Finnish Alcohol Policy at the Crossroads
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Income Tax (Einkommensteuer) 1
INVENTORY LEVIED IN THE MEMBER STATES OF THE EUROPEAN UNION 16th edition — Supplement AUSTRIA FINLAND SWEDEN * »* • • • • • *** EUROPEAN COMMISSION EUROPEAN COMMISSION DIRECTORATE-GENERAL XXI CUSTOMS AND INDIRECTTAXATION DIRECTORATE-GENERAL XV INTERNAL MARKET AND FINANCIAL SERVICES Inventory of taxes levied in the Member States of the European Union by the State and the local authorities (Lander, départements, regions, districts, provinces, communes) 16TH EDITION — Supplement Austria Finland Sweden DOCUMENT A great deal of additional information on the European Union is available on the Internet. It can be accessed through the Europa server (http://europa.eu.int) Cataloguing data can be found at the end of this publication Luxembourg: Office for Official Publications of the European Communities, 1996 ISBN 92-827-6986-0 © ECSC-EC-EAEC, Brussels · Luxembourg, 1996 Printed in Luxembourg Introductory note In collaboration with the Member States, the European Commission publishes a survey of the duties and taxes in force in the Member States of the European Union. The present edition reflects the situation on 1 January 1995 in Austria, Finland and Sweden and Is a supplement to the 16th edition. This publication aims to provide all those interested in tax law — public servants, university staff, students, businessmen, tax advisers, etc.—with a general view of the tax systems of the Member States. Directorates-General XXI and XV will be pleased to receive any comments or suggestions with a view to the improvement of this work. Rue de la Loi 200 B-1040 Brussels Abbreviations M.b. — Moniteur belge B.S. = Belgisch Staatsblad BGBl. = Bundesgesetzblatt VO = Verordnung BayBS = Bayrische Bereinigte Sammlung GVBI = Gesetz- und Verordnungsblatt RGBl = Reichsgesetzblatt RAO and AO = (Reichs). -

Government Monopoly As an Instrument for Public Health and Welfare Lessons for Cannabis from Experience with Alcohol Monopolies
International Journal of Drug Policy 74 (2019) 223–228 Contents lists available at ScienceDirect International Journal of Drug Policy journal homepage: www.elsevier.com/locate/drugpo Policy Analysis Government monopoly as an instrument for public health and welfare: T Lessons for cannabis from experience with alcohol monopolies ⁎ Robin Rooma,b, , Jenny Cisneros Örnbergb a Centre for Alcohol Policy Research, La Trobe University, Melbourne, Australia b Centre for Social Research on Alcohol and Drugs, Department of Public Health Sciences, Stockholm University, Stockholm, Sweden ARTICLE INFO ABSTRACT Keywords: Background: Government monopolies of markets in hazardous but attractive substances and activities have a Alcohol long history, though prior to the late 19th century often motivated more by revenue needs than by public health Cannabis and welfare. Government monopoly Methods: A narrative review considering lessons from alcohol for monopolization of all or part of legal markets Market control in cannabis as a strategy for public health and welfare. Control system Results: A monopoly can constrain levels of use and harm from use through such mechanisms as price, limits on times and places of availability, and effective implementation of restrictions on who can purchase, andless directly by replacing private interests who would promote sales and press for greater availability, and as a potential test-bed for new policies. But such monopolies can also push in the opposite direction, particularly if revenue becomes the prime consideration. Drawing on the alcohol experience in recent decades, the paper discusses issues relevant to cannabis legalization in monopolization of different market levels and segments – production, wholesale, import, retail for off-site and for on-site use – and choices about the structuring and governance of monopolies and their organizational location in government, from the perspective of maximizing public health and welfare interests. -

Statement on the Corporate Governance and Steering System 2016 Finnvera’S Financial Review 2016 2
Statement on the Corporate Governance and Steering System 2016 FINNVERA’s FinanciaL REVIEW 2016 2 Statement on the Corporate Governance and Steering System Finnvera’s Financial Review 2016 Statement on the Corporate Governance and Steering System Contents Statement on the Corporate Governance and Steering System .............. 3 Acts and rules governing the operations ........................................... 3 The goals of good corporate governance ........................................... 3 Ownership and ownership policy ..................................................... 4 Administrative bodies of Finnvera ........................................ ........... 4 General Meeting of Shareholders ........................................ 4 Supervisory Board ............................................................ 4 Board of Directors ............................................................ 5 Inspection Committee of the Board of Directors ..................... 7 Remuneration Committee of the Board of Directors ................ 7 Chief Executive Officer, Management Group and Corporate Management Team ............................................. 8 Salaries and fees .......................................................................... 8 Operating principles for internal control ............................................ 9 Risk management ......................................................................... 9 Controlling the financial reporting process ........................................ 9 Compliance function ..................................................................... -

Regulator\ Reform in Finland
5HJXODWRU\ 5HIRUP LQ )LQODQG 7KH 5ROH RI &RPSHWLWLRQ 3ROLF\ LQ 5HJXODWRU\ 5HIRUP ORGANISATION FOR ECONOMIC CO-OPERATION AND DEVELOPMENT Pursuant to Article 1 of the Convention signed in Paris on 14th December 1960, and which came into force on 30th September 1961, the Organisation for Economic Co-operation and Development (OECD) shall promote policies designed: to achieve the highest sustainable economic growth and employment and a rising standard of living in Member countries, while maintaining financial stability, and thus to contribute to the development of the world economy; to contribute to sound economic expansion in Member as well as non-member countries in the process of economic development; and to contribute to the expansion of world trade on a multilateral, non-discriminatory basis in accordance with international obligations. The original Member countries of the OECD are Austria, Belgium, Canada, Denmark, France, Germany, Greece, Iceland, Ireland, Italy, Luxembourg, the Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, Turkey, the United Kingdom and the United States. The following countries became Members subsequently through accession at the dates indicated hereafter: Japan (28th April 1964), Finland (28th January 1969), Australia (7th June 1971), New Zealand (29th May 1973), Mexico (18th May 1994), the Czech Republic (21st December 1995), Hungary (7th May 1996), Poland (22nd November 1996), Korea (12th December 1996) and the Slovak Republic (14th December 2000). The Commission of the European Communities takes part in the work of the OECD (Article 13 of the OECD Convention). Publié en français sous le titre : LE ROLE DE LA POLITIQUE DE LA CONCURRENCE DANS LA RÉFORME DE LA RÉGLEMENTATION © OECD 2003. -
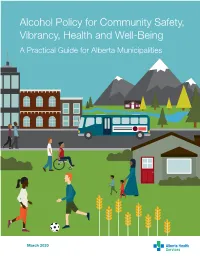
Alcohol Policy for Community Safety, Vibrancy, Health and Well-Being a Practical Guide for Alberta Municipalities
Alcohol Policy for Community Safety, Vibrancy, Health and Well-Being A Practical Guide for Alberta Municipalities March 2020 This guide was developed by Provincial Addiction Prevention, Alberta Health Services. This edition was completed March 13, 2020. The Project team included Leslie Munson, Shiela Bradley, Z’Anne Harvey-Jansen and Teresa Curtis. To cite this guide: Alberta Health Services. (2020). Alcohol policy for community safety, vibrancy, health and well-being: A practical guide for Alberta municipalities. Calgary, AB: Author. For more information or to request print or digital copy, please contact AHS Provincial Addiction Prevention at [email protected]. The Canadian Institute for Substance Use Research gave Alberta Health Services (AHS) permission to reproduce sections of Helping Municipal Governments Reduce Alcohol-Related Harms: Limiting Alcohol Availability, Ensuring Safer Drinking Environments, Reducing Drinking and Driving, Limiting Alcohol Availability, Strengthening the Community, and Advocating to Other Levels of Government for this guide. The Nova Scotia Health Authority gave AHS permission to reproduce sections of Municipal Alcohol Policies: Options for Nova Scotia Municipalities for this guide. Finally, the Nova Scotia Federation of Municipalities (formerly the Union of Nova Scotia Municipalities) gave AHS permission to reproduce sections of Progressive and Prosperous: Municipal Alcohol Policies for a Balanced and Vibrant Future, A Municipal Alcohol Policy Guide for Nova Scotia Municipalities for this guide. The story relayed about Lloydminster in the section “Real Communities, Real Issues, Real Solutions” originally appeared in the Winter 2017 edition of Apple Magazine, written by Valerie Berenyi. This story was adapted with permission from Alberta Health Services. Copyright © 2020, Alberta Health Services. -
Annual Report Annual 2011
Annual Report 2011 www.altiacorporation.com 2 | 3 Altia annual report 2011 3 | 3 _Contents 04 32 Altia’s year Framework for sustainable 08 development CEO’s review 33 Framework and definition 10 of reporting Value in three 35 waves Financial 14 responsibility Never-ending passion 36 for brands Environmental WE THINK responsibility AHEAD 16 Brands are the core of 39 our growth IN Altia’s quality, safety GOOD and environmental COMPANY principles FAST TRACK 18 TO THE Selection of Altia’s MARKETS own brands 44 Social responsibility SHARING THE BEST 20 Fast track to the Nordic 49 MOMENTS and Baltic markets We follow responsible THIRST 22 business principles FOR Selection of Altia’s 51 GROWTH partner brands Comparing the report to the recommendation by Global 24 Reporting Initiative PASSION Industrial Services to customers 52 FOR Board of Directors BRANDS 26 Competitiveness through 54 BORN production, logistics and Executive Management sourcing Team RESPONSIBLE 30 56 Responsibility report Contact details 4 | 5 Altia annual report 2011 5 | 5 _ Leading in the Nordics and Baltics Altia is the leading wine and spirits company offering quality brands in the Nordic and Baltic countries. Altia produces, delivers, markets, sells, imports and exports alcoholic beverages in these markets. Altia’s own brands such as Blossa, Chill Out, Explorer, Renault, Grönstedts, Koskenkorva, Jaloviina, O.P. Anderson, Xanté and Key Ratios for Altia Group 2011 2010 2009 Skåne Akvavit have a strong market position and many of them a long heritage to cherish. Net sales, EUR million 524.8 487.9 407.3 Operating profit, EUR million 34.4 32.6 15.6 ( % of net sales ) 6.6 6.7 3.8 Altia’s partner brands represent both local and international Profit before taxes,EUR million 31.1 29.6 9.4 ( % of net sales) 5.9 6.1 2.3 brands from all over the world, such as Codorníu, Drostdy-Hof, Profit for the period, EUR million 21.3 25.7 5.3 Hardy’s, Jack Daniel’s, Bowmore, Nederburg, Ravenswood ( % of net sales) 4.1 5.3 1.3 Statement of financial position, and Robert Mondavi. -

The Economic and Social Consequences of Liquor Privatization in Western Canada
Impaired Judgement: The Economic and Social Consequences of Liquor Privatization in Western Canada by David Campanella and Greg Flanagan Impaired Judgement: The Economic and Social Consequences of Liquor Privatization in Western Canada About the Authors David Campanella is the Public Policy Research Manager for the Parkland Institute and is based in Calgary. David holds a Master’s degree from York University (MES), where he focused on political economy, and an undergraduate degree from the University of Waterloo (BES). Greg Flanagan is a public finance economist and has taught for 30 years in Alberta at various colleges and universi- ties. He retired from the University of Lethbridge in 2006. He holds degrees from University of Calgary (BA Economics), York University (MES Political Economy), and the University of British Columbia (MA Economics). His research interests focus on the economics of public policy. He served as a director on the board of Parkland Institute, Faculty of Arts, University of Alberta since its inception until 2011. As well as authoring numerous papers and articles, he is co-author of two textbooks: Economics in a Canadian Setting, HarperCollins Publishers, 1993, and Economics Issues, a Canadian Perspective, McGraw-Hill, 1997. About the Parkland Institute Parkland Institute is an Alberta research network that examines public policy issues. We are based in the Faculty of Arts at the University of Alberta and our research network includes members from most of Alberta’s academic institutions as well as other organizations involved in public policy research. Parkland Institute was founded in 1996 and its mandate is to: • conduct research on economic, social, cultural, and political issues facing Albertans and Canadians. -

Yhtiöittämisen Periaatteet Valtiolla
Valtiovarainministeriö Yhtiöittämisen periaatteet valtiolla Esiselvitys 30.1.2018 Valtionhallinnon kehittämisosasto 30.1.2018 SISÄLLYS JOHDANTO .............................................................................................................................................. 2 1 Valtion yhtiöt ja omistajapolitiikan periaatteet ................................................................................ 3 1.1 Valtion omistamisen perusta ......................................................................................................... 3 1.2 Omistajaohjaus .............................................................................................................................. 4 1.3 Valtion yhtiöt .................................................................................................................................. 6 2 Valtion liikelaitokset ..................................................................................................................... 10 2.1 Euroopan yhteisön päätös Tieliikelaitosta koskien ...................................................................... 10 2.2 Valtion liikelaitoksia koskeva lainsäädäntö .................................................................................. 12 3 Rahastot ...................................................................................................................................... 14 3.1 Valtion talousarvion ulkopuoliset rahastot ................................................................................... 14 3.2 Itsenäiset -

Alcohol Monopoly As an Idea and As a Reality: Some Perspectives from History1
(Published in Swedish in Alkoholpolitik: Tidskrift för nordisk alkoholforskning 2:1-6, 1985. The references have been updated.) ALCOHOL MONOPOLY AS AN IDEA AND AS A REALITY: SOME PERSPECTIVES FROM HISTORY1 Robin Room Alcohol Research Group 1816 Scenic Ave. Berkeley, California 94709 November, 1984 The idea that the state has an interest in the conditions of production and distribution of alcohol can be found in the earliest records of written legislation. The idea that the state should create a monopoly for itself or for a designated agent in some part of the production and distribution of alcohol also has a respectable antiquity (see, for instance, Österberg, 1985; Moskalewicz, 1985). But the idea of an alcohol monopoly motivated at least in part by public health and public order considerations seems to have come on the world stage first in the mid-19th century, in Scandinavia. In earlier times, the primary motivation for monopolization of commodities by local authorities or central governments had been the raising of revenues. With the central state often lacking the bureaucratic and police means to enforce an excise tax, the auctioning of monopoly rights in a commodity to the highest bidder became a common alternative across much of Europe. With tobacco, for instance, the leasing of a monopoly right in 1608 in Britain reflected James I's subordination of his strong feelings against tobacco to his needs for revenue (Austin 1978, p. 3). The strong and profitable private-monopoly system instituted by Venice in 1659 became a model for the rest of Europe, including the ancien regime in France (Austin 1978, pp. -

Saskatchewan’S Prohibition-Era Approach to Liquor Stores
POLICYP O L I C Y SERIESSFRONTIERE R I E CENTRES FOR PUBLIC POLICY FCPP POLICYFCPP SERIES POLICY NO. 70 SERIES • SEPTEMBER NO. 70 • SEPTEMBER 2009 2009 P OLICYS ERIES Ending Saskatchewan’s Prohibition-Era Approach to Liquor Stores By Dave Snow 1 © 20O9 ENDING SASKATCHEWAN’S PROHIBITION-ERA APPROACH TO LIQUOR STORES FRONTIER CENTRE ENDING SASKATCHEWAN’S PROHIBITION-ERA APPROACH TO LIQUOR STORES POLICY SERIES About the Author Dave Snow is a PhD student in the Department of Political Science at the University of Calgary, specializing in constitutional law and comparative politics. He received a BA from St. Thomas University in Fredericton, New Brunswick, and an MA from the University of Calgary. He is a graduate fellow at the Institute for Advanced Policy Research and has previously published a paper on affordable housing and homelessness with the Canada West Foundation. The Frontier Centre for Public Policy is an independent, non-profi t organization that undertakes research and education in support of economic growth and social outcomes that will enhance the quality of life in our communities. Through a variety of publications and public forums, the Centre explores policy innovations required to make the prairies region a winner in the open economy. It also provides new insights into solving important issues facing our cities, towns and provinces. These include improving the performance of public expenditures in important areas like local government, education, health and social policy. The author of this study has worked independently and the opinions expressed are therefore their own, and do not necessarily refl ect the opinions of the board of the Frontier Centre for Public Policy. -

This Document Has Been Downloaded from Tampub – the Institutional Repository of University of Tampere
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Trepo - Institutional Repository of Tampere University This document has been downloaded from TamPub – The Institutional Repository of University of Tampere Post-print The permanent address of the publication is http://urn.fi/URN:NBN:fi:uta-201405281513 Author(s): Kankaanpää, Jari; Oulasvirta, Lasse; Wacker, Jani Title: Steering and Monitoring Model of State-Owned Enterprises Year: 2014 Journal Title: International Journal of Public Administration Vol and number: 37 : 7 Pages: 409-423 ISSN: 0190-0692 Discipline: Business and management; Political science School /Other Unit: School of Management Item Type: Journal Article Language: en DOI: http://dx.doi.org/10.1080/01900692.2013.858355 URN: URN:NBN:fi:uta-201405281513 All material supplied via TamPub is protected by copyright and other intellectual property rights, and duplication or sale of all part of any of the repository collections is not permitted, except that material may be duplicated by you for your research use or educational purposes in electronic or print form. You must obtain permission for any other use. Electronic or print copies may not be offered, whether for sale or otherwise to anyone who is not an authorized user. Steering and Monitoring Model of State-Owned Enterprises Introduction Privatisation of stated-owned enterprises (SOEs) gained considerable momentum in developing and developed countries in the 1980s and 1990s (The World Bank, 2006, p. 3). Despite wide-ranging privatisation programmes, SOEs are still and will be an important part of many economies, especially in developing economies (La Porta, Lopez-de-Silanes, & Shleifer, 1999; Ezzamel, Wilmott, & Worthington, 2008; Vagliasindi, 2008; Ennser-Jedenastik, 2013). -

The Fiscal and Social Effects of State Alcohol Control Systems May 2013
The Fiscal and Social Effects of State Alcohol Control Systems May 2013 Roland Zullo Xi (Belinda) Bi Yu (Sean) Xiaohan Zehra Siddiqui Institute for Research on Labor, Employment, and the Economy University of Michigan 506 East Liberty Street, 3rd Floor Ann Arbor, MI 48104‐2210 734‐998‐0156 Please contact the lead author for inquiries at: [email protected] Acknowledgements: The authors of this report are grateful for the data and advice provided by Bill Ponicki at the Prevention Research Center at UC Berkeley and Adam Rogers at the Beverage Information Group. We also thank Mark Price, Stephen Herzenberg, Steve Schmidt and Jim Sgueo for constructive reviews of our research, David Hetrick for data management help and Jackie Murray for keen editorial assistance. This report was supported by a grant from the National Alcohol Beverage Control Association. Table of Contents Executive Summary i Section 1: Background 1 Section 2: Scope of Study 3 Section 3: Data and Measures 4 3.1 Alcohol Monopoly 4 3.2 Alcohol Consumption 8 3.3 Alcohol-Related State Income 9 3.4 Alcohol-Related Traffic Fatalities 14 3.5 Crime Rates 17 3.6 Advertising Regulations for Distilled Spirits 18 3.7 Prohibited Hours and Days of Sale 19 3.8 Penalties Related to Alcohol and Driving 21 Section 4: State Financial Trends and Histories 22 4.1 Utah 22 4.2 Pennsylvania 23 4.3 Mississippi 25 4.4 Virginia 26 4.5 Montana 28 4.6 Iowa 29 4.7 Maine 30 4.8 West Virginia 32 Section 5: Analysis 34 5.1 Alcohol Consumption 34 5.2 Alcohol-Related State Income 44 5.3 Alcohol-Related Traffic Fatalities 49 5.4 Crime Rates 56 Section 6: Summary 60 Bibliography 64 Appendix A: Estimating Equation 67 Appendix B: Data Sources 68 Appendix C: Variables, Statistics and Regression Results 72 Executive Summary The objective of this research is to examine, from the perspective of the state, the costs and benefits of state-owned alcohol distribution and sales systems.