A Dictionary of Hallucinations Jan Dirk Blom
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Blindsight in Man and Monkey
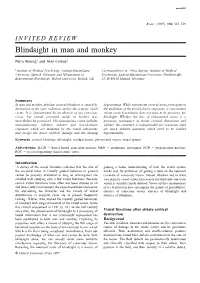
braini0301 Brain (1997), 120, 535–559 INVITED REVIEW Blindsight in man and monkey Petra Stoerig1 and Alan Cowey2 1Institute of Medical Psychology, Ludwig-Maximilians- Correspondence to: Petra Stoerig, Institute of Medical University, Munich, Germany and 2Department of Psychology, Ludwig-Maximilians-University, Goethestraβe Experimental Psychology, Oxford University, Oxford, UK 31, D-80336 Munich, Germany Summary In man and monkey, absolute cortical blindness is caused by degeneration. While extrastriate cortical areas participate in destruction of the optic radiations and/or the primary visual the mediation of the forced-choice responses, a concomitant cortex. It is characterized by an absence of any conscious striate cortical activation does not seem to be necessary for vision, but stimuli presented inside its borders may blindsight. Whether the loss of phenomenal vision is a nevertheless be processed. This unconscious vision includes necessary consequnce of striate cortical destruction and neuroendocrine, reflexive, indirect and forced-choice whether this structure is indispensable for conscious sight responses which are mediated by the visual subsystems are much debated questions which need to be tackled that escape the direct cerebral damage and the ensuing experimentally. Keywords: cortical blindness; blindsight; residual vision; phenomenal vision; visual system Abbreviations: dLGN 5 dorsal lateral geniculate nucleus; OKN 5 optokinetic nystagmus; PGN 5 pregeniculate nucleus; ROC 5 receiver-operating-characteristic curve Introduction ‘A survey of the recent literature indicates that the roˆle of gaining a better understanding of how the visual system the occipital lobes in visually guided behavior in general works and, by exclusion, of getting a hold on the neuronal cannot be properly evaluated as long as investigators are correlate of conscious vision. -

Mygland, Aali, Matre, Gilhus Spine, and One of Us (Lhermitte) Published
846 Mygland, Aali, Matre, Gilhus 14 Gautel M, Lakey A, Barlow DP, et al. Titin antibodies in 18 Mantegazza R, Beghi E, Pareyson D, et al. A multicentre myasthenia gravis: Identification of a major autogenic follow up study of 1152 patients with myasthenia gravis J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.57.7.846 on 1 July 1994. Downloaded from region of titin. Neurology 1994 (in press). in Italy. J Neurol 1990;237:339-44. 15 Grob D, Arsura EL, Brunner NG, Namba T. The course 19 Pagala MKD, Nandakumar NV, Venkatachari SAT, of myasthenia gravis and therapies affecting outcome. Ravindran K, Namba T, Grob D. Responses of inter- Ann NYAcad Sci 1987;505:472-99. costal muscle biopsies from normal subjects and 16 Oosterhuis HJGH. The natural course of mysthenia patients with myasthenia gravis. Muscle Nerve 1990;13: gravis: a long term follow up study. .J Neurol Neurosurg 1012-22. Psychiariy 1989;52:1 121-7. 20 Nielson VK, Paulson OB, Rosenkvist J, Holsoe E, Lefvert 17 Durelli L, Maggi G, Casadio C, Ferri R, Rendine S, AK. Rapid improvement of myasthenia gravis after Bergamini L. Actuarial analysis of the occurrence of plasma exchange. Ann Neurol 1982;11: 160-9. remissions following thymectomy for myasthenia gravis 21 Namba T, Brunner NG, Grob D. Idiopathic giant cell in 400 patients. Jf Neurol Neurosurg Psychiatry 1994;54: polymyositis: report of a case and review of the syn- 406-11. drome. Arch Neurol 1974;31:27-30. Jean Lhermitte 1877-1959 He showed the importance of the inferior olivary nucleus in myoclonus. -

Demonic Possession by Jean Lhermitte
G Model ENCEP-991; No. of Pages 5 ARTICLE IN PRESS L’Encéphale xxx (2017) xxx–xxx Disponible en ligne sur ScienceDirect www.sciencedirect.com Commentary Demonic possession by Jean Lhermitte Possession diabolique par Jean Lhermitte a b c,∗ E. Drouin , T. Péréon , Y. Péréon a Centre des hautes études de la Renaissance, université de Tours, 37000 Tours, France b Pôle hospitalo-universitaire de psychiatrie adulte, centre hospitalier Guillaume-Régnier, 35703 Rennes, France c Centre de référence maladies neuromusculaires Nantes–Angers, laboratoire d’explorations fonctionnelles, Hôtel-Dieu, CHU de Nantes, 44093 Nantes cedex, France a r t i c l e i n f o a b s t r a c t Article history: The name of the French neurologist and psychiatrist Jean Lhermitte (1877–1959) is most often associ- Received 13 September 2016 ated with the sign he described back in 1927 in three patients with multiple sclerosis. We are reporting Accepted 13 March 2017 unpublished handwritten notes by Jean Lhermitte about ‘demonic possession’, which date from the 1950s. Available online xxx Drawing from his experiences in neuropsychiatry, Lhermitte gathered notable case reviews as well as individual case histories. For him, cases of demonic possession are of a psychiatric nature with social back- Keywords: ground exerting a strong influence. Like Freud did earlier, Lhermitte believes that the majority of those Demonopathy possessed people have been subjected to sexual trauma with scruples, often linked to religion. Demonic Handwritten notes possession cases were not so rare in the 1950s but their number has nowadays declined substantially with the development of modern psychiatry. -

Joseph Jumentié 1879-1928
Joseph Jumentié 1879-1928 Olivier Walusinski Médecin de famille 28160 Brou [email protected] Fig. 1. Joseph Jumentié à La Salpêtrière en 1910 (BIUsanté Paris, domaine public). Résumé Joseph Jumentié (1879-1928), par ses qualités de clinicien et sa sagacité d’anatomo- pathologiste, sut faire honneur à ses maîtres en neurologie, Jules Dejerine, Augusta Dejerine- Klumpke et Joseph Babiński. Leur notoriété a laissé dans l’ombre la collaboration précieuse que Jumentié leur a assurée. A côté d’une remarquable thèse de doctorat fixant la sémiologie des tumeurs de l’angle ponto-cérébelleux en 1911, ses nombreuses publications ont abordé tous les domaines de la neurologie. Nous présentons, à titre d’exemple, ses recherches concernant le cervelet, les tumeurs cérébrales et mettons en valeur l’aide fournie à Mme Dejerine dans l’identification des « faisceaux » des grandes voies cortico-spinales au niveau bulbo- protubérantiel par la technique des coupes sériées multiples. Cette évocation est précédée d’une brève biographie illustrée de photos, pour la plupart, inédites. 1 Jules Dejerine (1849-1917) et Joseph Babiński (1857-1932) sont des neurologues célèbres et reconnus mondialement. Leurs travaux n’auraient sans doute pas toute la valeur que nous leur accordons, s’ils n’avaient pas eu l’aide déterminante de collaborateurs compétents et zélés. Joseph Jumentié est l’un de ceux-ci, formé par ces deux maîtres de la neurologie auxquels il resta fidèlement très attaché. Leur célébrité, comme une ombre portée, a plongé dans l’oubli l’œuvre de Jumentié. C’est celle-ci que nous souhaitons remettre en lumière. Joseph Julien Jumentié est né le 28 octobre 1879 à Clermont-Ferrand d’un père Alfred Jumentié (1848-1909) professeur au lycée et d’une mère au foyer Mathilde Poisson (1852-1902). -

The Role of Motion Streaks in the Perception of the Kinetic Zollner Illusion
Journal of Vision (2012) 12(6):19, 1–14 http://www.journalofvision.org/content/12/6/19 1 The role of motion streaks in the perception of the kinetic Zollner illusion The School of Optometry and Vision Science, The University of New South Wales, Sieu K. Khuu Sydney, New South Wales $ In classic geometric illusions such as the Zollner illusion, vertical lines superimposed on oriented background lines appear tilted in the direction opposite to the background. In kinetic forms of this illusion, an object moving over oriented background lines appears to follow a titled path, again in the direction opposite to the background. Existing literature does not proffer a complete explanation of the effect. Here, it is suggested that motion streaks underpin the illusion; that the effect is a consequence of interactions between detectors tuned to the orientation of background lines and those sensing the motion streaks that arise from fast object motion. This account was examined in the present study by measuring motion-tilt induction under different conditions in which the strength or salience of motion streaks was attenuated: by varying object speed (Experiment 1), contrast (Experiment 2), and trajectory/length by changing the element life-time within the stimulus (Experiment 3). It was predicted that, as motion streaks become less available, background lines would less affect the perceived direction of motion. Consistent with this prediction, the results indicated that, with a reduction in object speed below that required to generate motion streaks (, 1.128/s), Weber contrast (, 0.125) and motion streak length (two frames) reduced or extinguished the motion-tilt-induction effect. -

Geometrical Optical Illusion Via Sub-Riemannian Geodesics in the Roto-Translation Group
Geometrical Optical Illusion via Sub-Riemannian Geodesics in the Roto-Translation Group B. Franceschiello1, A. Mashtakov2, G. Citti3, and A. Sarti4 1 Fondation Asile des Aveugles and Laboratory for Investigative Neurophisiology, Department of Radiology, CHUV - UNIL, Lausanne 2 Program Systems Institute of RAS, Russia, CPRC, 3 Department of Mathematics, University of Bologna, Italy 4 CAMS, Center of Mathematics, CNRS - EHESS,Paris, France [email protected], [email protected], [email protected], [email protected] Abstract. We present a neuro-mathematical model for geometrical op- tical illusions (GOIs), a class of illusory phenomena that consists in a mismatch of geometrical properties of the visual stimulus and its associ- ated percept. They take place in the visual areas V1/V2 whose functional architecture have been modelled in previous works by Citti and Sarti as a Lie group equipped with a sub-Riemannian (SR) metric. Here we ex- tend their model proposing that the metric responsible for the cortical connectivity is modulated by the modelled neuro-physiological response of simple cells to the visual stimulus, hence providing a more biologically plausible model that takes into account a presence of visual stimulus. Il- lusory contours in our model are described as geodesics in the new metric. The model is confirmed by numerical simulations, where we compute the geodesics via SR-Fast Marching. 1 Introduction Geometrical-optical illusions (GOIs) have been discovered in the XIX century by German psychologists (Oppel 1854 [50], Hering, 1878,[33]) and have been defined as situations in which there is an awareness of a mismatch of geometrical prop- erties between an item in the object space and its associated percept [68]. -

Computational Role of Disinhibition in Brain Function
COMPUTATIONAL ROLE OF DISINHIBITION IN BRAIN FUNCTION A Dissertation by YINGWEI YU Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY August 2006 Major Subject: Computer Science COMPUTATIONAL ROLE OF DISINHIBITION IN BRAIN FUNCTION A Dissertation by YINGWEI YU Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY Approved by: Chair of Committee, Yoonsuck Choe Committee Members, Ricardo Gutierrez-Osuna Thomas Ioerger Takashi Yamauchi Head of Department, Valerie E. Taylor August 2006 Major Subject: Computer Science iii ABSTRACT Computational Role of Disinhibition in Brain Function. (August 2006) Yingwei Yu, B.E., Beihang University, China Chair of Advisory Committee: Dr. Yoonsuck Choe Neurons are connected to form functional networks in the brain. When neurons are combined in sequence, nontrivial effects arise. One example is disinhibition; that is, inhibition to another inhibitory factor. Disinhibition may be serving an important purpose because a large number of local circuits in the brain contain disinhibitory connections. However, their exact functional role is not well understood. The objective of this dissertation is to analyze the computational role of dis- inhibition in brain function, especially in visual perception and attentional control. My approach is to propose computational models of disinhibition and then map the model to the local circuits in the brain to explain psychological phenomena. Several computational models are proposed in this dissertation to account for disinhibition. (1) A static inverse difference of Gaussian filter (IDoG) is derived to account explic- itly for the spatial effects of disinhibition. -

Color Afterimages in Autistic Adults
Color afterimages in autistic adults Article (Published Version) Maule, John, Stanworth, Kirstie, Pellicano, Elizabeth and Franklin, Anna (2018) Color afterimages in autistic adults. Journal of Autism and Developmental Disorders, 48 (4). pp. 1409-1421. ISSN 0162-3257 This version is available from Sussex Research Online: http://sro.sussex.ac.uk/id/eprint/61156/ This document is made available in accordance with publisher policies and may differ from the published version or from the version of record. If you wish to cite this item you are advised to consult the publisher’s version. Please see the URL above for details on accessing the published version. Copyright and reuse: Sussex Research Online is a digital repository of the research output of the University. Copyright and all moral rights to the version of the paper presented here belong to the individual author(s) and/or other copyright owners. To the extent reasonable and practicable, the material made available in SRO has been checked for eligibility before being made available. Copies of full text items generally can be reproduced, displayed or performed and given to third parties in any format or medium for personal research or study, educational, or not-for-profit purposes without prior permission or charge, provided that the authors, title and full bibliographic details are credited, a hyperlink and/or URL is given for the original metadata page and the content is not changed in any way. http://sro.sussex.ac.uk J Autism Dev Disord DOI 10.1007/s10803-016-2786-5 S.I. : LOCAL VS. GLOBAL PROCESSING IN AUTISM SPECTRUM DISORDERS Color Afterimages in Autistic Adults 1 1 2 1 John Maule • Kirstie Stanworth • Elizabeth Pellicano • Anna Franklin Ó The Author(s) 2016. -

© 2017 the American Academy of Neurology Institute. THE
THE ANIMATED MIND OF GABRIELLE LÉVY Peter J Koehler, MD, PhD, FAAN Zuyderland Medical Cente Heerlen, The Netherlands "Sa vie fut un exemple de labeur, de courage, d'énergie, de ténacité, tendus vers ce seul but, cette seule raison: le travail et le devoir à accomplir"1 [Her life was an example of labor, of courage, of energy, of perseverance, directed at that single target, that single reason: the work and the duty to fulfil] These are words, used by Gustave Roussy, days after the early death at age 48, in 1934, of his colleague Gabrielle Lévy. Eighteen years previously they had written their joint paper on seven cases of a particular familial disease that became known as Roussy-Lévy disease.2 In the same in memoriam he added "And I have to say that in our collaboration, in which my name was often mentioned with hers, it was almost always her first idea and the largest part was done by her". Who was this Gabrielle Lévy and what did she achieve during her short life? Gabrielle Lévy Gabrielle Charlotte Lévy was born on January 11th, 1886 in Paris.*,1,3 Her father was Emile Gustave Lévy (1844- 1912; from Colmar in the Alsace region, working in the textile branch), who had married Mina Marie Lang (1851- 1903; from Durmenach, also in the Alsace) in 1869. They had five children (including four boys), the youngest of whom was Gabrielle. At first she was interested in the arts, music in particular. Although not loosing that interest, she chose to study medicine and became a pupil of the well-known Paris neurologist Pierre Marie and his pupils (Meige, Foix, Souques, Crouzon, Laurent, Roussy and others), who had been professor of anatomic-pathology since 1907 and succeeded Dejerine at the chair of neurology ('maladies du système nerveux'; that had been created for Jean-Martin Charcot in 1882). -
Color Appearance Models Second Edition
Color Appearance Models Second Edition Mark D. Fairchild Munsell Color Science Laboratory Rochester Institute of Technology, USA Color Appearance Models Wiley–IS&T Series in Imaging Science and Technology Series Editor: Michael A. Kriss Formerly of the Eastman Kodak Research Laboratories and the University of Rochester The Reproduction of Colour (6th Edition) R. W. G. Hunt Color Appearance Models (2nd Edition) Mark D. Fairchild Published in Association with the Society for Imaging Science and Technology Color Appearance Models Second Edition Mark D. Fairchild Munsell Color Science Laboratory Rochester Institute of Technology, USA Copyright © 2005 John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England Telephone (+44) 1243 779777 This book was previously publisher by Pearson Education, Inc Email (for orders and customer service enquiries): [email protected] Visit our Home Page on www.wileyeurope.com or www.wiley.com All Rights Reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning or otherwise, except under the terms of the Copyright, Designs and Patents Act 1988 or under the terms of a licence issued by the Copyright Licensing Agency Ltd, 90 Tottenham Court Road, London W1T 4LP, UK, without the permission in writing of the Publisher. Requests to the Publisher should be addressed to the Permissions Department, John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England, or emailed to [email protected], or faxed to (+44) 1243 770571. This publication is designed to offer Authors the opportunity to publish accurate and authoritative information in regard to the subject matter covered. -

Proquest Dissertations
INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction Is dependent upon the quality of the copy subm itted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough. substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g.. maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher qualify 6” x 9” black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order. Bell & Howell Information and Leaming 300 North Zeeb Road. Ann Arbor. Ml 48106-1346 USA UMI800-521-0600 THE CONTAGION OFLIFE: ROSSETTI, PATER, WILDE, AND THE AESTHETICIST BODY DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Stephen Weninger, MA., M A., M Phil. ***** The Ohio State University 1999 Dissertation Committee: Approved By: Professor David G. -

Applying Emmert's Law to the Poggendorff Illusion
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Frontiers - Publisher Connector ORIGINAL RESEARCH published: 16 October 2015 doi: 10.3389/fnhum.2015.00531 Applying Emmert’s Law to the Poggendorff illusion Umur Talasli and Asli Bahar Inan* Department of Psychology, Atilim University, Ankara, Turkey The Poggendorff illusion was approached with a novel perspective, that of applying Emmert’s Law to the situation. The extensities between the verticals and the transversals happen to be absolutely equal in retinal image size, whereas the registered distance for the verticals must be smaller than that of the transversals due to the fact that the former is assumed to occlude the latter. This combination of facts calls for the operation of Emmert’s Law, which results in the shrinkage of the occluding space between the verticals. Since the retinal image shows the transversals to be in contact with the verticals, the shrinkage must drag the transversals inwards in the cortical representation in order to eliminate the gaps. Such dragging of the transversals produces the illusory misalignment, which is a dictation of geometry. Some of the consequences of this new explanation were tested in four different experiments. In Experiment 1, a new illusion, the tilting of an occluded continuation of an oblique line, was predicted and achieved. In Experiments 2 and 3, perceived nearness of the occluding entity was Edited by: manipulated via texture density variations and the predicted misalignment variations Baingio Pinna, were confirmed by using a between-subjects and within-subjects designs, respectively. University of Sassari, Italy In Experiment 4, tilting of the occluded segment of the transversal was found to vary in Reviewed by: Branka Spehar, the predicted direction as a result of being accompanied by the same texture cues used University of New South Wales, in Experiments 2 and 3.