available to individual members residing in the following counties: Baker Morrow Gilliam Sherman Grant Umatilla Harney Union Lake Wallowa Malheur Wheeler Affinity is designed to ensure members find the care they need, when they need it, Affinity helps members looking for customized care that fits their individual lifestyle and budget, and find the care they need, when they need it. With Affinity, members have access to a large selection of providers including Blue Mountain Hospital District, Good Shepherd, Grande Ronde Hospital, Harney District Hospital, Lake District Hospital, Pioneer Memorial Hospital (Heppner), St. Alphonsus Baker City, St. Alphonsus Ontario, and Wallowa Memorial Hospital. Although the Affinity name is new, we don’t expect any changes to your current workflow. Reimbursement, referrals to in-network providers, prior authorizations and processes will be the same. Individuals choosing plans supported by the Affinity network will be asked to select a primary care physician (PCP) to coordinate care. -
Seeking Asylum: Race, Memory, and the American Landscape
ABSTRACT Title of Thesis: SEEKING ASYLUM: RACE, MEMORY, AND THE AMERICAN LANDSCAPE Daniela Tai, Dual Master’s Degree in Architecture and Historic Preservation, 2019 Thesis Directed By: Professor, Ronit Eisenbach, School of Architecture, Planning & Preservation The stories and places we choose to preserve tell us who we are as a people. What does it say about ourselves when the stories that are associated with a particular place are ones that we wish to keep in the dark? As we look towards the future of preservation it has become clear that our perception of what is “significant” has shifted. Modern preservation has expanded to include tangible and intangible landscapes, environmental conservation, and more voices at the table. This thesis explores how to use preservation, storytelling, and sustainable practices to respond to places of difficult history and reclaim that space, while using Crownsville State Hospital as a model. The racial and systemic trauma experienced at the formerly racially segregated mental health facility permeated the campus grounds; not only does the community need to heal, the land does too. SEEKING ASYLUM: RACE, MEMORY, AND THE AMERICAN LANDSCAPE by Daniela Tai Thesis submitted to the Faculty of the Graduate School of the University of Maryland, College Park, in partial fulfillment of the requirements for the degree of Dual Master’s Degree in Architecture and Historic Preservation 2019 Advisory Committee: Professor Ronit Eisenbach, Chair Dr. Donald W. Linebaugh, Interim Dean Professor Emeritus Karl F.G. Du Puy, AIA © Copyright by Daniela Tai 2019 Preface Opened in 1911 as the Hospital for the Negro Insane of Maryland, Crownsville State Hospital stands at a crossroads in American history; on one side stands the triumphs of medical progress and on the other stands the racial injustice and community trauma that made that progress possible. -

City of Salem Natural Hazards Mitigation Plan
City of Salem Natural Hazards Mitigation Plan Photo Credits Gary Halvorson, Oregon State Archives September 2017 Volume I: Basic Plan Prepared for: City of Salem Emergency Management June 2015 Final Report Prepared by: University of Oregon Community Service Center Oregon Partnership for Disaster Resilience June 2015 Final Report June 2015 Final Report June 2015 Final Report This Natural Hazard Mitigation Plan was prepared by: With support from: Planning grant funding provided by: Federal Emergency Management Agency (FEMA) Pre-Disaster Mitigation Program Grant: EMS-2014-PC-0011 Sub-grant Application Reference: PDMC-PL-10-OR-2014-002 Additional Support Provided by: This material is a result of tax-supported research and, as such, is not copyrightable. It may be freely reprinted with the customary crediting of the source. SPECIAL THANKS & ACKNOWLEDGEMENTS City of Salem developed this Natural Hazards Mitigation Plan (NHMP) through a regional partnership funded by the Federal Emergency Management Agency’s (FEMA) Pre-Disaster Mitigation (PDM) Competitive Grant Program: EMS-2014-PC-0011, Sub-grant Application Reference: PDMC-PL-10-OR-2014-002. The city utilized a four-phased planning process, plan templates and plan development support provided by the Oregon Partnership for Disaster Resilience (OPDR) at the University of Oregon’s Community Service Center. Special thanks to Roger Stevenson, City of Salem Emergency Manager for his leadership in convening the committee. City of Salem NHMP Update Steering Committee • Convener, Roger Stevenson, City -
Treat Or Repeat
Treat or Repeat A State Survey of Serious Mental Illness, Major Crimes and Community Treatment September 2017 TreatmentAdvocacyCenter.org/treat-or-repeat The gatekeepers of the chronically mentally ill must recognize that a failure to assess not just the rights of the mentally ill persons, but also their ability to achieve a minimum standard of acceptable behavior in the community will further erode public confidence in the professionals who govern patient care. … When the personal freedom of the mentally ill is given priority over all other considerations, the tyranny of some will jeopardize the autonomy of all. — Gary Maier, M.D., 1989 “The Tyranny of Irresponsible Freedom” Hospital and Community Psychiatry, 40, 453 Treat or Repeat A STATE SURVEY OF SERIOUS MENTAL ILLNESS, MAJOR CRIMES AND COMMUNITY TREATMENT E. Fuller Torrey, M.D. Founder Treatment Advocacy Center Lisa Dailey, J.D. Legislative and Policy Counsel Treatment Advocacy Center H. Richard Lamb, M.D. Emeritus Professor of Psychiatry and Behavioral Sciences Keck School of Medicine of the University of Southern California Elizabeth Sinclair, M.P.H. Research Associate Treatment Advocacy Center John Snook, J.D. Executive Director Treatment Advocacy Center Online at TreatmentAdvocacyCenter.org/treat-or-repeat © 2017 Treatment Advocacy Center Arlington, Virginia TREAT OR REPEAT n TABLE OF CONTENTS Executive Summary ................................................................................................................. 1 Introduction .......................................................................................................................... -

Antimicrobial Stewardship Initiative's Hospital Collaborative
Antimicrobial Stewardship Initiative’s Hospital Collaborative In 2012, the Oregon Patient Safety Commission and the Oregon Health Authority created the Oregon Antimicrobial Initiative with funding from the Oregon Department of Justice. This initiative included support for improved outpatient antimicrobial use through the Alliance Working for Antibiotic Resistance Education, a survey of Oregon hospitals’ current stewardship practices, one-day trainings for interested hospitals, and a 12-month quality improvement collaborative for hospitals ready to commit the time and energy required. Collaborative Dates Collaborative Participants November 2012 to November 2013 Columbia Memorial Hospital Collaborative Structure Doernbecher Children’s Hospital Lake District Hospital The Collaborative included learning sessions for all participants to learn best Mid-Columbia Medical Center practices together and share strategies with each other, conference calls and Randall Children’s Hospital webinars to provide additional content and help participants remain Rogue Regional Medical Center connected between meetings, and site visits to provide expert consultation to Sacred Heart Medical Center teams and leaders while ensuring continued progress. From November to Salem Hospital March, collaborative staff worked with hospitals to prepare for Salmon Creek Medical Center implementation of activities. Hospitals began formal implementation of Samaritan Albany Hospital antimicrobial stewardship activities in mid-March 2013. Samaritan North Lincoln Hospital -
FY 2020 Proposed Rule Impact File.Xlsx
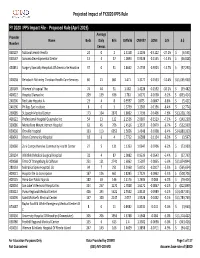
Projected Impact of FY2020 IPPS Rule FY 2020 IPPS Impact File ‐ Proposed Rule (April 2019) Average Provider Name Beds Daily Bills CMIV36 CMIV37 ∆CMI ∆ % ∆ $ Number Census 060107 National Jewish Health 24 0 2 1.5158 1.1036 ‐0.4122 ‐27.2%$ (6,595) 050547 Sonoma Developmental Center 13 4 37 1.0893 0.9338 ‐0.1555 ‐14.3% $ (46,028) 450831 Surgery Specialty Hospitals Of America Se Houston 37 0 31 2.8662 2.4739 ‐0.3923 ‐13.7%$ (97,290) 320038 Rehoboth Mckinley Christian Health Care Services 60 21 861 1.471 1.3177 ‐0.1533 ‐10.4%$ (1,055,930) 150149 Women's Hospital The 74 44 31 1.582 1.4228 ‐0.1592 ‐10.1%$ (39,482) 400022 Hospital Damas Inc 209 139 636 1.781 1.6172 ‐0.1638 ‐9.2%$ (833,414) 240206 Red Lake Hospital A 23 4 8 0.9597 0.875 ‐0.0847 ‐8.8%$ (5,421) 240196 Phillips Eye Institute 8 0 3 1.3739 1.2583 ‐0.1156 ‐8.4%$ (2,774) 260085 St Joseph Medical Center 173 104 2870 1.8602 1.7196 ‐0.1406 ‐7.6%$ (3,228,176) 400122 Professional Hospital Guaynabo Inc 54 13 122 2.1536 2.0007 ‐0.1529 ‐7.1%$ (149,230) 330086 Montefiore Mount Vernon Hospital 63 45 706 1.4516 1.3537 ‐0.0979 ‐6.7%$ (552,939) 050030 Oroville Hospital 133 113 6052 1.5656 1.4648 ‐0.1008 ‐6.4%$ (4,880,333) 460043 Orem Community Hospital 18 6 4 1.7712 1.6588 ‐0.1124 ‐6.3%$ (3,597) 320060 Zuni Comprehensive Community Health Center 27 5 131 1.1353 1.0647 ‐0.0706 ‐6.2%$ (73,989) 250134 Whitfield Medical Surgical Hospital 32 4 87 1.0082 0.9539 ‐0.0543 ‐5.4%$ (37,793) 420068 Trmc Of Orangeburg & Calhoun 251 121 2741 1.6062 1.5207 ‐0.0855 ‐5.3%$ (1,874,844) 280133 Nebraska Spine Hospital,