New York Obstetrics & Gynecology, P.C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report Measures the State of Parks in Brooklyn
P a g e | 1 Table of Contents Introduction Page 2 Methodology Page 2 Park Breakdown Page 5 Multiple/No Community District Jurisdictions Page 5 Brooklyn Community District 1 Page 6 Brooklyn Community District 2 Page 12 Brooklyn Community District 3 Page 18 Brooklyn Community District 4 Page 23 Brooklyn Community District 5 Page 26 Brooklyn Community District 6 Page 30 Brooklyn Community District 7 Page 34 Brooklyn Community District 8 Page 36 Brooklyn Community District 9 Page 38 Brooklyn Community District 10 Page 39 Brooklyn Community District 11 Page 42 Brooklyn Community District 12 Page 43 Brooklyn Community District 13 Page 45 Brooklyn Community District 14 Page 49 Brooklyn Community District 15 Page 50 Brooklyn Community District 16 Page 53 Brooklyn Community District 17 Page 57 Brooklyn Community District 18 Page 59 Assessment Outcomes Page 62 Summary Recommendations Page 63 Appendix 1: Survey Questions Page 64 P a g e | 2 Introduction There are 877 parks in Brooklyn, of varying sizes and amenities. This report measures the state of parks in Brooklyn. There are many different kinds of parks — active, passive, and pocket — and this report focuses on active parks that have a mix of amenities and uses. It is important for Brooklynites to have a pleasant park in their neighborhood to enjoy open space, meet their neighbors, play, and relax. While park equity is integral to creating One Brooklyn — a place where all residents can enjoy outdoor recreation and relaxation — fulfilling the vision of community parks first depends on measuring our current state of parks. This report will be used as a tool to guide my parks capital allocations and recommendations to the New York City Department of Parks and Recreation (NYC Parks), as well as to identify recommendations to improve advocacy for parks at the community and grassroots level in order to improve neighborhoods across the borough. -

The New York City Waterfalls
THE NEW YORK CITY WATERFALLS GUIDE FOR CHILDREN AND ADULTS WELCOME PLAnnING YOUR TRIP The New York City Waterfalls are sited in four locations, and can be viewed from many places. They provide different experiences at each site, and the artist hopes you will visit all of the Waterfalls and see the various parts of New York City they have temporarily become part of. You can get closest to the Welcome to THE NEW YORK CIty WATERFALLS! Waterfalls at Empire-Fulton Ferry State Park in DUMBO; along the Manhattan Waterfront Greenway, north of the Manhattan Bridge; along the Brooklyn The New York City Waterfalls is a work of public art comprised of four Heights Promenade; at Governors Island; and by boat in the New York Harbor. man-made waterfalls in the New York Harbor. Presented by Public Art Fund in collaboration with the City of New York, they are situated along A great place to go with a large group is Empire-Fulton Ferry State Park in Brooklyn, which is comprised of 12 acres of green space, a playground, the shorelines of Lower Manhattan, Brooklyn and Governors Island. picnic benches, as well as great views of The New York City Waterfalls. These Waterfalls range from 90 to 120-feet tall and are on view from Please see the map on page 18 for other locations. June 26 through October 13, 2008. They operate seven days a week, You can listen to comments by the artist about the Waterfalls before your from 7 am to 10 pm, except on Tuesdays and Thursdays, when the visit at www.nycwaterfalls.org (in the podcast section), or during your visit hours are 9 am to 10 pm. -
Public Design Commission Conceptual Presentation on Open
PUBLIC DESIGN COMMISSION FINAL REVIEW JANUARY 19, 2021 WILLOUGHBY SQUARE OPEN SPACE NEW YORK CITY ECONOMIC DEVELOPMENT CORPORATION HARGREAVES JONES LANDSCAPE ARCHITECTURE GARRISON ARCHITECTS // DELTA FOUNTAINS // TILLETT LIGHTING LANGAN // WESLER-COHEN ASSOCIATES // PAUL COWIE & ASSOCIATES // CRAUL LAND SCIENTIST NORTHERN DESIGN // SITEWORKS // MILROSE CONSULTANTS THE ORATORY CHURCH OF ST 4 METROTECH CENTER DELI BONIFACE CHURCH (1ST FL) (JP MORGAN CHASE & CO) FLATBUSH AVENUE BROOKLYN BROOKLYN SAVANNA DEVELOPMENT (141 WILLOUGHBY STREET) Manhattan New Jersey WILLOUGHBY WILLOUGHBY STREET SQUARE Brooklyn AVA DOBRO Staten Island BROOKLYN POINT MIXED USE - RESIDENTIAL/COMMERCIAL BRIDGE STREET DUFFIELD STREET ALOT WILLOUGHBY FLATBUSH AVENUE GOLD STREET / ALBEE SQUARE (W HOTELS) SQUARE CITY NTS East Brooklyn SHERATON Bridge BROOKLYN River Park Cadman Navy Plaza Flatbush Ave Ext Yard Flushing Ave Clark St Cadman Plaza W Commodore Barry Park 227 DUFFIELD 230 DUFFIELD ST STREET Pierrepont St Brooklyn-Queens Expwy Tillary St (TOWNHOUSE) Johnson St HOTEL INDIGO CITY POINT (299 DUFFIELD STREET) (7 DEKALB AVENUE) Henry St Myrtle Ave Clinton St Ft Greene Gold St Duffield St Bridge St Willoughby St Park OFFERMAN Vanderbilt Ave ONE WILLOUGHBY SQUARE WILLOUGHBY Bklyn BUILDING MIXED USE - SCHOOL/OFFICE Fulton St Long Island Hospital SQUARE University Center Dekalb Ave Adams St Smith St BRIQ Hoyt St (237 DUFFIELD STREET) Bond St Atlantic St Nevins St THE AZURE (436 ALBEE SQUARE) Brooklyn-Queens Expwy NEIGHBORHOOD 1000’ SITE N RESIDENTIAL MIXED-USE SCALE: NTS -

Emergency Response Incidents
Emergency Response Incidents Incident Type Location Borough Utility-Water Main 136-17 72 Avenue Queens Structural-Sidewalk Collapse 927 Broadway Manhattan Utility-Other Manhattan Administration-Other Seagirt Blvd & Beach 9 Street Queens Law Enforcement-Other Brooklyn Utility-Water Main 2-17 54 Avenue Queens Fire-2nd Alarm 238 East 24 Street Manhattan Utility-Water Main 7th Avenue & West 27 Street Manhattan Fire-10-76 (Commercial High Rise Fire) 130 East 57 Street Manhattan Structural-Crane Brooklyn Fire-2nd Alarm 24 Charles Street Manhattan Fire-3rd Alarm 581 3 ave new york Structural-Collapse 55 Thompson St Manhattan Utility-Other Hylan Blvd & Arbutus Avenue Staten Island Fire-2nd Alarm 53-09 Beach Channel Drive Far Rockaway Fire-1st Alarm 151 West 100 Street Manhattan Fire-2nd Alarm 1747 West 6 Street Brooklyn Structural-Crane Brooklyn Structural-Crane 225 Park Avenue South Manhattan Utility-Gas Low Pressure Noble Avenue & Watson Avenue Bronx Page 1 of 478 09/30/2021 Emergency Response Incidents Creation Date Closed Date Latitude Longitude 01/16/2017 01:13:38 PM 40.71400364095638 -73.82998933154158 10/29/2016 12:13:31 PM 40.71442154062271 -74.00607638041981 11/22/2016 08:53:17 AM 11/14/2016 03:53:54 PM 40.71400364095638 -73.82998933154158 10/29/2016 05:35:28 PM 12/02/2016 04:40:13 PM 40.71400364095638 -73.82998933154158 11/25/2016 04:06:09 AM 40.71442154062271 -74.00607638041981 12/03/2016 04:17:30 AM 40.71442154062271 -74.00607638041981 11/26/2016 05:45:43 AM 11/18/2016 01:12:51 PM 12/14/2016 10:26:17 PM 40.71442154062271 -74.00607638041981 -

2015 City Council District Profiles
B RO O K LY N CITY COUNCIL MIDTOWN LONG SOUTH ISLAND CITY DISTRICT MURRAY 2015 CityHILL Council District Profiles W 28 ST SUNNYSIDE GARDENS CHELSEA E 33 ST HUNTERS QUEENS BLVD 33 POINT 49 AVE HUNTE T FLATIRON BO R S RDE S S L P N A L O T VE I IN S 3 K T E H A TC VE W M DU W 14 ST C G U BLISSVILLE I 46 ST N N PROVOST ST E GRAMERCY S S K IN 4 B N ST G FREEMA L S V L A VE D N A UNION GREEN ST N 5 D STUYVESANT E SQUARE HURON ST A W TOWN V INDIA ST E T O 26 W T AVE N EENPOIN WESTGreenpoint GR CR 19 EEK MASPETH GREENPOINT North Side AVE OAK ST NORMAN VE South Side AVE NEWEL ST A LE ECKFORD ST EAST RO SE MANHATTAN AVE AVE BUSHWIC ME NASSAU Williamsburg VILLAGE K INLET MEEKER R HOUSTON ST Clinton HillU SOHO 4 30 S E T C V A S E AVE T VE H DRIGGS Vinegar Hill A 6 T GREENWICH ST Y W Brooklyn Heights HUDSON RIVER 5 LITTLE ITALY 2 NORTH VE A Downtown Brooklyn SIDE 28 2 N 10 ST ORD VE BoerumD A Hill 1 BOWERY DF GRAN BE N 8 ST CHAMBERS ST CHINATOWN R N 3 ST D N 6 ST R D CIVIC F AN AVE BATTERY ETROPOLIT CENTER LOWER S 1 ST M PARK EAST SIDE EAST SOUTH CITY S 3 ST WILLIAMSBURG SIDE WILLIAMSBURG B L U E S H N W N A I FLUSHING AVE C H K C EAST RIVER NAVY A V T E YARD U O W B 16 A BASIN L Y L 23 C A 34 KO W HOOPER ST JOHN ST PENN ST FF A 1 27 LEE AVE VE WATER ST HEYWARD ST MIDDLETON ST 21 14 10 33 26 BUSHWICK 37 30 20 Navy Yard FRANKLIN 9 NOSTRAND 3 8 AVE BROADWAY BUSHWICK 11 FLUSHING AVE PARK 13 HICKS ST 25 HENRY ST BROOKLYN QUEENS EXPWY BEDFORD TLE AVE 15 A MYR BROOKLYN 24 VE 17 A HEIGHTS VE Legend JORALEMON ST A VE FULTON ST AVE GROVE ST 7 WILLOUGHBY ATLANTIC -

HER HERO Bye
INSIDE Including The Bensonhurst Paper New places to nosh Published weekly by Brooklyn Paper Publications, 26 Court St., Brooklyn, NY 11242 Phone 718-834-9350 AD fax 718-834-1713 • NEWS fax 718-834-9278 © 2003 Brooklyn Paper Publications • 16 pages including GO BROOKLYN • Vol.26, No. 26 BRZ–BENHURST • June 30, 2003 • FREE Tyson brawls Bye, bye in Brooklyn, HER HERO Grippo Woman honors cop who saved her life District super at again as 9-11 terror gripped the Trade Center last board meet By Patrick Gallahue By Deborah Kolben and Neil Sloane The Brooklyn Papers By Deborah Kolben with Associated Press reports The Brooklyn Papers A police officer and the Bay Ridge woman Former heavyweight champion Senior Superintendent Vincent Grippo said Mike Tyson was released from the she saved on the morning of Sept. 11, 2001, / Louis Lanzano goodbye to District 20 at the school board’s 84th Precinct Downtown were reunited at an awards ceremony at the 68th Precinct this week. farewell meeting on Monday night. Saturday afternoon, 11 hours Under the new changes to the city public schools after his arrest on assault charges Calling their reconnection a “miracle,” police of- ficer Alicia Regans was presented with an award the school boards will exist until December. Grippo is stemming from a brawl with two moving on to join the Leadership Academy, a program Associated Press from Diane Hunt, a Bay Ridge resident who tracked men outside the Marriott hotel on developed by Schools Chancellor Joel Klein and the Regans without as much as a name or precinct num- Adams Street. -

BUNKER MENTALITY CB2 Tells Bloomie to Take Hike
INSIDE BROOKLYN’S WEEKLY NEWSPAPER Including The Downtown News, Carroll Gardens-Cobble Hill Paper and Fort Greene-Clinton Hill Paper ‘Nut’ gala raises $700G for BAM Published weekly by Brooklyn Paper Publications Inc, 26 Court St., Brooklyn 11242 Phone 718-834-9350 AD fax 718-834-1713 • NEWS fax 718-834-9278 © 2002 Brooklyn Paper Publications • 12 pages including GO BROOKLYN • Vol. 25, No. 51 BWN, DTG, PSG, MID • December 30, 2002 • FREE NEW YEAR’S BLAST! BUNKER MENTALITY CB2 tells Bloomie to take hike By Patrick Gallahue The Brooklyn Papers Calling it a hazard to Downtown Brooklyn and its residents, Community Board 2 and Councilman David Yassky this week came down strongly against the city’s plan to build a new Office of Emergency Management headquarters at 165 Cadman Plaza East, the former home of the American Red Cross. / File photo “On public safety grounds I just do not think this is a viable place for such a sensitive facility as the OEM headquarters next to ex- Plans to put the city’s Office of Emergency Management headquar- tremely sensitive, and quite possi- ters at the Red Cross building site at 165 Cadman Plaza East, have The Brooklyn Papers The Brooklyn bly, target facilities, namely the come under fire. The Brooklyn Papers / File photos Brooklyn Bridge and the federal courthouse,” Yassky said. OEM headquarters is built there. ceived a cold response from the Besides stating his position at a The OEM proposal is making its community and he pledged to re- GAP fireworks to mark 2003 public hearing before Borough way through the city’s public re- vise the design. -

Cop Saves Woman from Slope Rapist
GARCIA MAKES METS AS CLONES CLINCH BACK PAGE INSIDE BROOKLYN’S WEEKLY NEWSPAPER Including The Downtown News, Carroll Gardens-Cobble Hill Paper and Fort Greene-Clinton Hill Paper Painters take on avant-garde Published weekly by Brooklyn Paper Publications at 26 Court St., Brooklyn, NY 11242 Phone 718-834-9350 © Brooklyn Paper Publications • 16 pages including GO BROOKLYN • Vol.26, No. 36 BWN • September 8, 2003 • FREE Cop saves woman from Slope rapist By Patrick Gallahue thug took off and Ward chased him and tack- instinct was to go over and chase the perp Bridge. A suspect was arrested in the incident. The Brooklyn Papers led him near Prospect Park West. down,” said Deputy Inspector Edward On July 10, a 45-year-old woman was at- The suspect, Bennie Hogan, 39, of Browns- Mullen, commanding officer of the 78th tacked at Lookout Hill, inside the park off A quick-thinking police officer chased ville, has been charged with attempted rape, as- Precinct. Prospect Park South and Terrace Place, at down a career criminal and convicted sex sault and resisting arrest. The scooter was purchased for the precinct around 10:45 am. offender on the Park Slope side of The beaten and bloodied victim was taken last Christmas by Park Slope Councilman Bill The assailant was scared off by another Prospect Park on Tuesday after the sus- to Kings County Medical Center where she DeBlasio using discretionary funds allocated jogger as the victim tried to fight off her at- pect allegedly attempted to rape a 33-year- was treated for severe cuts and bruises. -

Brooklyn Night Bus
BBrrookkllyynn BBuuss Night Night M Mapap 1:00 AM to 5:00 AM Q 23 St ae E Northern Blvd nq 46 100 Queensboro Plaza CHELSEA 12 28 St 33 St Q n7 23 St Q 66 f MADISON AV Court Sq 39 E Queens Plaza HIGH LINE W 14 ST 23 St 46 7 23 St 65 St EIGHTH AV E E 37 AV 12 28 St HUNTERS 39 AV FEDERAL 36 AV ELEVATED 62 Q Jackson Hts Downtown Brooklyn Court Sq 7 Q Downtown Brooklyn BUILDING LIC / Queens Plaza New Jersey PARK ae L 8 Av 18 St POINT 32 Roosevelt Av 14 St nq G 70 X Q70 SBS E 38 AV 23 St E 34 St / 21 St G Court Sq Q to LaGuardia SBS CADMAN PLAZA WEST 14 St 28 LEXINGTON AV THOMSO 46 ST Midtown 60 Q Q F ED KOCH 12 f Vernon Blvd - WOODSIDE TILLARY ST 14 St SUNNYSIDE 35 ST ROTUNDA East River Ferry Jackson Av N AV LIRR 53 70 Q 46 JACKSON AV YARD 39 ST 6 Av L Hunters Point South / 7 WOODSIDE SBS SBS GALLERY 26 62 66 23 St 42 ST QUEENSBORO BRIDGE UNION Long Island City 52 41 23 ST ST 7 33 St- 7 74 St- SQUARE LIRR Q 7 7 PIERREPONT ST Q BROADWAY E 23 ST WATERSIDE Rawson St 7 Bway East River Ferry HUNTERSPOINT AV 32 69 St Q LONG PARK LIRR 30 PL 100 PLAZA 7 7 40 St 7 52 St 61 St - 38 26 LONG Lowery St Woodside 32 ISLAND ISLAND Hunters SUNNYSIDE 7 Q IRVING PL 3 AV McGUINNESS BLVD Point Av 58 ST BROOKLYN 14 St- 11 ST Q CHRISTOPHER ST SEVENTH AV nql CITY 46 St QUEENS BLVD Q 60 Q 21 ST CITY Union Sq 30 ST HISTORICAL FAMILY QUEENS PLAZA S PETER 39 Bliss St 63 ST 1 2 AV 25 102 ROOSEVELT 101 21 St VAN DAM SOCIETY NY STATE JOHNSON ST F CRESCENT ST Christopher St 12 l 3 Av COOPER Q MONTAGUE ST COURT Queensbridge Sheridan Sq 48 AV 44 AV SUPREME 25 ISLAND VILLAGE -
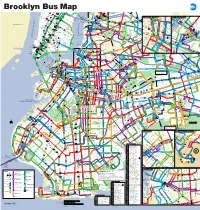
Brooklyn Bus Map
Brooklyn Bus Map To E 5757 StSt 7 7 Q M R C E BM Queensboro N W Northern Blvd Q Q 100 Plaza 23 St 23 St R W 5 5 AV 1 28 St 6 E 34 ST 103 69 Q WEST ST 66 33 St Court Sq 7 7 Q 37 AV Q18 to 444 DR 9 M CHELSEA F M 4 D 3 E E M Queens Astoria R Plaza Q104 to BROADWAY 23 St QUEENS MIDTOWN7 Court Sq - Q 65 St HIGH LINE W 14 S 23 ST 23 St R 7 46 AV 39 AV Astoria 18 M R 37 AV 1 X 6 Q FEDERAL 36 ELEVATED T 32 62 Q Jackson Hts Downtown Brooklyn LIC / Queens Plaza AV 47 AV D Q Downtown Brooklyn BUILDING 67 LIC / Queens Plaza 27 1 T Q PARK 18 St MADISON28 AVSt 32 ST Roosevelt Av 14 St A C E TUNNEL G Court Sq 58 ST 70 R W 67 212 ST 102 E ST 44 Q70 SBS L 8 Av X 28 S Q 6 S E F 38 T 4 TILLARY ST E 34 St / HUNTERSHUNTER BLV21 StSt G SKILLMAN AV SBS 103 AV 28 23 St VERNON to LaGuardia BACABAC F 14 St LEXINGTON AV T THOMSO 0 48 T O 6 Q Q M R ED KOCH Midtown 9 ST Q CADMAN PLAZA F M VernonVe Blvdlvd - 5 ST T 37 S WOODSIDE 1 2 3 14 St 3 LIRRRR 53 70 POINT JaJ cksonckson AvAv SUNNYSIDE S 104 ROTUNDA Q East River Ferry N AV 40 ST Q 2 ST EIGHTH AV 6 JACKSONAV QUEENS BLVD 43 AV NRY S 40 AV Q 3 23 St 4 WOODSIDEOD E TILLARY ST L 7 7 LIRR YARD SBS SBS 32 GALLERY 26 H N 66 23 Hunters Point South / 46 St T AV HE 52 41 QUEENSBORO 9 UNION E 23 ST M 7 L R 6 BROADWAY BRIDGEB U 6 Av HUNTERSPOINT AV 7 33 St- Bliss St E 7 Q32 E Long Island City A 7 7 69 St to 7 PIERREPONT ST W Q SQUARE Rawson St WOOD 69 ST 62 57 D WATERSIDE 49 AV T ROOSEV 61 St - Jackson G Q Q T 74 St- LONG East River Ferry T LIRR 100 PARK S ST 7 T Woodside Bway PARK AV S S 7 40 St S Heights 103 1 38 26 PLAZA -

Building the Future of New York Parks and Open Space
NEW YORK BUILDING CONGRESS BUILDING THE FUTURE OF NEW YORK PARKS AND OPEN SPACE In collaboration with: For New York to continue to thrive as a global Our Building the Future of New York series springboards real city, now is the time to not only dream big, but to conversations between stakeholders and helps move the needle on put shovels in the ground. These proposals may some of the region’s biggest challenges. The series urges policy makers seem aspirational, but New York must see itself and the public to return to a spirit of aspirational planning and building in this vision and reshape our city if we are truly by proposing substantive projects and significant administrative going to continue to lead the world. reforms that could engender a new century of growth and success. Demand for Parks and Open Space Parks are an essential public service, providing for the social, economic, physical and mental wellbeing of nearly nine million New Yorkers. In the nation’s most densely populated city, they offer respite from the chaos of urban life, encourage active lifestyles, foster community engagement, counteract the effects of climate change and strengthen local economies. During the COVID-19 pandemic, parks are safe places to social distance, relieve stress and remain healthy. Open public spaces also complement the role of traditional parks by activating streets and sidewalks for recreation, relaxation and commerce. The City of New York has recently expanded programs to convert space exclusively for vehicular use into safe, shared space that all New Yorkers can use. The Open Streets initiative, which encompasses Play Streets, Cool Streets and Open Restaurants, temporarily reclaims sidewalks, parking spaces and roadways for pedestrians, cyclists, children, those escaping the heat and restaurants providing outdoor dining. -
Take a Good Look at the Brooklyn Skyline, Because What You See Won’T Be There for Long
September 1, 2015 From left: Greenland Forest City Ratner Partners’ 550 Vanderbilt in Pacific Park and Hudson Companies’ Gowanus Green Take a good look at the Brooklyn skyline, because what you see won’t be there for long. Fueled by a frothy economy and unrelenting demand, developers hit the gas on residential projects over the past 18 months. Overall, Brooklyn development topped 41.6 million square feet— second only to Manhattan — spanning nearly 600 projects and 45,359 apartments, according to The Real Deal’s analysis of building permits and offering plans filed between Jan. 1, 2011 and July 31, 2015. Notably, a massive 85 percent of those plans were submitted since January 2013. Since that time, developers initiated plans for 35.3 million square feet, 534 projects and 38,375 residential units, TRD found. Hudson Companies dominated the borough’s list of the most prolific developers by square footage. The firm filed plans for just over 2.71 million square feet since 2011, including 2,307 units spread over 14 projects. The largest, Gowanus Green, is a planned mixed-income village on 5.8 acres in Gowanus, which Hudson is developing with partners Bluestone Organization, the Fifth Avenue Committee and Jonathan Rose Companies. Plans call for eight towers totaling 790,000 square feet with 774 rental and condo units. Meanwhile, David and Jed Walentas’ Two Trees Management, the developers behind the $1.5 billion redevelopment of the old Domino Sugar refinery in Williamsburg, clocked in at No. 2 with just over 1.96 million square feet across seven projects with more than 2,200 total units.