The Morphology of Common Interosseous Artery and Its Clinical
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Additional Branch of Brachial Artery Terminating in Superficial Palmar Arch
International Journal of Advances in Science Engineering and Technology, ISSN(p): 2321 –8991, ISSN(e): 2321 –9009 Vol-6, Iss-1, Spl. Issue-2 Mar.-2018, http://iraj.in ADDITIONAL BRANCH OF BRACHIAL ARTERY TERMINATING IN SUPERFICIAL PALMAR ARCH 1BILLAKANTI PRAKASH BABU, 2HUBAN THOMAS 1Associate Professor, Kasturba Medical College/Manipal Academy of Higher Education, Anatomy Department, Kasturba Medical College,Manipal,KARNATAKA-INDIA,576104 2Senior Lecturer, Kasturba Medical College/Manipal Academy of Higher Education, Anatomy Department, Kasturba Medical College,Manipal,KARNATAKA-INDIA,576104 E-mail: [email protected], [email protected] Abstract - Superficial palmar arch is an arterial arcade in the palm of the hand formed by superficial branch of ulnar artery and can be completed on lateral side by superficial palmar branch of radial artery or any one of these arteries viz. princeps pollicis artery, radialis indicis artery or the median artery. The arch develops as a terminal plexus of axis artery of upper limb which is later joined by median, ulnar and radial arteries as these arteries develop. The present study was conducted in the Department of Anatomy, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India on 60 formalin fixed adult human cadaver hands. Out of 60 (30 on right and 30 on left side) in one specimen a unique variation was encountered in the arteries taking part in the formation of superficial palmar arch on the right side. Superficial palmar arch formation was normal and in addition an additional branch arose from the medial side of the brachial artery just below the middle of the arm. -

Anatomy, Shoulder and Upper Limb, Brachial Artery
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Shoulder and Upper Limb, Brachial Artery Authors Thomas N. Epperson1; Matthew Varacallo2. Affiliations 1 University of Louisville School of Med. 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: January 4, 2019. Introduction The brachial artery is the extension of the axillary artery starting at the lower margin of the teres major muscle and is the major artery of the upper extremity. The brachial artery courses along the ventral surface of the arm and gives rise to multiple smaller branching arteries before reaching the cubital fossa.[1] These branching arteries include the deep brachial artery, the superior ulnar collateral artery, and the inferior ulnar collateral artery. Once the brachial artery reaches the cubital fossa, it divides into its terminal branches: the radial and ulnar arteries of the forearm. The brachial artery and its branches supply the biceps brachii muscle, triceps brachii muscle, and coracobrachialis muscle. The median nerve, a division of the brachial plexus, initially lies lateral to the brachial artery at its proximal segment. At its distal segment, the median nerve crosses the medial side of the brachial artery and lies in the ventral cubital fossa. Structure and Function The following are the branches of the brachial artery in order of origin, proximal to distal. Profunda Brachii/Deep Brachial Artery The first branch of the brachial artery, this branch of the brachial artery arises below the inferior border of the teres major muscle. -

Research Paper Medical Science Variant Brachial Artery with Incomplete Superficial Palmer Arch - a Case Report
Volume : 2 | Issue : 1 | Jan 2013 • ISSN No 2277 - 8160 Research Paper Medical Science Variant Brachial Artery with Incomplete Superficial Palmer Arch - A Case Report Dr. Sharadkumar Associate Professor, Department of Anatomy, K. J. Somaiya Medical College, So- Pralhad Sawant maiya Ayurvihar, Eastern Express Highway, Sion, Mumbai During routine dissection, of the right upper limb of a 70 years old donated embalmed male cadaver in the ABSTRACT Department of Anatomy, K.J. Somaiya Medical College, Sion, Mumbai, India, we observed a high level trifurcation of the brachial artery into the radial, ulnar and common interosseous arteries. The brachial artery trifurcated above the cubital fossa in the lower part of the arm. The ulnar artery travelled downward superficial to the superficial flexor muscles of the forearm. The common interosseous artery was longer in length. The common interosseous artery divided at unusual site in the cubital fossa into the anterior and posterior interosseous arteries. There were no associated altered anatomy of the nerves observed in the specimen. The variations were unilateral and the left upper limb was normal. The photographs of the high level trifurcation of the brachial artery into radial, ulnar and common interosseous artery were taken for proper documentation. Topographical anatomy of the normal and abnormal variations of the axillary artery are clinically important for surgeons, orthopaedicians operating on the supracondylar fracture of humerus and radiologists performing angiographic studies on the upper limb. KEYWORDS: Brachial Artery, Trifurcation, Radial Artery, Ulnar Artery, Common Interosseous Artery, Surgeons, Orthopaedicians Introduction: The brachial artery ends in the cubital fossa by dividing into the ra- dial and ulnar arteries. -

01 Natsis.P65
Folia Morphol. Vol. 68, No. 4, pp. 193–200 Copyright © 2009 Via Medica R E V I E W A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Persistent median artery in the carpal tunnel: anatomy, embryology, clinical significance, and review of the literature K. Natsis1, G. Iordache2, I. Gigis1, A. Kyriazidou1, N. Lazaridis1, G. Noussios3, G. Paraskevas1 1Department of Anatomy, Medical School, Aristotle University of Thessaloniki, Greece 2University of Medicine and Pharmacy of Craiova, Romania 3Laboratory of Anatomy, Department of Physical Education and Sport Sciences (Serres), Aristotle University of Thessaloniki, Greece [Received 5 June 2009; Accepted 16 September 2009] The median artery usually regresses after the eighth week of intrauterine life, but in some cases it persists into adulthood. The persistent median artery (PMA) pas- ses through the carpal tunnel of the wrist, accompanying the median nerve. During anatomical dissection in our department, we found two unilateral cases of PMA originating from the ulnar artery. In both cases the PMA passed through the carpal tunnel, reached the palm, and anastomosed with the ulnar artery, forming a medio-ulnar type of superficial palmar arch. In addition, in both cases we observed a high division of the median nerve before entering the carpal tunnel. Such an artery may result in several complications such as carpal tunnel syndrome, pronator syndrome, or compression of the anterior interosseous nerve. Therefore, the presence of a PMA should be taken into consideration in clinical practice. This study presents two cases of PMA along with an embryological explanation, analysis of its clinical significance, and a review of the literature. -

Volume-8, Issue-3 July-Sept-2018 Coden:IJPAJX-CAS-USA
Volume-8, Issue-3 July-Sept-2018 Coden:IJPAJX-CAS-USA, Copyrights@2018 ISSN-2231-4490 Received: 8th June-2018 Revised: 15th July-2018 Accepted: 16th July-2018 DOI: 10.21276/Ijpaes http://dx.doi.org/10.21276/ijpaes Case Report VARIANT ARTERIAL PATTERN IN THE FOREARM WITH ITS EMBRYOLOGICAL BASIS Vaishnavi Joshi and Dr. Shaheen Sajid Rizvi Department of Anatomy, K. J. Somaiya Medical College, Somaiya, Ayurvihar, Eastern Express Highway, Sion, Mumbai-400 022 ABSTRACT: During routine dissection for the first MBBS students, we observed that the radial artery was absent in the right upper limb of a 70 years old, donated embalmed male cadaver in the Department of Anatomy, K.J.Somaiya Medical College, Sion. In the lower part of the arm, brachial artery divided into ulnar and common Interosseous artery. Anterior interosseous artery was large in size. Deep to pronator quadratus, it turned laterally and reached the dorsum of the hand, where its lateral branch supplied the thumb and index finger and its medial branch dipped into the palm at the second inter-metacarpal space. Superficial palmar arch was absent. Digital arteries from the medial and lateral branches of ulnar artery supplied the fingers. Embryological basis is presented. Key words: Brachial artery, Anterior interosseous artery, Common Interosseous artery, Radial artery, ulnar artery *Corresponding autor: Dr. Shaheen Sajid Rizvi, Department of Anatomy, K. J. Somaiya Medical College, Somaiya, Ayurvihar, Eastern Express Highway, Sion, Mumbai-400 022; Email : rizvishaheen68@ gmail.com Copyright: ©2018 Dr. Shaheen Sajid Rizvi. This is an open-access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited INTRODUCTION The main artery of the arm, the brachial artery divides at the level of the neck of the radius into radial and ulnar arteries. -

Arteries of The
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Arteries of the Arm st The AXILLARY ARTERY begins at the border of the 1 rib as a continuation of the subclavian artery Subclavian artery The FIRST PART stretches between the 1st rib and the medial border of pectoralis minor. First rib It has only one branch – the superior thoracic artery Superior thoracic artery The SECOND PART lies under the pectoralis Thoracoacromial artery minor; it has 2 branches: Which pierces the - The Thoracoacromial artery costocoracoid membrane - The Lateral Thoracic artery deep to the clavicular head The THIRD PART stretches from the lateral border of pectoralis major of pectoralis minor to the inferior border of Teres Major; it has 3 branches: Pectoralis major - The Anterior circumflex humeral artery - The Posteror circumflex humeral artery Pectoralis minor - The Subscapular artery Axillary nerve Posterior circumflex humeral artery Lateral Thoracic artery Travels through the quadrangular space together Which follows the lateral with the axillary nerve. It’s the larger of the two. border of pectoralis minor onto the chest wall Anterior circumflex humeral artery Passes laterally deep to the coracobrachialis and Circumflex scapular artery the biceps brachii Teres Major Passes dorsally between subscapularis and teres major to supply the dorsum of the scapula Profunda Brachii- deep artery of the arm Thoracodorsal artery Passes through the lateral triangular space (with Goes to the inferior angle of the scapula, the radial nerve) into the posterior compartment Triceps brachii supplies mainly the latissimus dorsi of the arm. -

Arterial Damages in Acute Elbow Dislocations: Which Diagnostic Tests Are Required? Christoph Lutter,1,2 Ronny Pfefferkorn,2 Volker Schoeffl2
Rare disease BMJ Case Reports: first published as 10.1136/bcr-2016-216336 on 19 July 2016. Downloaded from CASE REPORT Arterial damages in acute elbow dislocations: which diagnostic tests are required? Christoph Lutter,1,2 Ronny Pfefferkorn,2 Volker Schoeffl2 1CVPath Institute, SUMMARY radiographs. After reduction, the left arm was Gaithersburg, Maryland, USA Blunt vessel injuries of peripheral arteries caused by a immobilised in a splint and the patient was dis- 2Department of Sports Orthopedics, Sports Medicine, direct trauma are rare. Studies have described the charged. Several days later, MRI was performed, Sports Traumatology, frequency of arterial ruptures following closed elbow showing a partial detachment of the extensor Department for Orthopedics dislocations in 0.3–1.7% of all cases. However, arterial muscles from the radial epicondyle and a medial and Traumatology, Klinikum damage does not always necessarily appear as a sided ligamental lesion (figure 1). In addition, a Bamberg, Bamberg, Germany complete rupture of the vessel with a loss of peripheral partial rupture of the brachial muscle tendon and a Correspondence to circulation and ischaemic symptoms; a relatively strong haematoma within the brachial muscle were Dr Christoph Lutter, periarticular system of collaterals can maintain detected. christoph.lutter@googlemail. circulation. Furthermore, the traumatic dislocation can com also cause intimal tears, arterial dissections and INVESTIGATIONS Accepted 5 July 2016 aneurysms or thrombosis. In all cases of vessel injury, including total disruption, a peripheral pulse might still Two weeks later, the patient was seen in our out- be palpable. 3 weeks after an acute elbow dislocation, patient clinic. The left arm was still immobilised in we have diagnosed a patient with a long-segment a 110° extension position in the elbow, and an old stenosis of the brachial artery and a thrombosis of the haematoma was visible on the medial side of the radial artery. -

A Variant Branch of the Axillary Artery Impacting in the Superficial Palmar Arch Composition
Case Report Annals of Clinical Anatomy Published: 25 Jun, 2018 A Variant Branch of the Axillary Artery Impacting in the Superficial Palmar Arch Composition Expedito S Nascimento Jr*, Jorge Landivar Coutinho, Karolina Duarte Rego, Jeovana Pinheiro F Souza, Marina Maria VF Caldas, Naryllenne Maciel Araújo, Wylqui Mikael G Andrade and Fernando Vagner Lobo Ladd Department of Morphology, Bioscience Center, Federal University of Rio Grande do Norte, Brazil Abstract During routine dissection of an approximately 60-year-old female cadaver for the undergraduate medical students at Morphology Department of Federal University of Rio Grande do Norte, Brazil, was observed a variant branch originated from the second part of the axillary artery. The second part of the right axillary artery gave rise to aberrant brachial artery that travels down superficially in the medial aspect of the upper limb. Furthermore, this superficial brachial artery terminates in the superficial palmar arch completely replacing the ulnar artery at this level. Variations in the upper limb arterial distribution are notably important for surgeons performing interventional or diagnostic in vascular diseases. Keywords: Axillary artery; Superficial palmar arch; Anatomic variation Introduction The axillary artery is a continuation of the subclavian artery, extending from the outer border of the first rib to the lower border of the teres major muscle where it continuous as brachial artery. Using as a reference the pectoralis minor muscle, the axillary artery could be divided into three parts: the first part extends from the outer board of the first rib to the superior board of the pectoralis OPEN ACCESS minor muscle; the second part is entirely covered by the pectoralis minor muscle; and the third part extends from the inferior border of the pectoralis minor muscle to the lower board of the teres *Correspondence: major muscle [1]. -

Subcutaneous Superficial Palmar Arch – an Unusual Variant
eISSN 1308-4038 International Journal of Anatomical Variations (2015) 8: 26–29 Case Report Subcutaneous superficial palmar arch – an unusual variant Published online November 30th, 2015 © http://www.ijav.org Sushama Kalidas CHAVAN Abstract Rajendra Namdeo WABALE Superficial palmar arch is the source of blood supply to hand. Formed by continuation of ulnar artery and completed usually by superficial branch of radial artery. The arch lies deep to the palmar aponeurosis. In our routine dissection for students, we came across an unusual variant of superficial palmar arch in the right hand. It was present in a plane. The branching pattern Department of Anatomy, Rural Medical College, Pravara was also variable showing four common palmar digital branches. The case along with its Institute of Medical Sciences, Loni, Ahmednagar, INDIA. embryological basis and clinical relevance is discussed. © Int J Anat Var (IJAV). 2015; 8: 26–29. Dr. Mrs. Sushama Kalidas Chavan Department of Anatomy Rural Medical College Loni Ahmednagar (M) INDIA. +91 9552033318 [email protected] Received January 30th, 2014; accepted August 9th, 2014 Key words [superficial palmar arch] [palmar aponeurosis] [common palmar digital arteries] Introduction branching pattern. We have come across a variation of SPA not Arterial arches of hand are the major blood supply to the recorded till date and we considered it as important to put in structures in the hand. The two arches, superficial and deep the record of literature. palmar arches make an important anastomose between the radial and ulnar arteries. Superficial palmar arch (SPA) is Case Report formed by direct continuation of ulnar artery, i.e. -

Occult Elbow Dislocation with Brachial Artery Injury Kazuo Ikeda* and Naoki Osamura Department of Orthopaedic Surgery, Kanazawa Medical Center, Japan
ical C lin as C e f R Ikeda and Osamura, J Clin Case Rep 2014, 4:9 o l e a p DOI: 10.4172/2165-7920.1000420 n o r r t u s o J Journal of Clinical Case Reports ISSN: 2165-7920 Case Report Open Access Occult Elbow Dislocation with Brachial Artery Injury Kazuo Ikeda* and Naoki Osamura Department of Orthopaedic Surgery, Kanazawa Medical Center, Japan Keywords: Brachial artery; Surgery; Elbow dislocation was only discovered when general anaesthesia was administered in the operating room (Figure 3). The ulnar collateral ligament was Introduction immediately sutured using a suture anchor and the brachial artery was Although elbow dislocation is the second most frequent type of reconstructed by an end-to-end suture with a 3 cm resection of the dislocation in the human body, complications in the brachial artery damaged area. Directly after surgery, the anastomosis of the artery was are rare [1]. In addition, brachial artery injury due to elbow dislocation strong enough to endure the tension of elbow extension and an orthosis which is not discernible during the initial examination (occult of 30 degrees elbow flexion was applied. One week after surgery, a joint dislocation) is even more rare [2]. Since reduction of the dislocated apparatus which restricted lateral instability was applied in order to elbow has already happened to be taken place at the scene, it is difficult allow early motion of the elbow joint. The patient did not experience to detect the elbow dislocation or understand why brachial artery any complications such as intermittent claudication or gangrene of the occlusion has occurred when there is no damage to the bone or elbow hand and returned to his electric maintenance job of his original job joint structures. -
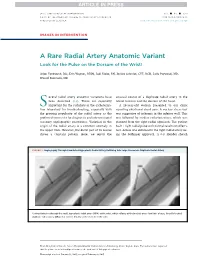
A Rare Radial Artery Anatomic Variant Look for the Pulse on the Dorsum of the Wrist!
JACC: CARDIOVASCULAR INTERVENTIONS VOL. - ,NO.- ,2017 ª 2017 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jcin.2017.02.026 IMAGES IN INTERVENTION A Rare Radial Artery Anatomic Variant Look for the Pulse on the Dorsum of the Wrist! Arjun Venkatesh, BSC, Erin Wagner, RT(R), Jodi Klebe, RN, Jessica Schmidt, CVT, RCIS, Laila Payvandi, MD, Wassef Karrowni, MD everal radial artery anatomic variations have unusual course of a duplicate radial artery in the S been described (1,2). These are especially lateral forearm and the dorsum of the hand. important for the radialists in the catheteriza- A56-year-oldwomanpresentedtoourclinic tion laboratory for troubleshooting, especially with reporting exertional chest pain. A nuclear stress test the growing popularity of the radial artery as the was suggestive of ischemia in the inferior wall. This preferred access site for diagnostic and interventional was followed by cardiac catheterization, which was coronary angiographic procedures. Variation in the planned from the right radial approach. The patient origin of the radial artery is a common anomaly in had 1þ right radial pulse with normal results on Allen’s the upper limb. However, the distal part of its course test. Access was obtained in the right radial artery us- shows a constant pattern. Here, we report the ing the Seldinger approach. A 6-F Slender sheath FIGURE 1 Angiography Through CannulatedHypoplasticRadialArteryRefluxing Into Large Anomalous Duplicate Radial Artery Contrast injection through the small, hypoplastic radial artery (HRA) at the wrist, which refluxes at the brachial artery level into a large, laterally located duplicate radial artery (DRA) that crosses distally to the dorsum of the wrist. -

An Anatomical Study of Variations in Termination of Brachial Artery, with Its Embryological Basis and Clinical Significance
Available online at www.ijmrhs.com International Journal of Medical Research & ISSN No: 2319-5886 Health Sciences, 2016, 5, 3:85-89 An anatomical study of variations in termination of brachial artery, with its embryological basis and clinical significance *Deepa T. K. and Martin K. John Assistant Professor, Department of Anatomy, MES Medical College, Perinthalmanna, Kerala *Corresponding Email: [email protected] _____________________________________________________________________________________________ ABSTRACT The brachial artery is the main artery of the arm. It begins as the continuation of 3 rd part of axillary artery, at the level of inferior border of teres major muscle. It ends at the level of the neck of radius by dividing into radial and ulnar arteries. In the present study we found higher division of brachial artery at mid arm level into its terminal branches with superficial course of radial artery. The present study was done on 51 cadavers from our dept. of Anatomy. The upper limbs of the cadaver were dissected and observed for any variations in the branching pattern of brachial artery. In the present study, a total number of 51 cadaver’s, 102 upper limbs were studied. In one male cadaver we found bilateral higher division of brachial artery, trifurcation on left side and bifurcation on right side brachial artery, with superficial course of radial artery. The knowledge of variation in origin and course of brachial artery is useful for orthopaedicians, physicians, radiologist, vascular and plastic surgeons. Key words : brachial artery, higher trifurcation & bifurcation, superficial radial artery _____________________________________________________________________________________________ INTRODUCTION The brachial artery provides the main arterial supply to the arm.