Research Article High Origin of Radial Artery: a Comparative, Anatomical and Embryological Consideration
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Morphology of Common Interosseous Artery and Its Clinical
Scholars Journal of Applied Medical Sciences (SJAMS) ISSN 2320-6691 (Online) Sch. J. App. Med. Sci., 2015; 3(3B):1126-1131 ISSN 2347-954X (Print) ©Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources) www.saspublisher.com Research Article The Morphology of Common Interosseous Artery and its Clinical Significance Waseem Al Talalwah1*, Dereje Getachew2 and Roger Soames3 1King Abdullah International Medical Research Center / King Saud bin Abdulaziz University for Health Sciences, College of Medicine, Department of Basic Medical Sciences Hospital – NGHA, Riyadh, P.O. Box 3660, Riyadh 2Anatomy Department, College of Medicine and Health sciences, Hawassa University, Awassa, 1560 3Centre for Anatomy and Human Identification, College of Art, Science and Engineering, University of Dundee Dundee, DD1 5EH, UK *Corresponding author Dr. Waseem Al-Talalwah Abstract: The common interosseous artery is main branch the ulnar artery which divides into anterior and posterior interosseous branches. The current study investigates common interosseous artery and its branch to provide detailed information regarding the morphology which would be of use to clinicians, orthopaedic surgeons, plastic surgeons and anatomists. Routine dissections of the right and left upper limb of 34 adult cadavers (20 male and 14 female: mean age 78.9 year) were undertaken. The common interosseous artery presents in 67.6% whereas it is congenital absence in 32.4%. The origin distance of bifurcation of common interosseous from the ulnar artery origin is between 33.11 and 33.45 mm. The anterior and posterior interosseous arteries present in 98.5% and 92.9% whereas they are congenital absence in 1.5% and 7.1% respectively in total cases. -

Volume-8, Issue-3 July-Sept-2018 Coden:IJPAJX-CAS-USA
Volume-8, Issue-3 July-Sept-2018 Coden:IJPAJX-CAS-USA, Copyrights@2018 ISSN-2231-4490 Received: 8th June-2018 Revised: 15th July-2018 Accepted: 16th July-2018 DOI: 10.21276/Ijpaes http://dx.doi.org/10.21276/ijpaes Case Report VARIANT ARTERIAL PATTERN IN THE FOREARM WITH ITS EMBRYOLOGICAL BASIS Vaishnavi Joshi and Dr. Shaheen Sajid Rizvi Department of Anatomy, K. J. Somaiya Medical College, Somaiya, Ayurvihar, Eastern Express Highway, Sion, Mumbai-400 022 ABSTRACT: During routine dissection for the first MBBS students, we observed that the radial artery was absent in the right upper limb of a 70 years old, donated embalmed male cadaver in the Department of Anatomy, K.J.Somaiya Medical College, Sion. In the lower part of the arm, brachial artery divided into ulnar and common Interosseous artery. Anterior interosseous artery was large in size. Deep to pronator quadratus, it turned laterally and reached the dorsum of the hand, where its lateral branch supplied the thumb and index finger and its medial branch dipped into the palm at the second inter-metacarpal space. Superficial palmar arch was absent. Digital arteries from the medial and lateral branches of ulnar artery supplied the fingers. Embryological basis is presented. Key words: Brachial artery, Anterior interosseous artery, Common Interosseous artery, Radial artery, ulnar artery *Corresponding autor: Dr. Shaheen Sajid Rizvi, Department of Anatomy, K. J. Somaiya Medical College, Somaiya, Ayurvihar, Eastern Express Highway, Sion, Mumbai-400 022; Email : rizvishaheen68@ gmail.com Copyright: ©2018 Dr. Shaheen Sajid Rizvi. This is an open-access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited INTRODUCTION The main artery of the arm, the brachial artery divides at the level of the neck of the radius into radial and ulnar arteries. -

Arteries of The
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Arteries of the Arm st The AXILLARY ARTERY begins at the border of the 1 rib as a continuation of the subclavian artery Subclavian artery The FIRST PART stretches between the 1st rib and the medial border of pectoralis minor. First rib It has only one branch – the superior thoracic artery Superior thoracic artery The SECOND PART lies under the pectoralis Thoracoacromial artery minor; it has 2 branches: Which pierces the - The Thoracoacromial artery costocoracoid membrane - The Lateral Thoracic artery deep to the clavicular head The THIRD PART stretches from the lateral border of pectoralis major of pectoralis minor to the inferior border of Teres Major; it has 3 branches: Pectoralis major - The Anterior circumflex humeral artery - The Posteror circumflex humeral artery Pectoralis minor - The Subscapular artery Axillary nerve Posterior circumflex humeral artery Lateral Thoracic artery Travels through the quadrangular space together Which follows the lateral with the axillary nerve. It’s the larger of the two. border of pectoralis minor onto the chest wall Anterior circumflex humeral artery Passes laterally deep to the coracobrachialis and Circumflex scapular artery the biceps brachii Teres Major Passes dorsally between subscapularis and teres major to supply the dorsum of the scapula Profunda Brachii- deep artery of the arm Thoracodorsal artery Passes through the lateral triangular space (with Goes to the inferior angle of the scapula, the radial nerve) into the posterior compartment Triceps brachii supplies mainly the latissimus dorsi of the arm. -

Arterial Damages in Acute Elbow Dislocations: Which Diagnostic Tests Are Required? Christoph Lutter,1,2 Ronny Pfefferkorn,2 Volker Schoeffl2
Rare disease BMJ Case Reports: first published as 10.1136/bcr-2016-216336 on 19 July 2016. Downloaded from CASE REPORT Arterial damages in acute elbow dislocations: which diagnostic tests are required? Christoph Lutter,1,2 Ronny Pfefferkorn,2 Volker Schoeffl2 1CVPath Institute, SUMMARY radiographs. After reduction, the left arm was Gaithersburg, Maryland, USA Blunt vessel injuries of peripheral arteries caused by a immobilised in a splint and the patient was dis- 2Department of Sports Orthopedics, Sports Medicine, direct trauma are rare. Studies have described the charged. Several days later, MRI was performed, Sports Traumatology, frequency of arterial ruptures following closed elbow showing a partial detachment of the extensor Department for Orthopedics dislocations in 0.3–1.7% of all cases. However, arterial muscles from the radial epicondyle and a medial and Traumatology, Klinikum damage does not always necessarily appear as a sided ligamental lesion (figure 1). In addition, a Bamberg, Bamberg, Germany complete rupture of the vessel with a loss of peripheral partial rupture of the brachial muscle tendon and a Correspondence to circulation and ischaemic symptoms; a relatively strong haematoma within the brachial muscle were Dr Christoph Lutter, periarticular system of collaterals can maintain detected. christoph.lutter@googlemail. circulation. Furthermore, the traumatic dislocation can com also cause intimal tears, arterial dissections and INVESTIGATIONS Accepted 5 July 2016 aneurysms or thrombosis. In all cases of vessel injury, including total disruption, a peripheral pulse might still Two weeks later, the patient was seen in our out- be palpable. 3 weeks after an acute elbow dislocation, patient clinic. The left arm was still immobilised in we have diagnosed a patient with a long-segment a 110° extension position in the elbow, and an old stenosis of the brachial artery and a thrombosis of the haematoma was visible on the medial side of the radial artery. -
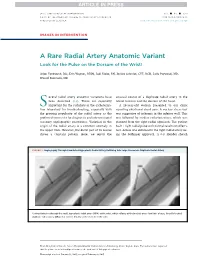
A Rare Radial Artery Anatomic Variant Look for the Pulse on the Dorsum of the Wrist!
JACC: CARDIOVASCULAR INTERVENTIONS VOL. - ,NO.- ,2017 ª 2017 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jcin.2017.02.026 IMAGES IN INTERVENTION A Rare Radial Artery Anatomic Variant Look for the Pulse on the Dorsum of the Wrist! Arjun Venkatesh, BSC, Erin Wagner, RT(R), Jodi Klebe, RN, Jessica Schmidt, CVT, RCIS, Laila Payvandi, MD, Wassef Karrowni, MD everal radial artery anatomic variations have unusual course of a duplicate radial artery in the S been described (1,2). These are especially lateral forearm and the dorsum of the hand. important for the radialists in the catheteriza- A56-year-oldwomanpresentedtoourclinic tion laboratory for troubleshooting, especially with reporting exertional chest pain. A nuclear stress test the growing popularity of the radial artery as the was suggestive of ischemia in the inferior wall. This preferred access site for diagnostic and interventional was followed by cardiac catheterization, which was coronary angiographic procedures. Variation in the planned from the right radial approach. The patient origin of the radial artery is a common anomaly in had 1þ right radial pulse with normal results on Allen’s the upper limb. However, the distal part of its course test. Access was obtained in the right radial artery us- shows a constant pattern. Here, we report the ing the Seldinger approach. A 6-F Slender sheath FIGURE 1 Angiography Through CannulatedHypoplasticRadialArteryRefluxing Into Large Anomalous Duplicate Radial Artery Contrast injection through the small, hypoplastic radial artery (HRA) at the wrist, which refluxes at the brachial artery level into a large, laterally located duplicate radial artery (DRA) that crosses distally to the dorsum of the wrist. -

A Case of Persistent Median Artery Splitting
A CASE OF PERSISENT MEDIAN ARTERY SPLITTING THE MEDIAN NERVE Nicolette Alberti, Ilana Anmuth, Justin Canakis, David Bigley, Maryanne Lubas, Kevin Amuquandoh, Michael McGuinness Department of Bio-Medical Sciences and Center for Chronic Disorders of Aging, Philadelphia College of Osteopathic Medicine, Philadelphia, PA 19131. ABSTRACT RESULTS 3 Introduction: Development of vascular abnormalities throughout the body are not Median n uncommon. Little insight can be found regarding the clinical manifestations and Artery & nerve progression through arm: development of these irregularities in the current data, indicating that further research • Brachial artery runs medial to lateral across the anterior surface of the median nerve PMA needs to be done in order to gain full understanding of their implications. In the current • The Ulnar and Radial arteries originate in the median cubital fossa posterior to the pronator case presentation, a persistent median artery (PMA) was identified in the left forearm of teres muscle and distal to the elbow joint. a cadaver. Normal vasculature of the forearm proceeds as follows; the brachial artery splits into the radial and ulnar arteries. The common interosseous artery branches off of Artery & nerve progression through forearm (Figure 1A and 2): the ulnar artery and then splits into an anterior and posterior portion. The anterior • Radial artery continues through the arm along a typical path terminating in the hand. interosseous artery pierces the interosseous membrane and anastomoses with the • The ulnar artery traveled 3.8 cm before the common interosseous artery originates. SPA posterior interosseous artery on the dorsum of the hand to form the dorsal carpal arch. • The common interosseous artery measures 0.5 cm before trifurcating into anterior On the ventral aspect of the hand the radial and ulnar arteries form the superficial and interosseous posterior interosseous and PMA. -

An Anatomical Variation of Superficial Palmar Arch and Its Clinical Significance: a Case Report
Case Report Anatomy Journal of Africa 2 (1): 114-116 (2013) AN ANATOMICAL VARIATION OF SUPERFICIAL PALMAR ARCH AND ITS CLINICAL SIGNIFICANCE: A CASE REPORT Nair CKV, Nair RV, Mookambica RV, Somayaji SN, Somayaji K, Jetti R *Corresponding Author: Dr. Raghu Jetti, Department of Anatomy, Melaka Manipal Medical College (Manipal campus), Manipal University, Manipal, 576104. Karnataka, India. Phone: 91-820-2922635. Fax: 91-820-2571905. Mail: [email protected] SUMMARY The familiarity of variations in vascular architecture of hand is helpful to surgeons, in microsurgical procedures precipitated by crush injuries of hand and in amputations. The efficiency of collateral circulation in hand is essential in certain peripheral vascular diseases like Raynaud’s disease and in harvesting of the radial artery for coronary bypass graft. Variation in the formation of superficial palmar arch is common. We report a rare variation of equitable distribution of superficial palmar arch. Variations of the superficial palmar arterial arch are not uncommon. Allen’s test, doppler ultra sound, arterial angiography pulse oximetry should therefore be used to assess the efficiency of collateral circulation before surgical interventions. Keywords: Vascular anatomy; superficial palmar arch INTRODUCTION formed by anastomosis of ulnar and median According to the classical description, superficial arteries. In case of type 4 it is formed by joining palmar arch (SPA) is formed by the continuation of ulnar, radial, median arteries. In type 5 it is of superficial branch of ulnar artery into the formed by branch from deep palmar arch palm, completed by a branch from radial artery. (Loukas et al., 2005). We describe a case of a The SPA lies between palmar aponeurosis, long non-dominant SPA, superficial to the flexor flexor tendons, lumbrical muscles and digital retinaculum. -

The Superficial Palmar Branch of the Radial Artery: a Corrosion Cast Study M
Folia Morphol. Vol. 77, No. 4, pp. 649–655 DOI: 10.5603/FM.a2018.0033 O R I G I N A L A R T I C L E Copyright © 2018 Via Medica ISSN 0015–5659 www.fm.viamedica.pl The superficial palmar branch of the radial artery: a corrosion cast study M. Ilić1, M. Milisavljević2, A. Maliković2, D. Laketić3, D. Erić4, J. Boljanović2, A. Dožić5, B.V. Štimec6, R. Manojlović1 1Institute for Orthopaedic Surgery and Traumatology, Clinical Centre of Serbia, Faculty of Medicine, University of Belgrade, Serbia 2Laboratory for Vascular Anatomy, Institute of Anatomy, Faculty of Medicine, University of Belgrade, Serbia 3Medical Department, Faculty of Sport and Physical Education, University of K. Mitrovica, Serbia 4Department of Plastic, Reconstructive, and Hand Surgery, Faculty of Medicine, University of East Sarajevo, Foča, Republic of Srpska, Bosnia and Herzegovina 5Institute of Anatomy, Faculty of Dentistry, University of Belgrade, Serbia 6Faculty of Medicine, Department of Cellular Physiology and Metabolism, Anatomy Sector, University of Geneva, Switzerland [Received: 10 January 2018; Accepted: 14 March 2018] Background: Surgical procedures such as thenar flaps and radial artery (RA) harvesting call for an elaborate anatomical study of the RA’s superficial palmar branch (SPB). The aim of this study was to describe the branching pattern of this vessel related to the morphometric characteristics and variations of this artery. Materials and methods: Twenty 4% formalin solution-injected hands were dis- sected. For the morphometric study we used another group of 35 human hands of adult persons, injected with methyl methacrylate fluid into the ulnar and radial arteries. As soon as polymerisation was completed, a 40% solution of potassium hydroxide was applied for corrosion. -

A Rare Variation in Origin of Common Interosseous Artery: a Review of Anatomical Studies and Case Report
Summer & Autumn 2017, Volume 14 Number 2 Review Paper: A Rare Variation in Origin of Common Interosseous Artery: A Review of Anatomical Studies and Case Report Saieed Babaee1, Maryam Baazm1, Parvindokht Bayat1, Mohammad Bayat1, Mohammad Hassan Sakhaie1* 1. Department of Anatomy, School of Medicine, Arak University of Medical Sciences, Arak, Iran. Citation: Babaee S, Baazm M, Bayat P, Bayat M, Sakhaie MH. A Rare Variation in Origin of Common Interosseous Artery: A Review of Anatomi- cal Studies and Case Report. Anatomical Sciences. 2017; 14(2):61-64. Dr. Mohammad Hasan Sakhaie is the assistance professor of Anatomical Sciences, at the Department of Anatomy, School of Medicine, Arak University of Medical Sciences. His research interests are Neurodegenerative disease, Neurosciences, and Gross anatomy. Article info: A B S T R A C T Received: 21 Oct 2016 Accepted: 01 Feb. 2017 An unusual origin of the common interosseous artery is reported in the paper. During educational Available Online: 01 Jul. 2017 dissection of a 37-year-old male, a rare variation in the origin of common interosseous artery of the right upper limb was observed. The common interosseous artery directly separated from radial artery. The right anterior interosseous artery is continued from common interosseous artery. Anterior and posterior ulnar recurrent arteries arising from common interosseous artery were noted on the right side of upper limb. In the present case, the median artery was replaced with anterior interosseous artery. Additionally, the ulnar artery passed superficially on flexor Keywords: digitorum superficialis. In the cadaver, there was no other arterial or muscular variation. The Anatomic variation, embryological interpretation of this variation may be attributed to arising of the artery as a Interosseous artery, Radial result of modifications to the normal pattern of capillary vessel maintenance and regression. -

Abnormal Radial Artery in Down's Syndrome
Arch Dis Child: first published as 10.1136/adc.61.9.885 on 1 September 1986. Downloaded from Archives of Disease in Childhood, 1986, 61, 885-890 Abnormal radial artery in Down's syndrome R N S LO, M P LEUNG, K C LAU, AND C Y YEUNG Department of Paediatrics, Queen Mary Hospital, University of Hong Kong SUMMARY Abnormal arterial patterns in the forearm were discovered in 12 of 77 patients (16%) with Down's syndrome. Eight patients had an enlarged anterior interosseous artery, the distal portion of which was palpable over the dorsum of the hand; in seven it was associated with absence of the radial artery and in one it coexisted with the radial and ulnar arteries. Three patients had a hypoplastic radial artery and a relatively dominant ulnar artery. One patient had a vestigial radial artery that ended as muscular branches in the forearm. The developmental aspects of these aberrations are discussed. The radial artery in its superficial position on the Patients and methods volar aspect of the wrist offers a well known access for clinical evaluation of the circulation. Its palpable From January 1983 to December 1985 a total of 1087 pulsation on the radial side of the wrist between the Chinese children were studied. Of these, 510 were flexor carpi radialis tendon medially and the bony otherwise normal children with congenital heart prominence of the lower part of the radius laterally disease and 77 were patients with Down's syndrome copyright. has been remarkably constant, and reports on (40 boys and 37 girls), of whom 50 had congenital variations are scanty.t 2 Reports on congenital heart heart disease. -

High Origin of Radial Artery: an Anatomical Variation with Its Embryological Basis & Clinical Significance
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article High Origin of Radial Artery: An Anatomical Variation with Its Embryological Basis & Clinical Significance Kusum R Gandhi1, K.Naga Vidya Lakshmi2 1Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Bhopal 2Associate Professor, Department of Anatomy, St. Joseph’s Dental College, Eluru, Andhra Pradesh Corresponding Author: K.Naga Vidya Lakshmi ABSTRACT BACKGROUND: Radial artery is the smaller terminal branch of brachial artery. Abnormal variations in the anatomy of radial artery may produce an iatrogenic injury leading to undesired complications. MATERIALS & METHODS: Study was carried out on 18 formalin fixed cadavers i.e. 36 limbs of adult age in the Department of Anatomy. Arm and forearm of both upper limbs were carefully dissected to note the variation in the origin of Radial artery. RESULT: Unilateral Variations of high origin of Radial artery were observed in two cases (5.55%). In first case, radial artery was originated from right brachial artery 13.5 centimetre above the intercondylar line while in second case it was 19 centimetres above the intercondylar line. CONCLUSION: In recent times, there has been an increase in the use of radial artery for various diagnostic & invasive procedures which requires the qualified apprehension of the variant anatomy to avoid iatrogenic injury and perform safe procedures. Key Words: Superficial Radial artery, High origin, Invasive procedures INTRODUCTION centimeter below the bend of elbow. It The insight of the course and the traverses deep to the brachioradialis muscle relationships of upper limb vasculature in the forearm and terminates in the hand by accounts for a lot of diagnostic measures forming the deep palmar arch after and handful surgical approaches. -

Anatomical Variations of the Superficial and Deep Palmar Arches
Folia Morphol. Vol. 64, No. 2, pp. 78–83 Copyright © 2005 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Anatomical variations of the superficial and deep palmar arches Marios Loukas1, 2, Danny Holdman1, Shelly Holdman1 1Department of Anatomy, American University of the Caribbean, Sint Maarten, Netherlands Antilles 2Harvard Medical School, Boston, MA, USA [Received 6 April 2004; Revised 21 February 2005; Accepted 22 February 2005] The use of radial arteries as an arterial bypass conduit is an invasive procedure which is becoming popular among various medical centres. The greatest risk associated with harvesting the radial artery is ischaemia of the soft tissues of the hand. In this study we dissected 200 hands derived from 100 formalin-fixed cadavers in order to identify arterial patterns that will allow safe removal of the radial artery for use in bypass procedures. A complete superficial palmar arch (SPA) was found in 90% of the cases and divided into 5 types, while the remain- ing 10% possessed an incomplete palmar arch. Types of SPA are designated by the letter S. In type S-I (40%), the SPA is formed by anastomosis of the superfi- cial volar branch of the radial artery to the ulnar artery. Type S-II (35%) is formed entirely of the ulnar artery. Type S-III (15%) is formed by anastomosis of the ulnar and median arteries. Type S-IV (6%) is formed by anastomosis of the ulnar, radial, and median arteries and Type S-V (4%) is formed by a branch of the deep palmar arch (DPA) communicating with the SPA.DPA was identified in all speci- mens and classified into three types, all designated by the letter D.