Research Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Provider-Based Evaluation (Probe) 2014 Preliminary Report
The Provider-Based Evaluation (ProBE) 2014 Preliminary Report I. Background of ProBE 2014 The Provider-Based Evaluation (ProBE), continuation of the formerly known Malaysia Government Portals and Websites Assessment (MGPWA), has been concluded for the assessment year of 2014. As mandated by the Government of Malaysia via the Flagship Coordination Committee (FCC) Meeting chaired by the Secretary General of Malaysia, MDeC hereby announces the result of ProBE 2014. Effective Date and Implementation The assessment year for ProBE 2014 has commenced on the 1 st of July 2014 following the announcement of the criteria and its methodology to all agencies. A total of 1086 Government websites from twenty four Ministries and thirteen states were identified for assessment. Methodology In line with the continuous and heightened effort from the Government to enhance delivery of services to the citizens, significant advancements were introduced to the criteria and methodology of assessment for ProBE 2014 exercise. The year 2014 spearheaded the introduction and implementation of self-assessment methodology where all agencies were required to assess their own websites based on the prescribed ProBE criteria. The key features of the methodology are as follows: ● Agencies are required to conduct assessment of their respective websites throughout the year; ● Parents agencies played a vital role in monitoring as well as approving their agencies to be able to conduct the self-assessment; ● During the self-assessment process, each agency is required to record -

The Development of English Education in Kota Setar, 1909- 1957
International Journal of Academic Research in Business and Social Sciences Vol. 10, No. 9, 2020, E-ISSN: 2222 -6990 © 2020 HRMARS The Development of English Education in Kota Setar, 1909- 1957 Muhammad Qiwamuddin Alif Mahamad Najib, Khairi Ariffin To Link this Article: http://dx.doi.org/10.6007/IJARBSS/v10-i9/7981 DOI:10.6007/IJARBSS/v10-i9/7981 Received: 25 July 2020, Revised: 17 August 2020, Accepted: 30 August 2020 Published Online: 25 September 2020 In-Text Citation: (Najib, & Ariffin, 2020) To Cite this Article: Najib, M. Q. A. M., & Ariffin, K. (2020). The Development of English Education in Kota Setar, 1909-1957. International Journal of Academic Research in Business and Social Sciences. 10(9), 1011-1022. Copyright: © 2020 The Author(s) Published by Human Resource Management Academic Research Society (www.hrmars.com) This article is published under the Creative Commons Attribution (CC BY 4.0) license. Anyone may reproduce, distribute, translate and create derivative works of this article (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this license may be seen at: http://creativecommons.org/licences/by/4.0/legalcode Vol. 10, No. 9, 2020, Pg. 1011 - 1022 http://hrmars.com/index.php/pages/detail/IJARBSS JOURNAL HOMEPAGE Full Terms & Conditions of access and use can be found at http://hrmars.com/index.php/pages/detail/publication-ethics 1011 International Journal of Academic Research in Business and Social Sciences Vol. 10, No. 9, 2020, E-ISSN: 2222 -6990 © 2020 HRMARS The Development of English Education in Kota Setar, 1909-1957 Muhammad Qiwamuddin Alif Mahamad Najib, Khairi Ariffin Sultan Idris Education University, 35900 Tanjong Malim, Perak Abstract This research aims to study the development of English education in Kota Setar from 1909 to 1957. -

(CPRC), Disease Control Division, the State Health Departments and Rapid Assessment Team (RAT) Representative of the District Health Offices
‘Annex 26’ Contact Details of the National Crisis Preparedness & Response Centre (CPRC), Disease Control Division, the State Health Departments and Rapid Assessment Team (RAT) Representative of the District Health Offices National Crisis Preparedness and Response Centre (CPRC) Disease Control Division Ministry of Health Malaysia Level 6, Block E10, Complex E 62590 WP Putrajaya Fax No.: 03-8881 0400 / 0500 Telephone No. (Office Hours): 03-8881 0300 Telephone No. (After Office Hours): 013-6699 700 E-mail: [email protected] (Cc: [email protected] and [email protected]) NO. STATE 1. PERLIS The State CDC Officer Perlis State Health Department Lot 217, Mukim Utan Aji Jalan Raja Syed Alwi 01000 Kangar Perlis Telephone: +604-9773 346 Fax: +604-977 3345 E-mail: [email protected] RAT Representative of the Kangar District Health Office: Dr. Zulhizzam bin Haji Abdullah (Mobile: +6019-4441 070) 2. KEDAH The State CDC Officer Kedah State Health Department Simpang Kuala Jalan Kuala Kedah 05400 Alor Setar Kedah Telephone: +604-7741 170 Fax: +604-7742 381 E-mail: [email protected] RAT Representative of the Kota Setar District Health Office: Dr. Aishah bt. Jusoh (Mobile: +6013-4160 213) RAT Representative of the Kuala Muda District Health Office: Dr. Suziana bt. Redzuan (Mobile: +6012-4108 545) RAT Representative of the Kubang Pasu District Health Office: Dr. Azlina bt. Azlan (Mobile: +6013-5238 603) RAT Representative of the Kulim District Health Office: Dr. Sharifah Hildah Shahab (Mobile: +6019-4517 969) 71 RAT Representative of the Yan District Health Office: Dr. Syed Mustaffa Al-Junid bin Syed Harun (Mobile: +6017-6920881) RAT Representative of the Sik District Health Office: Dr. -

Infiltration Study for Urban Soil: Case Study of Sungai Kedah Ungauged Catchment
Journal of Environmental Science and Engineering B 3 (2014) 291-299 doi: 10.17265/2162-5263/2014.06.001 D DAVID PUBLISHING Infiltration Study for Urban Soil: Case Study of Sungai Kedah Ungauged Catchment Steven Poh Tze Wei and Khirluddin Bin Abdullah Department of Irrigation and Drainage, Division of Water Resources and Hydrology, Kuala Lumpur 68000, Malaysia Abstract: The DID (Department of Irrigation and Drainage) in Malaysia has produced a manual on urban stromwater management specifically for the Malaysia region with usage of infiltration method towards controlling the quantity and quality of surface runoff. With this method, the volume of surface runoff can be reduced and flood problems in major cities can be eliminated. The study areas of Sungai Kedah ungauged catchment are located at the northern region of Malaysia. The Kota Setar sub-catchment is located at the downstream of Sungai Kedah with the newly completed development of control barrage at the upper Kota Setar. This paper will describe the analyses of the infiltration curves at Kota Setar. The resulting infiltration maps have developed based on the infiltration capacities. Key words: Sungai Kedah ungauged catchment, type of soil, infiltration curve, infiltration map. 1. Introduction 2. Study Area Undeveloped land has a little surface runoff, due to The study area, Sungai Kedah catchment, is located most precipitation infiltrate into the topsoil and the at the northern region of Malaysia as shown in Fig. 2. occurrence of hydraulic conductivity flow through as The nonlinear rainfall-runoff model [2] has been interflow into stream [1]. As a result of this process, applied to the Sungai Kedah catchment, which is located the precipitation effects are averaged out over a long in the northern region of Malaysia. -

Stoneflies (Insecta: Plecoptera) in Malaysian Tropical Rivers: Diversity and Seasonality
Journal of Entomology and Nematology Vol. 3(2), pp. 030-036, February 2011 Available online at http://www.academicjournals.org/jen ISSN 2006- 9855 ©2011 Academic Journals Full Length Research Paper Stoneflies (Insecta: Plecoptera) in Malaysian tropical rivers: Diversity and seasonality Suhaila Abdul Hamid* and Che Salmah Md. Rawi School of Biological Sciences, Universiti Sains Malaysia. 11800 Minden, Penang, Malaysia. Accepted 23 December, 2010 Adult stoneflies (Plecoptera) were light-trapped monthl from January to December 2008 in Tupah River, Kedah, Malaysia. Two families of Plecoptera, Perlidae and Nemouridae were represented with nine species. More Plecoptera was collected in the wet seasons especially for the family Nemouridae. Neoperla asperata was a common species that occurred throughout the year. Neoperla fallax was equally common but this species was absent during early part of the year. The percentage of females was higher than male for all species of Plecoptera collected. Key words: Upstream river, Plecoptera, season, sex ratio, peninsular Malaysia. INTRODUCTION Plecoptera are primitive group of insects also known as valued and plentiful food source for bats and birds that stoneflies or salmonflies. The diversity of Plecoptera feed at dusk on flying insects (Fochetti and Tierno de declines rapidly from temperate Asian latitudes (nine Figueroa 2008). Moreover, according to Sweeney (1993), families) to tropical latitudes (four or fewer families). The mammals such as shrews and raccoons also eat on only diverse stonefly family in the Malaysian region is the Plecoptera nymphs as well as emerging adults. Perlidae. Comparative to their temperate counterparts, Aquatic insect emergence is strongly influenced by tropical stoneflies are incompletely understood (Sheldon season. -

Laporan Pasaran Harta Separuh Pertama
LAPORAN PASARAN HARTA SEPARUH PERTAMA PROPERTY MARKET REPORT FIRST HALF 2006 Kandungan LAPORAN Contents PASARAN HARTA SEPARUH PERTAMA 2006 PROPERTY MARKET REPORT FIRST HALF 2006 i JABATAN PENILAIAN DAN PERKHIDMATAN HARTA KEMENTERIAN KEWANGAN MALAYSIA VALUATION AND PROPERTY SERVICES DEPARTMENT MINISTRY OF FINANCE MALAYSIA HARGA: RM75.00 ii Jabatan Penilaian dan Perkhidmatan Harta Valuation and Property Services Department Kementerian Kewangan Malaysia Ministry Of Finance Malaysia C Hak Cipta Terpelihara 2006 C Copyrights Reserved 2006 (ISSN 1675 - 2686) (ISSN 1675 - 2686) Naskhah jualan boleh didapati daripada: Sales copies are obtained from: (i) Ketua Pengarah (i) Director General Jabatan Penilaian dan Perkhidmatan Harta Valuation and Property Services Department Aras 3, Blok Selatan Presint 2 Level 3, Southern Block, Precint 2 Pusat Pentadbiran Putrajaya Pusat Pentadbiran Putrajaya 62592 Putrajaya 62592 Putrajaya Telefon : 03 - 8882 4600 Telefon : 03 - 8882 4600 Telefaks : 03 - 8882 4601 Telefaks : 03 - 8882 4601 e-mail : [email protected] e-mail : [email protected] (ii) Pusat Maklumat Harta Tanah Negara (NAPIC) (ii) National Property Information Centre (NAPIC) Jabatan Penilaian dan Perkhidmatan Harta Valuation and Property Services Department Aras 4, Blok Selatan Presint 2 Level 4, Southern Block, Precint 2 Pusat Pentadbiran Putrajaya Pusat Pentadbiran Putrajaya 62592 Putrajaya 62592 Putrajaya Telefon : 03 - 8882 4600 Telefon : 03 - 8882 4600 Telefaks : 03 - 8882 4609 Telefaks : 03 - 8882 4609 e-mail : [email protected] e-mail : [email protected] (iii) Cawangan-cawangan Jabatan (iii) Branch offices of The Valuation and Penilaian dan Perkhidmatan Harta Property Services Department Atur huruf dan kerja seni oleh: Typesetting and artwork by: Pusat Maklumat Harta Tanah Negara (NAPIC) National Property Information Centre (NAPIC) KANDUNGAN CONTENTS GAMBARAN KESELURUHAN PASARAN HARTA DI MALAYSIA BAGI SEPARUH TAHUN 2006 ...................................... -

Household Expenditure 2019 Kedah
MALAYSIA LAPORAN SURVEI PERBELANJAAN ISI RUMAH MENGIKUT NEGERI DAN DAERAH PENTADBIRAN HOUSEHOLD EXPENDITURE SURVEY REPORT BY STATE AND ADMINISTRATIVE DISTRICT KEDAH 2019 Pemakluman/Announcement: Kerajaan Malaysia telah mengisytiharkan Hari Statistik Negara (MyStats Day) pada 20 Oktober setiap tahun. Tema sambutan MyStats Day 2020 adalah “Connecting The World With Data We Can Trust”. The Government of Malaysia has declared National Statistics Day (MyStats Day) on 20th October each year. MyStats Day 2020 theme is “Connecting The World With Data We Can Trust”. JABATAN PERANGKAAN MALAYSIA DEPARTMENT OF STATISTICS, MALAYSIA Diterbitkan dan dicetak oleh/Published and printed by: Jabatan Perangkaan Malaysia Department of Statistics, Malaysia Blok C6, Kompleks C, Pusat Pentadbiran Kerajaan Persekutuan, 62514 Putrajaya, MALAYSIA Tel. : 03-8885 7000 Faks : 03-8888 9248 Portal : https://www.dosm.gov.my Facebook / Twitter / Instagram : StatsMalaysia Emel / Email : [email protected] (pertanyaan umum/general enquiries) [email protected] (pertanyaan & permintaan data/ data request & enquiries) Harga / Price : RM30.00 Diterbitkan pada Julai 2020/Published on July 2020 Hakcipta terpelihara/All rights reserved. Tiada bahagian daripada terbitan ini boleh diterbitkan semula, disimpan untuk pengeluaran atau ditukar dalam apa-apa bentuk atau alat apa jua pun kecuali setelah mendapat kebenaran daripada Jabatan Perangkaan Malaysia. Pengguna yang mengeluarkan sebarang maklumat dari terbitan ini sama ada yang asal atau diolah semula hendaklah meletakkan kenyataan -

Annual Report 2019 Annual R Epo T 2019 Commission of M Alaysia Human Rig H Ts
HUMAN RIGHTS COMMISSION OF MALAYSIA ANNUAL REPORT 2019 ANNUAL ANNUAL R EPO R T 2019 COMMISSION OF HUMAN RIG H TS HUMAN RIGHTS COMMISSION OF MALAYSIA M SUHAKAM ALAYSIA Level 11, Menara TH Perdana, 1001, Jalan Sultan Ismail, 50250 Kuala Lumpur. URL: http://www.suhakam.org.my HUMAN RIGHTS COMMISSION OF MALAYSIA ANNUAL REPORT 2019 FIRST PRINTING, 2020 Copyright Human Rights Commission of Malaysia (SUHAKAM) The copyright of this report belongs to the Commission. All or any part of this report may be reproduced provided acknowledgment of source is made or with the Commission’s permission. The Commission assumes no responsibility, warranty and liability, expressed or implied by the reproduction of this publication done without the Commission’s permission. Notification of such use is required. All rights reserved. Published in Malaysia by HUMAN RIGHTS COMMISSION OF MALAYSIA (SUHAKAM) 11th Floor, Menara TH Perdana 1001 Jalan Sultan Ismail 50250 Kuala Lumpur E-mail: [email protected] URL : http://www.suhakam.org.my Printed in Malaysia by Mihas Grafik Sdn Bhd No. 9, Jalan SR 4/19 Taman Serdang Raya 43300 Seri Kembangan Selangor Darul Ehsan National Library of Malaysia Cataloguing-in-Publication Data ISSN: 1511 - 9521 MEMBERS OF THE COMMISSION 2019 From left: Prof. Dato’ Noor Aziah Mohd. Awal (Children’s Commissioner), Dato’ Seri Mohd Hishamudin Md Yunus, Datuk Godfrey Gregory Joitol, Mr. Jerald Joseph, Tan Sri Othman Hashim (Chairman), Dato’ Mah Weng Kwai, Datuk Lok Yim Pheng, Dr. Madeline Berma and Associate Prof. Dr. Nik Salida Suhaila -

Unable to Take Pollution in Sg Petani, Green Activist Moves to Penang
8/2/2021 Unable to take pollution in Sg Petani, green activist moves to Penang | Free Malaysia Today (FMT) Unable to take pollution in Sg Petani, green activist moves to Penang By Predeep Nambiar - July 29, 2021 10:55 PM 186 135 22 23 Shares A Department of Environment officer based in Sungai Petani claims the pollution was mainly caused by wood-based factories which had open furnaces. (Freepik pic) GEORGE TOWN: An activist who fought against poor air quality due to open burning by illegal recycling factories in Sungai Petani has revealed that she moved out of Kedah due to such pollution. Having spent most of her life in the northern state, Persatuan Tindakan Alam Sekitar (PTAS) Sungai Petani’s Lydia Ong, 56, said her health was affected by the open burning, which continued unabated despite three years of campaigning by her group. She said she moved back to Penang six months ago after the acrid smell of burnt plastic became worse during the movement control order (MCO), and had even endangered her life because she was already suffering from breathing problems. At a forum organised by C4 Center today on imported waste, Ong said Kedah remained home to “hundreds” of illegal recycling factories burning non-recyclable waste in the wee hours of the morning despite repeated claims by the state that it would crack down on such operations. She added that with Covid-19 ravaging the Kuala Muda district, where Sungai Petani is located, the factories operated with impunity. She cited a wood products factory, branded illegal by the https://www.freemalaysiatoday.com/category/nation/2021/07/29/unable-to-take-pollution-in-sg-petani-green-activist-moves-to-penang/ 1/3 8/2/2021 Unable to take pollution in Sg Petani, green activist moves to Penang | Free Malaysia Today (FMT) authorities before, spewing black smoke next to a hypermarket in town “24 hours, seven days a week”. -

Urban Design Elements with a Case Study at Bandar Sungai Petani of Kedah
©2021 International Transaction Journal of Engineering, Management, & Applied Sciences & Technologies ISSN 2228-9860 eISSN 1906-9642 CODEN: ITJEA8 International Transaction Journal of Engineering, Management, & Applied Sciences & Technologies http://TuEngr.com Urban Design Elements with a Case Study at Bandar Sungai Petani of Kedah Aida Amalina Abd Rahim1, Mohamad Azil Muzammil Baharudin1, Yasser Arab1*, Ahmad Sanusi Hassan1, Khiensak Seangklieng2, Boonsap Witchayangkoon3 1 School of Housing, Building & Planning, Universiti Sains Malaysia, MALAYSIA. 2 Faculty of Architecture and Planning, Thammasat University, THAILAND. 3 Department of Civil Engineering, Thammasat School of Engineering, Thammasat University, THAILAND. *Corresponding Author (Tel: +60-142426181, Email: [email protected]). Paper ID: 12A3B Abstract Volume 12 Issue 3 This study focuses on the early development of Bandar Sungai Petani Received 01 October 2020 during the early 1990s and the impact of the colonization, resulting in Received in revised form 19 a variety of physical design and configuration that can encourage social December 2020 fabrics and economy. This study’s goal is to justify the identity, history of the Accepted 04 January 2021 early settlement of Bandar Sungai Petani during the early year and the Available online 06 January progress of development of urban design influence of typography, lifestyle of 2021 the habitants, economic capacity that made the area one of the major towns Keywords: in Peninsular Malaysia. Sungai Petani is known as an industrial town due to Colonial architecture; City development; its economic activity. This research method involves observation and data Mental mapping; collection.. The study finds that Bandar Sungai Petani has a masterplan with Commercial area; gridiron design, which is systematically arranged although irregularly. -

Original Article Factors Associated with Thalassaemia Carrier Among Form Four Students in Kedah, Malaysia
Malaysian Journal of Public Health Medicine 2021, Vol. 21 (1): 134-140 ORIGINAL ARTICLE FACTORS ASSOCIATED WITH THALASSAEMIA CARRIER AMONG FORM FOUR STUDENTS IN KEDAH, MALAYSIA Rosidah Omar1, Norizan Ahmad1 and Ngee Wen Sze1 1 Family Health Unit, Kedah State Health Department, Ministry of Health Malaysia, Simpang Kuala, Jalan Kuala Kedah, 05400 Alor Setar, Kedah, Malaysia Corresponding author: Rosidah Omar Email: [email protected] ABSTRACT Thalassaemia and abnormal haemoglobins are the most common genetic disorder worldwide. School-based screening thalassaemia program for form four students was introduced with the objective to screen for the thalassaemia status. There is paucity in the data in Kedah on distribution of thalassaemia carrier and the associated factors. Hence this study aims to identify the factors associated with being a thalassaemia carrier and to describe the laboratory cost for the thalassaemia screening. This study used secondary data from the school-based thalassaemia screening in 2018 obtained from Kedah State Health Department. Results showed the prevalence of thalassaemia carrier among form four students in Kedah was 10.91%. Multivariate logistic regression showed that students from Baling, Padang Terap and Yan were 1.40, 1.34 and 1.23 times more likely to be a thalassaemia carrier respectively compared to Kota Setar (aOR Baling 1.40;95% CI 1.21,1.64; aOR Padang Terap 1.34;95% CI 1.11,1.61 and aOR Yan 1.23;95% CI 1.03,1.47). Malay and Siamese students were five times more likely be thalassaemia carriers compared to Indian (aOR Malay 5.16;95%CI 3.42,7.79, aOR Siamese 5.63;95%CI 3.19,9.97). -
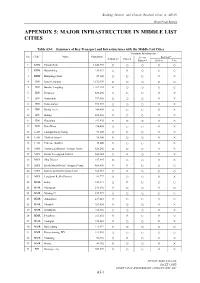
03 CN18 PR Appendix 5 Infras
Building Disaster and Climate Resilient Cities in ASEAN Draft Final Report APPENDIX 5: MAJOR INFRASTRUCTURE IN MIDDLE LIST CITIES Table A5-1 Summary of Key Transport and Infrastructures with the Middle List Cities Transport Infrastructure *1 No. Code Name Population Access Railway*5 Airport*2 Port*3 Road*4 Station Line 1 KHM Phnom Pénh 1,242,992 ○ ○ ○ ○ ○ 2 KHM Băttâmbâng 140,533 ○ × ○ ○ ○ 3 KHM Kâmpóng Cham 47,300 ○ ○ ○ × × 4 IDN Kota Semarang 1,672,999 ○ ○ ○ ○ ○ 5 IDN Bandar Lampung 1,167,101 × ○ ○ ○ ○ 6 IDN Denpasar 880,600 ○ ○ ○ × × 7 IDN Samarinda 797,006 ○ ○ ○ × × 8 IDN Kota Ambon 395,423 ○ ○ ○ × × 9 IDN Banda Aceh 249,499 ○ ○ ○ × × 10 IDN Bitung 202,204 × ○ ○ × × 11 IDN Gorontalo 197,970 × ○ ○ × × 12 IDN Kota Bima 156,400 ○ ○ ○ × × 13 LAO Luangprabang (luang) 90,300 ○ ○ ○ × × 14 LAO Thalhek (kham) 90,800 × ○ ○ × × 15 LAO Pakxane (bolikh) 45,000 × ○ ○ × × 16 MYS Timur Laut District (George Town) 520,242 ○ ○ ○ × × 17 MYS Kuala Terengganu District 343,284 ○ × ○ × × 18 MYS Sibu District 247,995 ○ ○ ○ × × 19 MYS Kuala Muda District (Sungai Petani) 456,605 × × ○ ○ ○ 20 MYS Kota Setar District (Alor Setar) 366,787 ○ × ○ ○ ○ 21 MYS Langkawi Kedha District 94,777 ○ ○ ○ × × 22 MMR Kalay 348,573 ○ × ○ ○ ○ 23 MMR Myingyan 276,096 × ○ ○ × ○ 24 MMR Nyaung-U 239,947 ○ ○ ○ ○ ○ 25 MMR Amarapura 237,618 ○ ○ ○ ○ ○ 26 MMR Mrauk-U 189,630 × ○ ○ × × 27 MMR Kyaukpyu 165,352 ○ ○ ○ × × 28 MMR Pwintbyu 163,692 × × ○ × ○ 29 MMR Toungup 158,341 × ○ ○ × × 30 MMR Rathedaung 111,974 × ○ ○ ○ ○ 31 MMR Kyimyindaing-WY 111,514 ○ ○ ○ ○ ○ 32 MMR Manaung 56,966 ○ × ○ × × 33 MMR Hakha 48,352 × ○ ○ × × 34 PHL Batangas city 305,607 × ○ ○ × × NIPPON KOEI CO.,LTD. PAC ET C ORP.