Pharmacology/Therapeutics I Block I Lectures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Zebrafish Behavioral Profiling Links Drugs to Biological Targets and Rest/Wake Regulation
www.sciencemag.org/cgi/content/full/327/5963/348/DC1 Supporting Online Material for Zebrafish Behavioral Profiling Links Drugs to Biological Targets and Rest/Wake Regulation Jason Rihel,* David A. Prober, Anthony Arvanites, Kelvin Lam, Steven Zimmerman, Sumin Jang, Stephen J. Haggarty, David Kokel, Lee L. Rubin, Randall T. Peterson, Alexander F. Schier* *To whom correspondence should be addressed. E-mail: [email protected] (A.F.S.); [email protected] (J.R.) Published 15 January 2010, Science 327, 348 (2010) DOI: 10.1126/science.1183090 This PDF file includes: Materials and Methods SOM Text Figs. S1 to S18 Table S1 References Supporting Online Material Table of Contents Materials and Methods, pages 2-4 Supplemental Text 1-7, pages 5-10 Text 1. Psychotropic Drug Discovery, page 5 Text 2. Dose, pages 5-6 Text 3. Therapeutic Classes of Drugs Induce Correlated Behaviors, page 6 Text 4. Polypharmacology, pages 6-7 Text 5. Pharmacological Conservation, pages 7-9 Text 6. Non-overlapping Regulation of Rest/Wake States, page 9 Text 7. High Throughput Behavioral Screening in Practice, page 10 Supplemental Figure Legends, pages 11-14 Figure S1. Expanded hierarchical clustering analysis, pages 15-18 Figure S2. Hierarchical and k-means clustering yield similar cluster architectures, page 19 Figure S3. Expanded k-means clustergram, pages 20-23 Figure S4. Behavioral fingerprints are stable across a range of doses, page 24 Figure S5. Compounds that share biological targets have highly correlated behavioral fingerprints, page 25 Figure S6. Examples of compounds that share biological targets and/or structural similarity that give similar behavioral profiles, page 26 Figure S7. -

Annual Report 2013
Annual Report 2013 “ Being active and having a positive outlook on life is what keeps me going every day.” Overview of 2013 “ Our performance in 2013 was defined by remarkable &R D output and further delivery of sustained financial performance for our shareholders.” Please go to page 4 for more More at gsk.com Performance highlights £26.5bn £8.0bn £7.0bn £5.2bn Group turnover Core* operating profit Total operating profit Returned to shareholders 6 112.2p 112.5p 13% Major medicines approved Core* earnings per share Total earnings per share Estimated return on R&D investment 10 6 1st 1st Potential phase III study starts in 2014/15 Potential medicines with phase III data in Access to Medicines Index Pharmaceutical company to sign AllTrials expected 2014/15 campaign for research transparency Front cover story Betty, aged 65, (pictured) has Chronic “ Health is important to me, Obstructive Pulmonary Disease (COPD). She only has 25% lung capacity. This means I try to take care of my she finds even everyday tasks difficult, but medicines and inhaled oxygen allow her to health with all the tools live as normal a life as she can. Betty’s mindset I have and do the best is to stay busy and active, so every week she goes to rehab exercise classes. that I can with it.” COPD is a disease of the lungs that leads to Betty, COPD patient, damaged airways, causing them to become North Carolina, USA narrower and making it harder for air to get in and out. 210 million people around the world are estimated to have COPD. -

Evaluation of the Anticonvulsant Activity of the Seed Acetone Extract of Ferula Gummosa Boiss
Journal of Ethnopharmacology 82 (2002) 105Á/109 www.elsevier.com/locate/jethpharm Evaluation of the anticonvulsant activity of the seed acetone extract of Ferula gummosa Boiss. against seizures induced by pentylenetetrazole and electroconvulsive shock in mice Mohammad Sayyah a,*, Ali Mandgary a, Mohammad Kamalinejad b a Department of Physiology and Pharmacology, Institute Pasteur of Iran, Tehran, Iran b Department of Pharmacognosy, Faculty of Pharmacy, Shaheed Beheshti University of Medical Sciences, Tehran, Iran Received 6 February 2002; received in revised form 11 May 2002; accepted 6 June 2002 Abstract Ferula gummosa Boiss. (Apiaceae) which has been used as an antiepileptic remedy in Iranian traditional medicine was evaluated for anticonvulsant activity against experimental seizures. The seed acetone extract of F. gummosa protected mice against tonic convulsions induced by maximal electroshock (the median effective dose [ED50]/198.3 mg/kg) and especially by pentylenetetrazole (ED50 /55 mg/kg). Neurotoxicity (sedation and motor impairment) of the extract was assessed by the rotarod test and the median toxic dose (TD50) value of 375.8 mg/kg was obtained. Preliminary phytochemical analysis showed the presence of terpenoids and alkaloids in the extract. The acceptable acute toxicity of the extract recommends further studies to determine the mechanism(s) and compound(s) involved in the anticonvulsant activity. # 2002 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Ferula gummosa; Seizure; Maximal electroshock; Pentylenetetrazole 1. Introduction several seed extracts of F. gummosa against seizures induced by maximal electroshock (MES) or pentylene- Ferula gummosa Boiss. (Apiaceae) is a perennial plant tetrazole (PTZ). In order to evaluate the therapeutic native to central Asia, growing in the northern and value and safety, the neurotoxicity (sedation and motor western parts of Iran (Zargari, 1989). -

L. Gel Against Sulphur Mustard- Induced Systemic Toxicity and Skin Lesions
Research Paper Protective effect of Aloe vera L. gel against sulphur mustard- induced systemic toxicity and skin lesions G. Anshoo, S. Singh, A.S. Kulkarni, S.C. Pant, R. Vijayaraghavan ABSTRACT Objective: Sulphur mustard (SM), chemically 2,2'-dichloro diethyl sulphide, is an incapacitating and extremely toxic chemical warfare agent, and causes serious blisters on contact with human skin. SM forms sulphonium ion in the body that alkylates DNA and several other macromolecules, and induces oxidative stress. The aim of this study was to evaluate the protective effect of Aloe vera Defence Research L. gel against SM-induced systemic toxicity and skin lesions. and Development Materials and Methods: Aloe vera gel was given (250, 500 and 1000 mg/kg) orally to mice as three Establishment, doses, one immediately after SM administration by percutaneous route, and the other two doses on Gwalior – 474002. the next two days. Protective index was calculated with and without Aloe vera gel treatment. Aloe India vera gel was also given orally as three doses with 3 LD50 SM and the animals were sacrificed for Received: 8.7.2004 biochemical and histological evaluation, 7 days after SM administration. In another set of experi- Revised: 20.9.2004 ment Aloe vera gel was liberally applied on the SM administered skin site and the animals were Accepted: 29.9.2004 sacrificed after 14 days to detect its protective effect on the skin lesions induced by SM. Results: The protection given by Aloe vera gel was marginal. 1000 mg/kg dose of Aloe vera gel gave a protection index of 2.8. -
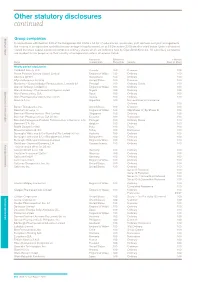
Other Statutory Disclosures Continued
Other statutory disclosures continued Strategic reportGroup companies Governance & remuneration Financial statements In accordance with Section 409 of the Companies Act 2006 a full list of subsidiaries, associates, joint ventures and joint arrangements, the country of incorporation and effective percentage of equity owned, as at 31 December 2015 are disclosed below. Unless otherwise stated the share capital disclosed comprises ordinary shares which are indirectly held by GlaxoSmithKline plc. All subsidiary companies are resident for tax purposes in their country of incorporation unless otherwise stated. Country of Effective % % Held by Name incorporation Ownership Security Class of Share Wholly owned subsidiaries 1506369 Alberta ULC Canada 100 Common 100 Action Potential Venture Capital Limited England & Wales 100 Ordinary 100 Adechsa GmbH Switzerland 100 Ordinary 100 Affymax Research Institute United States 100 Common 100 Alenfarma – Especialidades Farmaceuticas, Limitada (iv) Portugal 100 Ordinary Quota 100 Allen & Hanburys Limited (iv) England & Wales 100 Ordinary 100 Allen & Hanburys Pharmaceutical Nigeria Limited Nigeria 100 Ordinary 100 Allen Farmaceutica, S.A. Spain 100 Ordinary 100 Allen Pharmazeutika Gesellschaft m.b.H. Austria 100 Ordinary 100 Aners S.A (iv) Argentina 100 Non-endorsable Nominative Ordinary 100 Barrier Therapeutics, Inc. United States 100 Common 100 Beecham Group p l c England & Wales 100 20p Shares 'A'; 5p Shares B 100 Beecham Pharmaceuticals (Pte) Limited Singapore 100 Ordinary 100 Beecham Pharmaceuticals S.A (iv) (vi) Ecuador 100 Nominative 100 Beecham Portuguesa-Produtos Farmaceuticos e Quimicos, Lda Portugal 100 Ordinary Quota 100 Beecham S.A. (iv) Belgium 100 Ordinary 100 Biddle Sawyer Limited India 100 Equity 100 Biovesta Ilaçlari Ltd. Sti. Turkey 100 Nominative 100 Burroughs Wellcome & Co (Australia) Pty Limited (iv) (vi) Australia 100 Ordinary 100 Burroughs Wellcome & Co (Bangladesh) Limited Bangladesh 100 Ordinary 100 Burroughs Wellcome International Limited England & Wales 100 Ordinary 100 Caribbean Chemical Company, Ltd. -

Clinical Guidelines for Use of Depot Buprenorphine (Buvidal®
Clinical guidelines for use of depot buprenorphine (Buvidal® and Sublocade®) in the treatment of opioid dependence NSW Ministry of Health 100 Christie Street ST LEONARDS NSW 2065 Tel. (02) 9391 9000 Fax. (02) 9391 9101 TTY. (02) 9391 9900 www.health.nsw.gov.au Produced by: NSW Ministry of Health Lintzeris N, Dunlop A, Masters D (2019) Clinical guidelines for use of depot buprenorphine (Buvidal® and Sublocade®) in the treatment of opioid dependence. NSW Ministry of Health, Sydney Australia This work is copyright. It may be reproduced in whole or in part for study or training purposes subject to the inclusion of an acknowledgement of the source. It may not be reproduced for commercial usage or sale. Reproduction for purposes other than those indicated above requires written permission from the NSW Ministry of Health. © NSW Ministry of Health 2019 SHPN (CPH) 190431 ISBN 978-1-76081-226-3 Further copies of this document can be downloaded from the NSW Health website www.health.nsw.gov.au August 2019 ii NSW Health Use of depot BPN in the treatment of opioid dependence Authors Professor Nicholas Lintzeris (BMedSci MBBS PhD FAChAM) Director Drug and Alcohol Services, South East Sydney Local Health District Discipline Addiction Medicine, Faculty of Medicine and Health Sciences, University of Sydney NSW Drug and Alcohol Clinical Research and Improvement Network Professor Adrian Dunlop (MBBS, PhD, GdipEpiBiotat, FAChAM) Director Drug and Alcohol Clinical Services, Hunter New England Local Health District School of Medicine and Public Health, Faculty -

Multidisciplinary Approaches to Modern Therapeutics: Joining Forces for a Healthier Tomorrow
Available Online at www.jptcp.com www.cjcp.ca/ ABSTRACTS / RÉSUMÉS Multidisciplinary Approaches to Modern Therapeutics: Joining Forces for a Healthier Tomorrow May 24-27, 2011 Montreal, QC Canadian Society of Pharmacology and Therapeutics La Société canadienne de Pharmacologie et de Therapeutique J Popul Ther Clin Pharmacol Vol 18(2):e315-e363; May 22, 2011 e315 © 2011 Canadian Society of Clinical Pharmacology and Therapeutics. All rights reserved. 2011 CSPT ANNUAL CONFERENCE - ABSTRACTS Contents (Presenters are underlined) Oral Presentations May 26, 2011……………………………………………………………………………..e317 Poster Presentations May 25, 2011……………………………………………………………………………...e320 Poster Presentations May 26, 2011………………………………………………………………………………e338 e316 J Popul Ther Clin Pharmacol Vol 18 (2):e315-e363; May 22, 2011 © 2011 Canadian Society of Clinical Pharmacology and Therapeutics. All rights reserved. 2011 CSPT ANNUAL CONFERENCE - ABSTRACTS ORAL PRESENTATIONS 1Department of Physiology and Pharmacology and 2 THURSDAY - MAY 26, 2011 Division of Clinical Pharmacology, Department of Medicine, The University of Western Ontario, London, Ontario, Canada 1 Corresponding Author: [email protected] Effect of human equilibrative nucleoside Conflict of Interest: None declared transporter 1 (hENT1) expression on adenosine production from neurons Background: The HMG-CoA reductase inhibitors, or Chu S, Parkinson FE statins, are widely prescribed to reduce cardiovascular Department of Pharmacology and Therapeutics, disease risk. There is considerable interindividual University of Manitoba, Winnipeg, Canada variation in statin exposure and response arising from Corresponding Author: [email protected] variability in both transport and metabolism. Conflict of Interest: None declared Objective: Our aim was to better understand the in vivo relevance of the organic anion-transporting Background: Adenosine is produced in brain under polypeptide (OATP) 1B family to atorvastatin (ATV), ischemic conditions. -

Glaxosmithkline Plc Annual Report for the Year Ended 31St December 2000
GlaxoSmithKline 01 GlaxoSmithKline plc Annual Report for the year ended 31st December 2000 Contents Report of the Directors 02 Financial summary 03 Joint statement by the Chairman and the Chief Executive Officer 05 Description of business 29 Corporate governance 37 Remuneration report 47 Operating and financial review and prospects 69 Financial statements 70 Directors’ statements of responsibility 71 Report by the auditors 72 Consolidated statement of profit and loss 72 Consolidated statement of total recognised gains and losses 74 Consolidated statement of cash flow 76 Consolidated balance sheet 76 Reconciliation of movements in equity shareholders’ funds 77 Company balance sheet 78 Notes to the financial statements 136 Group companies 142 Principal financial statements in US$ 144 Financial record 153 Investor information 154 Shareholder return 156 Taxation information for shareholders 157 Shareholder information 158 Share capital 160 Cross reference to Form 20-F 162 Glossary of terms The Annual Report was approved by the Board 163 Index of Directors on 22nd March 2001 and published on 12th April 2001. Contact details 02 GlaxoSmithKline Financial summary 2000 1999 Increase Business performance £m £m CER % £ % Sales 18,079 16,164 9 12 Trading profit 5,026 4,378 12 15 Profit before taxation 5,327 4,708 11 13 Earnings/Net income 3,697 3,222 13 15 Earnings per Ordinary Share 61.0p 52.7p 14 16 Total results Profit before taxation 6,029 4,236 Earnings/Net income 4,154 2,859 Earnings per Ordinary Share 68.5p 46.7p Business performance: results exclude merger items and restructuring costs; 1999 sales and trading profit exclude the Healthcare Services businesses which were disposed of in 1999. -

Pharmacokinetics of Pancreatic Polypeptide in Man
Gut: first published as 10.1136/gut.19.10.907 on 1 October 1978. Downloaded from Gut, 1978, 19, 907-909 Pharmacokinetics of pancreatic polypeptide in man T. E. ADRIAN, G. R. GREENBERG, H. S. BESTERMAN, AND S. R. BLOOM From the Department ofMedicine, Royal Postgraduate Medical School, Hammersmith Hospital, London SUMMARY Pure bovine pancreatic polypeptide (PP) was infused into 23 healthy subjects at doses of 1, 3, and 5 pmol/kg/min over 60 minutes and plasma PP was measured by radioimmunoassay. During the infusions mean plasma levels of 203 + 34, 575 + 73, and 930 ± 48 pmol/l respectively were achieved. Mean disappearance half time on stopping the infusion was 6-9 + 0 3 min (mean + SEM). The metabolic clearance rate was 5-1 + 0-2 ml/kg/min (mean + SEM) and the apparent volume of distribution was calculated to be 51 ± 3 ml/kg (mean ± SEM). This study provides for the first time pharmacokinetic data for PP in man. Pancreatic polypeptide (PP) is a recently discovered syringe ram pump for a basal period of 30 minutes. hormonal 36 amino acid peptide localised in an BPP was then added to the infusion at nominal endocrine cell of the mammalian and avian pancreas doses of 1 (n = 6), 3 (n = 9), and 5 (n = 8) pmol/ (Kimmel et al., 1968; Lin and Chance, 1972). PP cir- kg/min. culates in plasma and levels rise substantially on the Blood samples were collected in chilled tubes with ingestion of a meal and remain raised for several 10 units heparin and 400 KIU aprotinin (Trasylol) hours (Adrian et al., 1976; Floyd et al., 1976; per ml, centrifuged, and the plasma frozen within 15 Schwartz et al., 1976). -

Chemoinformatics in Drug Design. Artificial Neural Networks for Simultaneous Prediction of Anti-Enterococci Activities and Toxicological Profiles
Chemoinformatics in Drug Design. Artificial Neural Networks for Simultaneous Prediction of Anti-enterococci Activities and Toxicological Profiles Alejandro Speck-Planche and M. N. D. S. Cordeiro REQUIMTE/Department of Chemistry and Biochemistry, University of Porto, 4169-007 Porto, Portugal Keywords: Artificial Neural Networks, Enterococci, Inhibitors, Toxicity, Topological Indices, mtk-QSBER, BC-3781. Abstract: Enterococci are dangerous opportunistic pathogens which are responsible of a huge number of nosocomial infections, displaying intrinsic resistance to many antibiotics. The battle against enterococci by using antimicrobial chemotherapies will depend on the design of new antibacterial agents with high activity and low toxicity. Multi-target methodologies focused on quantitative-structure activity relationships (mt- QSAR), have contributed to rationalize the process of drug discovery, improving the knowledge about the molecular patterns related with antimicrobial activity. Until know, almost all mt-QSAR models have considered the study of biological activity or toxicity separately. Here, we developed a unified mtk-QSBER (multitasking quantitative-structure biological effect relationships) model for simultaneous prediction of anti-enterococci activity and toxicity on laboratory animal and human immune cells. The mtk-QSBER model was created by using artificial neural network (ANN) analysis combined with topological indices, with the aim of classifying compounds as positive (high biological activity and/or low toxicity) or negative (otherwise) under multiple experimental conditions. The mtk-QSBER model correctly classified more than 90% of the whole dataset (more than 10900 cases). We used the model to predict multiple biological effects of the investigational drug BC-3781. Results demonstrate that our mtk-QSBER may represent a new horizon for the discovery of desirable anti-enterococci drugs. -

The Radioprotective Drugs Chosen for the First Phase of This Study Were
SUSTAINED-RELEASE OF RADIOPROTECTIVE AGENTS IN VITRO Jashovam Shani, Shimon Benita, Amram Samuni and Max Donbrow Departments of Pharmacology, Pharmacy and Molecular Biology, Hebrew University Medical School and School of Pharmacy, Jerusalem, Israel The major functional group of radioprotective agents contains a sulfur atom, either as a thiol (-SH) or in the oxidized state (-S-S-). These compounds protect against radiation as a result of their ability to trap primary free radicals formed via degradation radiolysis of water (1). The practical use of those radioprotectants is limited by their cumulative toxicity and rapid excretion and degradation. Moreover, for provision of adequate protection against irradiation effects, the concentration of the drug requires precise regulation, a difficult goal to achieve due to the rapidity of depletion on the one hand, and the low protective index on the other. Some protective doses and LD50 values for a highly effective radioprotective agent, cysteamine, in various mammalian species, are given in the following table (2): Species Route Protective Dose (mg/kg) LD50 (mg/kg) Mouse IP 75-150 260 Rat iP 75-150 140 Dog iv 75-110 Rabbit iv 150 Man iv 150-400 The radioprotective drugs chosen for the first phase of this study were cysteamine (g-mercaptoethylamine, H2N-CH2-CH2-SH) and cysteine (p-mercaptoalanine, H2N-CH(C00H)-CH2-SH), the most effective agents explored in mammals. The objective of this research is to improve the efficacy of these radioprotectants by development of new pharmaceutical formulations rather than by synthesis ing of new agents. With the growing use of nuclear enrgy throughout the world, and the risk of accidental irradiation becoming a dangerous hazard, we considered it desirable to develop a sustained-release radioprotec= tive formulation. -

Annual Report 2008 Find out More About GSK Online…
Do more, feel better, live longer Grow Deliver Simplify Annual Report 2008 Find out more about GSK online… www.gsk.com Website GlaxoSmithKline’s website www.gsk.com gives additional information on the Group. Information made available on the website does not constitute part of this Annual Report. Notice regarding limitations on Director liability under English Law Under the UK Companies Act 2006, a safe harbour limits the liability of Directors in respect of statements in and omissions from the Report of the Directors contained on pages 12 to 98. Under English law the Directors would be liable to the company (but not to any third party) if the Report of the Directors contains errors as a result of recklessness or knowing misstatement or dishonest concealment of a material fact, but would not otherwise be liable. Report of the Directors Pages 12 to 98 inclusive consist of a Report of the Directors that has been drawn up and presented in accordance with and in reliance upon English company law and the liabilities of the Directors in connection with that report shall be subject to the limitations and restrictions provided by such law. Cautionary statement regarding forward-looking statements The Group’s reports filed with or furnished to the US Securities and Exchange Commission (SEC), including this document and written information released, or oral statements made, to the public in the future by or on behalf of the Group, may contain forward-looking statements. Forward-looking statements give the Group’s current expectations or forecasts of future events. A shareholder can identify these statements by the fact that they do not relate strictly to historical or current facts.