Legislative Assembly of Alberta the 27Th Legislature Second Session
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Time for Growth Annual Report Issue: Seniors Discuss Vital Issues
Please complete member survey: P. 21-23 Vol. 44 No. 3 Serving Alberta’s Seniors since 1967 June-August, 2011 A time for growth Annual report issue: Seniors discuss vital issues Photos: Kathie Neu Organ Spring blossoms brighten the day as the ACA annual general meeting gets underway at the Golden Circle, Red Deer, right, May 31. 2 ACA News, June-August 2011 Board of Directors 2011-12 A registered charitable organization since 1967, the Alberta Council on Aging works to improve the quality of life for Seniors. ACA News is published by the Alberta Council on Aging. ACA Mission: To empower and educate Seniors and government to support the quality of life for Seniors and encourage their full Publisher & Editor: participation in all aspects of society ACA Executive Editorial Services: PRESIDENT REGION 4 BizEdmonton Inc. Gary Pool Norm Bezanson ACA News reserves the right to Morinville Edmonton condense, rewrite and reject 780-939-4842 1-888-423-9666 material. [email protected] [email protected] Deadline for submissions for our next issue is Sept. 30, 2011. TREASURER REGION 5 Frank Hoebarth Bev Hanes ACA Staff Calgary Red Deer Executive Director: 403-282-7986 1-888-423-9666 Gary Pool, acting [email protected] [email protected] Assistant to the Executive REGION 6 Director: Daniela Hiltebrand VICE-PRESIDENT Frank Hoebarth Director, Age-Friendly vacant Calgary Program Development: PAST PRESIDENT 403-282-7986 Kathie Neu Organ Floyd Sweet [email protected] Administrative Assistant: Vermilion Nadia Willigar 780-853-4252 REGION 7 [email protected] Murray Campbell Alberta Council on Aging Lethbridge Box 9, 11808 St. -

Public Accounts
Twenty-Seventh Legislature Second Session Report of the Standing Committee on Public Accounts Report on 2008 Activities February 2009 COMMITTEES OF THE LEGISLATIVE ASSEMBLY Standing Committee on Public Accounts 801 Legislature Annex Edmonton, AB T5K 1E4 (780) 644-8621 [email protected] www.assembly.ab.ca/committees/publicaccounts February, 2009 To the Honourable Ken Kowalski Speaker of the Legislative Assembly of the Province of Alberta The Standing Committee on Public Accounts of the Legislative Assembly of Alberta has the honour to submit this Report relating to its 2008 activities for consideration by the Legislative Assembly. (original signed by) Hugh MacDonald, MLA Edmonton-Gold Bar Chair Standing Committee on Public Accounts MEMBERS OF THE STANDING COMMITTEE ON PUBLIC ACCOUNTS 27th Legislature, First Session, 2008 Hugh MacDonald, MLA Chair Edmonton-Gold Bar (AL) Doug Griffiths, MLA Deputy Chair Battle River-Wainwright (PC) Carl Benito, MLA Mr. Naresh Bhardwaj, MLA Edmonton-Mill Woods (PC) Edmonton-Ellerslie (PC) Harry Chase, MLA Cal Dallas, MLA Calgary-Varsity (AL) Red Deer-South (PC) Jonathan Denis, MLA Wayne Drysdale, MLA Calgary-Egmont (PC) Grande Prairie-Wapiti (PC) Kyle Fawcett, MLA Broyce Jacobs, MLA Calgary-North Hill (PC) Cardston-Taber-Warner (PC) Jeff Johnson, MLA Darshan Kang, MLA Athabasca-Redwater (PC) Calgary-McCall (AL) Brian Mason, MLA Dave Quest, MLA Edmonton-Highlands-Norwood (ND) Strathcona (PC) Peter Sandhu, MLA Tony Vandermeer, MLA Edmonton-Manning (PC) Edmonton-Beverly-Clareview (PC) Teresa Woo-Paw, MLA Calgary-Mackay (PC) TABLE OF CONTENTS Page Number I. Introduction ................................................................................................ 1 II. Committee Activities .................................................................................. 2 III. Schedule of Standing Committee Meetings .............................................. 4 IV. Conference Attendance ............................................................................ -
Public Accounts
Twenty-Seventh Legislature Third Session Report of the Standing Committee on Public Accounts Report on 2009 Activities M a r c h 2 0 1 0 COMMITTEES OF THE LEGISLATIVE ASSEMBLY Standing Committee on Public Accounts 801 Legislature Annex 9718 – 107 Street Edmonton, AB T5K 1E4 780.644.8621 [email protected] www.assembly.ab.ca/committees/publicaccounts March, 2010 To the Honourable Ken Kowalski Speaker of the Legislative Assembly of the Province of Alberta The Standing Committee on Public Accounts of the Legislative Assembly of Alberta has the honour to submit this Report relating to its 2009 activities for consideration by the Legislative Assembly. Hugh MacDonald, MLA Edmonton-Gold Bar Chair Standing Committee on Public Accounts MEMBERS OF THE STANDING COMMITTEE ON PUBLIC ACCOUNTS 27th Legislature, Second Session, 2009 Hugh MacDonald, MLA Chair Edmonton-Gold Bar (AL) Dave Quest, MLA Deputy Chair Strathcona (PC) Carl Benito, MLA Naresh Bhardwaj, MLA Edmonton-Mill Woods (PC) Edmonton-Ellerslie (PC) Harry Chase, MLA Cal Dallas, MLA Calgary-Varsity (AL) Red Deer-South (PC) Jonathan Denis, MLA Wayne Drysdale, MLA Calgary-Egmont (PC) Grande Prairie-Wapiti (PC) Kyle Fawcett, MLA Broyce Jacobs, MLA Calgary-North Hill (PC) Cardston-Taber-Warner (PC) Jeff Johnson, MLA Darshan Kang, MLA Athabasca-Redwater (PC) Calgary-McCall (AL) Brian Mason, MLA Verlyn Olson, MLA Edmonton-Highlands-Norwood (ND) Wetaskiwin-Camrose (PC) Peter Sandhu, MLA Tony Vandermeer, MLA Edmonton-Manning (PC) Edmonton-Beverly-Clareview (PC) Teresa Woo-Paw, MLA Calgary-Mackay (PC) TABLE OF CONTENTS Page Number I. Introduction ................................................................................................ 1 II. Committee Activities .................................................................................. 2 III. Schedule of Standing Committee Meetings ............................................. -

P:\HANADMIN\BOUND\Committees\27Th Legislature\3Rd Session 2010\HE\HE Cover 101014.Wpd
Legislative Assembly of Alberta The 27th Legislature Third Session Standing Committee on Health Freedom of Information and Protection of Privacy Act Review Wednesday, October 13, 2010 9:30 a.m. Transcript No. 27-3-12 Legislative Assembly of Alberta The 27th Legislature Third Session Standing Committee on Health McFarland, Barry, Little Bow (PC), Chair Pastoor, Bridget Brennan, Lethbridge-East (AL), Deputy Chair Bhardwaj, Naresh, Edmonton-Ellerslie (PC)* Blakeman, Laurie, Edmonton-Centre (AL)** Forsyth, Heather, Calgary-Fish Creek (WA) Groeneveld, George, Highwood (PC) Horne, Fred, Edmonton-Rutherford (PC) Lindsay, Fred, Stony Plain (PC) Notley, Rachel, Edmonton-Strathcona (ND) Olson, Verlyn, QC, Wetaskiwin-Camrose (PC) Quest, Dave, Strathcona (PC) Sherman, Dr. Raj, Edmonton-Meadowlark (PC) Taft, Dr. Kevin, Edmonton-Riverview (AL) Vandermeer, Tony, Edmonton-Beverly-Clareview (PC) * substitution for Fred Horne ** substitution for Kevin Taft Department of Service Alberta Participants Cheryl Arseneau Director, Policy and Governance Di Nugent Director, Legislative and FOIP Services Office of the Information and Privacy Commissioner Participant Marylin Mun Assistant Commissioner Support Staff W.J. David McNeil Clerk Louise J. Kamuchik Clerk Assistant/Director of House Services Micheline S. Gravel Clerk of Journals/Table Research Robert H. Reynolds, QC Law Clerk/Director of Interparliamentary Relations Shannon Dean Senior Parliamentary Counsel/Clerk of Committees Corinne Dacyshyn Committee Clerk Jody Rempel Committee Clerk Karen Sawchuk Committee Clerk Rhonda Sorensen Manager of Corporate Communications and Broadcast Services Melanie Friesacher Communications Consultant Tracey Sales Communications Consultant Philip Massolin Committee Research Co-ordinator Stephanie LeBlanc Legal Research Officer Diana Staley Research Officer Rachel Stein Research Officer Liz Sim Managing Editor of Alberta Hansard Transcript produced by Alberta Hansard October 13, 2010 Health HE-669 9:30 a.m. -

Orange Chinook: Politics in the New Alberta
University of Calgary PRISM: University of Calgary's Digital Repository University of Calgary Press University of Calgary Press Open Access Books 2019-01 Orange Chinook: Politics in the New Alberta University of Calgary Press Bratt, D., Brownsey, K., Sutherland, R., & Taras, D. (2019). Orange Chinook: Politics in the New Alberta. Calgary, AB: University of Calgary Press. http://hdl.handle.net/1880/109864 book https://creativecommons.org/licenses/by-nc-nd/4.0 Attribution Non-Commercial No Derivatives 4.0 International Downloaded from PRISM: https://prism.ucalgary.ca ORANGE CHINOOK: Politics in the New Alberta Edited by Duane Bratt, Keith Brownsey, Richard Sutherland, and David Taras ISBN 978-1-77385-026-9 THIS BOOK IS AN OPEN ACCESS E-BOOK. It is an electronic version of a book that can be purchased in physical form through any bookseller or on-line retailer, or from our distributors. Please support this open access publication by requesting that your university purchase a print copy of this book, or by purchasing a copy yourself. If you have any questions, please contact us at [email protected] Cover Art: The artwork on the cover of this book is not open access and falls under traditional copyright provisions; it cannot be reproduced in any way without written permission of the artists and their agents. The cover can be displayed as a complete cover image for the purposes of publicizing this work, but the artwork cannot be extracted from the context of the cover of this specific work without breaching the artist’s copyright. COPYRIGHT NOTICE: This open-access work is published under a Creative Commons licence. -

Local Authorities Pension Plan Cost of Living
SENIORS UNITED NOW LOCAL AUTHORITIES PENSION PLAN COST OF LIVING ADVOCACY PROJECT IDENTIFY THE ISSUE: Alberta pensioners annual cost of living adjustment is currently based on only 60% of the Canadian consumer price index. For the average government pensioner this calculated to a 0.96% increase, which in dollars amounts to about a $10.00 monthly increase, resulting in a further fall behind of the real inflation rate. The Alberta Provincial Government promised cost of living adjustments to be comparable to the C.P.I. but continues to break this promise. A recent press release from the Local Authorities Pension Plan indicates the total elimination of the Cost of Living Adjustment! COST OF LIVING ADJUSTMENT STANDARDS SET BY OTHER PROVINCES: Following is a summary, obtained from Google, which outlines the COLA adjustment standards implemented by other Provincial Governments; British Columbia, over the last 25 years (except for one year) has provided COLA adjustments which provides increases at 100% of the Canadian Consumer Price Index. Manitoba, COLA is based on 2/3 of the C.P.I. Ontario, appears to be 100% of the C.P.I. Quebec, pensioners over the age of 65 receive 100% of the C.P.I. Newfoundland/Labrador, COLA is adjusted October of each year to 60% of the C.P.I. New Brunswick, has a “Shared Risk Pension Model”, as pension returns increase the higher the COLA is adjusted. Nova Scotia, if superannuation fund is insufficient , the Minister of Finance shall pay the shortfall out of General Revenue. Year 2011 to 2015 COLA is indexed at 1.25%. -
Alberta to Better Integrate Oil and Gas Policy and Regulatory System Regulatory Enhancement Task Force Delivers Report to Government
January 28, 2011 Alberta to better integrate oil and gas policy and regulatory system Regulatory Enhancement Task Force delivers report to government Calgary... Coordinated policy development and an integrated regulatory system for upstream oil and gas highlight a report from the task force established to review Alberta’s regulatory system. “I would like to thank Diana McQueen, Cal Dallas, and Evan Berger for their excellent work,” said Energy Minister Ron Liepert. “Government has accepted the report. The recommendations will now be immediately taken through the appropriate government review process for implementation. Legislation will be introduced this spring to begin implementation of the task force report.” The task force report and recommendations include: Establishing a new Policy Management Office and ensuring integration of natural resource policies; Creating a single oil and gas regulatory body; Providing clear public engagement processes; Using a common approach to risk assessment and management; Adopting performance measures to enable continuous system improvement; and Creating a mechanism to help resolve disputes between landowners and companies, and enforce agreements where required. “To maintain Alberta’s competitiveness the regulatory system must be effective, efficient, adaptable, predictable, fair and transparent,” said task force chair, Parliamentary Assistant for Energy Diana McQueen. “We will not compromise our responsibilities to environmental stewardship and the protection of public safety and public interests.” The review included analyses of all processes in place to develop and ensure compliance with provincial policies around upstream oil and gas development, and extensive engagement of First Nations, the oil and gas industry, and individuals from landowner, municipal, and environmental groups. Between March 31 and October 1, 2010 the task force hosted three rounds of engagement through a series of briefings, meetings, workshops and a forum. -

University of Lethbridge Alumnus Manwar Khan to Hold Anti-‐Bullying
For Immediate Release — Wednesday, August 12, 2015 University of Lethbridge alumnus Manwar Khan to hold Anti-Bullying Rally for victims of bullying and violence What: Do Not Be a Bystander Anti-Bullying Rally When: Saturday, August 15, 11:30 a.m. Where: Calgary City Hall – Municipal Plaza space Edmonton-based activist and University of Lethbridge alumnus Manwar Khan (BSc ’07), a father of twins, is holding a rally in Calgary at the Calgary City Hall as he continues to campaign across the province against bullying and violence. “We will be gathering in front of City Hall to show our support for every known and unknown victim of bullying and violence in Alberta,” says Khan, who witnessed a violent attack on an Edmonton LRT train in December 2012. It led to the death of one man and the incarceration of another. Khan invites everyone to gather at City Hall at 11:30 a.m. to rally in support of those who have been affected by violence and bullying. He is also asking people who are not able to attend the rally to leave their porch lights on from 6 to 7 p.m. on August 15, 2015 to show their support for the stand against violence and bullying. Khan established a series of anti-bullying rallies in 2013 and 2014, holding events in Edmonton, Calgary, Lethbridge and Airdrie. He has vowed to continue to represent victims of bullying and to try and stem the onset of violence so that it does not persist in society. “I believe firmly that it is a matter of great importance to teach our children that bullying is simply not acceptable in our society if we are to achieve safety and happiness for all,” he says. -
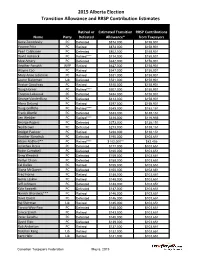
2015 Alberta Election Transition Allowance and RRSP Contribution Estimates
2015 Alberta Election Transition Allowance and RRSP Contribution Estimates Retired or Estimated Transition RRSP Contributions Name Party Defeated Allowance* from Taxpayers Gene Zwozdesky PC Defeated $874,000 $158,901 Yvonne Fritz PC Retired $873,000 $158,901 Pearl Calahasen PC Defeated $802,000 $158,901 David Hancock PC Retired**** $714,000 $158,901 Moe Amery PC Defeated $642,000 $158,901 Heather Forsyth WRP Retired $627,000 $158,901 Wayne Cao PC Retired $547,000 $158,901 Mary Anne Jablonski PC Retired $531,000 $158,901 Laurie Blakeman Lib Defeated $531,000 $158,901 Hector Goudreau PC Retired $515,000 $158,901 Doug Horner PC Retired**** $507,000 $158,901 Thomas Lukaszuk PC Defeated $484,000 $158,901 George VanderBurg PC Defeated $413,000 $158,901 Alana DeLong PC Retired $397,000 $158,901 Doug Griffiths PC Retired**** $349,000 $152,151 Frank Oberle PC Defeated $333,000 $138,151 Len Webber PC Retired**** $318,000 $116,956 George Rogers PC Defeated $273,000 $138,151 Neil Brown PC Defeated $273,000 $138,151 Bridget Pastoor PC Retired $238,000 $138,151 Heather Klimchuk PC Defeated $195,000 $103,651 Alison Redford** PC Retired**** $182,000** $82,456 Jonathan Denis PC Defeated $177,000 $103,651 Robin Campbell PC Defeated $160,000 $103,651 Greg Weadick PC Defeated $159,000 $103,651 Verlyn Olson PC Defeated $158,000 $103,651 Cal Dallas PC Retired $155,000 $103,651 Diana McQueen PC Defeated $150,000 $103,651 Fred Horne PC Retired $148,000 $103,651 Genia Leskiw PC Retired $148,000 $103,651 Jeff Johnson PC Defeated $148,000 $103,651 Kyle Fawcett -

Orange Chinook: Politics in the New Alberta
University of Calgary PRISM: University of Calgary's Digital Repository University of Calgary Press University of Calgary Press Open Access Books 2019-01 Orange Chinook: Politics in the New Alberta University of Calgary Press Bratt, D., Brownsey, K., Sutherland, R., & Taras, D. (2019). Orange Chinook: Politics in the New Alberta. Calgary, AB: University of Calgary Press. http://hdl.handle.net/1880/109864 book https://creativecommons.org/licenses/by-nc-nd/4.0 Attribution Non-Commercial No Derivatives 4.0 International Downloaded from PRISM: https://prism.ucalgary.ca ORANGE CHINOOK: Politics in the New Alberta Edited by Duane Bratt, Keith Brownsey, Richard Sutherland, and David Taras ISBN 978-1-77385-026-9 THIS BOOK IS AN OPEN ACCESS E-BOOK. It is an electronic version of a book that can be purchased in physical form through any bookseller or on-line retailer, or from our distributors. Please support this open access publication by requesting that your university purchase a print copy of this book, or by purchasing a copy yourself. If you have any questions, please contact us at [email protected] Cover Art: The artwork on the cover of this book is not open access and falls under traditional copyright provisions; it cannot be reproduced in any way without written permission of the artists and their agents. The cover can be displayed as a complete cover image for the purposes of publicizing this work, but the artwork cannot be extracted from the context of the cover of this specific work without breaching the artist’s copyright. COPYRIGHT NOTICE: This open-access work is published under a Creative Commons licence. -

P:\HANADMIN\BOUND\Committees
Legislative Assembly of Alberta The 27th Legislature Third Session Standing Committee on Resources and Environment Department of International and Intergovernmental Relations Consideration of Main Estimates Wednesday, March 10, 2010 6:30 p.m. Transcript No. 27-3-3 Legislative Assembly of Alberta The 27th Legislature Third Session Standing Committee on Resources and Environment Prins, Ray, Lacombe-Ponoka (PC), Chair Blakeman, Laurie, Edmonton-Centre (AL), Deputy Chair Anderson, Rob, Airdrie-Chestermere (WA) Berger, Evan, Livingstone-Macleod (PC) Boutilier, Guy C., Fort McMurray-Wood Buffalo (Ind) Dallas, Cal, Red Deer-South (PC) Hehr, Kent, Calgary-Buffalo (AL) Jacobs, Broyce, Cardston-Taber-Warner (PC) Mason, Brian, Edmonton-Highlands-Norwood (ND) McQueen, Diana, Drayton Valley-Calmar (PC) Mitzel, Len, Cypress-Medicine Hat (PC) VanderBurg, George, Whitecourt-Ste. Anne (PC) Weadick, Greg, Lethbridge-West (PC)* * substitution for George VanderBurg Also in Attendance Pastoor, Bridget Brennan, Lethbridge-East (AL) Department of International and Intergovernmental Relations Participant Hon. Iris Evans Minister Support Staff W.J. David McNeil Clerk Louise J. Kamuchik Clerk Assistant/Director of House Services Micheline S. Gravel Clerk of Journals/Table Research Robert H. Reynolds, QC Senior Parliamentary Counsel Shannon Dean Senior Parliamentary Counsel Corinne Dacyshyn Committee Clerk Jody Rempel Committee Clerk Karen Sawchuk Committee Clerk Rhonda Sorensen Manager of Communications Services Melanie Friesacher Communications Consultant Tracey Sales Communications Consultant Philip Massolin Committee Research Co-ordinator Stephanie LeBlanc Legal Research Officer Diana Staley Research Officer Rachel Stein Research Officer Liz Sim Managing Editor of Alberta Hansard Transcript produced by Alberta Hansard March 10, 2010 Resources and Environment RE-253 6:30 p.m. Wednesday, March 10, 2010 speak for alternating times of 10 minutes for a total of 20 minutes Title: Wednesday, March 10, 2010 RE per interaction. -

Premier Promotes Verlyn Olson and Greg Weadick to Cabinet Cal Dallas Becomes the New Parliamentary Assistant to Finance
February 17, 2011 Premier promotes Verlyn Olson and Greg Weadick to cabinet Cal Dallas becomes the new Parliamentary Assistant to Finance Edmonton... Premier Ed Stelmach announced today that Wetaskiwin-Camrose MLA Verlyn Olson, QC, has been named Minister of Justice and Attorney General, and Lethbridge West MLA Greg Weadick has been named Minister of Advanced Education and Technology. “I’m pleased to welcome Verlyn and Greg to the cabinet table,” said Premier Stelmach. “Verlyn and Greg bring the necessary talent and experience - Greg as a parliamentary assistant and Verlyn as a long-time member of the bar - to complete our cabinet team. Our cabinet will continue to provide the steady leadership required right now to continue building a better Alberta.” Premier Stelmach also named a new Parliamentary Assistant to the Minister of Finance and Enterprise. “I’m pleased that Red Deer South MLA Cal Dallas, who had been serving as the Parliamentary Assistant in Environment, will take over this important role and work closely with Finance Minister Lloyd Snelgrove,” said the Premier. Premier Stelmach also announced changes to committee memberships. Joining the Agenda and Priorities Committee are Sustainable Resource Development Minister Mel Knight, Children and Youth Services Minister Yvonne Fritz and Agriculture and Rural Development Minister Jack Hayden. New members of Treasury Board are Len Webber, Minister of Aboriginal Relations, Heather Klimchuk, Minister of Service Alberta, and Naresh Bhardwaj, MLA for Edmonton-Ellerslie. The new Cabinet members will be sworn in Friday, February 18 at 8:30 a.m. at Government House. Lloyd Snelgrove was sworn in as Minister of Finance and Enterprise on January 31.